
Abstract
Introduction
The syndrome of transient headache and neurological deficits with cerebrospinal fluid lymphocytosis (HaNDL) is a diagnosis made by exclusion. In the literature, different etiological explanations are proposed for HaNDL, including an immune-mediated reaction after a viral infection.
Case description
We present a case of a 23-year-old woman with several episodes of transient headache, neurological deficits and cerebrospinal fluid lymphocytosis. All diagnostic criteria for the HaNDL syndrome were fulfilled; however, additional cerebrospinal fluid analysis showed a positive polymerase chain reaction (PCR) for human herpes virus type 7 (HHV-7).
Discussion
The possible role of a (prodromal) viral infection in the etiology of HaNDL is discussed. Also the role of electroencephalography (EEG) recordings is discussed. Serial EEG recordings showed generalized slowing, frontal intermittent rhythmic delta activity (FIRDA) and symmetric triphasic frontal waves with a dilation lag.
Keywords
Introduction
The syndrome of transient headache and neurological deficits with cerebrospinal fluid (CSF) lymphocytosis (HaNDL) (1) is also known as migrainous syndrome with CSF pleocytosis (2) or as pseudomigraine with lymphocytic pleocytosis and transient neurological deficits (PMP syndrome) (3). The syndrome has been classified as a secondary headache attributed to a non-vascular intracranial disorder, according to the third edition of the International Classification of Headache Disorders (ICHD-III). HaNDL is characterized by episodes of moderate to severe headache, lasting for hours and accompanied by or presently followed by transient neurological deficits with CSF pleocytosis with a lymphocytic predominance. The diagnosis of HaNDL is made by exclusion. The episodes of HaNDL symptoms tend to recur over periods of less than three months and the patients should be asymptomatic between the episodes (4). Some patients report symptoms of preceding viral infection or fever. HaNDL is usually seen during the third and fourth decade of life and is a benign, self-limiting disorder (3). However, cases in childhood have been described (5). The minority of the described adult patients had a history or a family history of migraine (1,3). To fulfill the criteria, the results of neuroimaging tests must be normal. In this case report, the possible role of a (prodromal) viral infection in the etiology of HaNDL is discussed. Also, serial electroencephalography (EEG) recordings and their possible role in diagnosing HaNDL are described.
Case report
A 23-year-old right-handed woman presented at the emergency department with a few days’ severe headache, nausea and vomiting, and a few hours’ right-sided numbness and weakness. There was no relevant medical or family history and the patient did not take medication. The neurological examination showed an expressive aphasia and a right-sided hemiparesis graded as 4/5 using the Medical Research Council (MRC)-grading system. Neck stiffness and fever were absent. She had experienced two episodes of severe headache, nausea, vomiting and left-sided numbness lasting for half an hour to several hours five and six days prior to the visit to the emergency department. The patient had recently started a job working with young children.
Routine blood tests did not show any abnormalities. Brain computed tomography (CT) on the day of admission was normal. The CSF opening pressure was 32 cm H2O. CSF analysis showed lymphocytic (98%) pleocytosis, with a white cell count of 220 × 106/l, protein level of 1.43 g/l, glucose level of 2.9 mmol/l, and lactate acid of 2.0 mmol/l.
The first recorded EEG (on the day of admission) showed an asymmetrical background rhythm of 8.5 to 9.0 Hz on the right hemisphere with an average amplitude of 25 to 50 microvolts (μV), and with depression of the physiological background rhythm on the left hemisphere, which correlated with the patient’s symptoms. However, relatively symmetrical paroxysms of frontal intermittent rhythmic delta activity (FIRDA) were frequently seen, with an average amplitude of 50 to 75 μV. Also symmetrical isolated delta waves with a frontal maximum and triphasic configuration with typical antero-posterior time lag and an average amplitude of 50 to 150 µV were present (Figure 1). We concluded that the EEG was suspect for a diffuse encephalopathy without signs suggestive of epileptic disturbances.
We refer to the text for description of the electroencephalography (EEG). High-pass filter 0.100 Hz; low-pass filter 60 Hz; notch-filtered; bipolar montage; sensitivity 7 µV/mm; speed 30 mm/s.
The patient was admitted to the neurology ward with the tentative diagnosis of a viral encephalitis and was treated with intravenous acyclovir (10 mg/kg intravenous three times daily (tid)). Magnetic resonance imaging (MRI), including diffusion-weighted imaging (DWI), performed four days after admission showed no abnormalities. Polymerase chain reaction (PCR) of the CSF was negative for herpes simplex virus, varicella zoster virus, Epstein-Barr virus, cytomegalovirus, enterovirus, mycoplasma, parechovirus and human herpes virus-6 (HHV-6), but positive for human herpes virus-7 (HHV-7). Subsequent serological tests were negative for treponema pallidum, human immunodeficiency virus (HIV) and borrelia burgdorferi.
The patient recovered completely, but experienced a new episode of severe headache, expressive aphasia, confused behavior and right-sided numbness seven days after admission. The lumbar puncture was repeated and showed a CSF opening pressure of 28 cm H2O, persistent lymphocytic (98%) pleocytosis of 452 × 106/l, a protein level of 1.78 g/l, glucose level of 2.8 mmol/l and lactate acid level of 2.1 mmol/l. Oligoclonal bands were not detected in the CSF or serum. PCR of the CSF again was positive for HHV-7. Additional serological tests for paraneoplastic antibodies were negative. The HHV-6 and -7 serum immunoglobulin (Ig)G-titers were significantly increased compared to those determined in a serum sample from two years earlier (this serum was acquired for other serology and stored frozen at the microbiological laboratory). The serological profile in combination with the positive HHV-7 PCR on CSF was considered suggestive of a primary HHV-7 infection. (This serology is not routine diagnostics and was performed in the United Kingdom. There is insufficient evidence that HHV-7 IgM is a reliable test.) The intravenous acyclovir was stopped after the second negative CSF PCR for herpes simplex. The second EEG (performed seven days after admission) again showed an asymmetrical background rhythm of 8.0 to 8.5 Hz and an average amplitude of 25 to 50 µV in favor of the right hemisphere. FIRDA and symmetric isolated delta waves with a triphasic appearance and frontal maximum were also seen again (Figure 2). When she had almost completely recovered one day later, the third recorded EEG (performed eight days after admission) showed a background rhythm with a frequency of 9.0 to 9.5 Hz and an average amplitude of 25 to 50 µV. FIRDA was absent and only sporadically isolated runs of delta waves were seen with a frequency of 1.0 Hz, an amplitude of 75 to 100 µV with a frontal maximum; furthermore, a triphasic appearance, with the same time lag as described before, persisted (Figure 3). She made a complete recovery and was discharged 10 days after admission, with the clinical diagnosis of HaNDL.
We refer to the text for description of the electroencephalography (EEG). High-pass filter 0.100 Hz; low-pass filter 60 Hz; notch-filtered; bipolar montage; sensitivity 7 µV/mm; speed 30 mm/s. We refer to the text for description of the electroencephalography (EEG). High-pass filter 0.100 Hz; low-pass filter 60 Hz; notch-filtered; bipolar montage; sensitivity 7 µV/mm; speed 30 mm/s.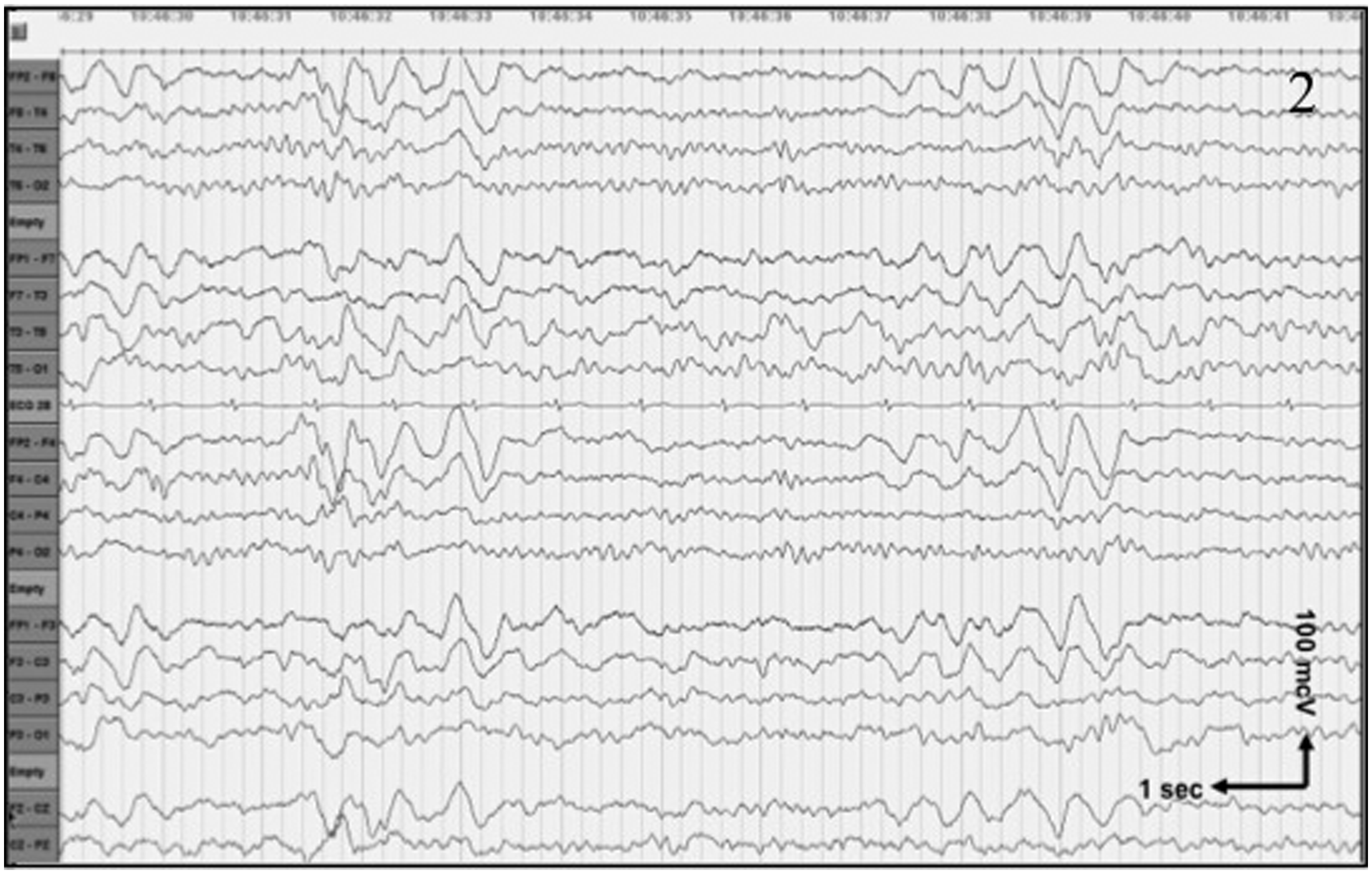

Four days later, she presented at the emergency department after another five episodes of headache, nausea, vomiting and right-sided numbness, as described earlier. The MRI-DWI of the brain was repeated and again it did not show any abnormalities. The fourth EEG (performed 15 days after the first admission) showed prolonged runs of FIRDA with an average amplitude of 75 to 150 µV in combination with a mixed asymmetrical occipital background rhythm of 5.5 to 6.0 Hz in favor of the right hemisphere with depression of the background rhythm on the left hemisphere (Figure 4). She was treated with intravenous methylprednisolone 1000 mg once daily for five days. She was discharged from the hospital and again made a full recovery. In the follow-up period over subsequent months, one relapse of severe headache, nausea, vomiting and left-sided numbness occurred. An EEG recorded nine months after the first admission showed a normal symmetrical occipital background rhythm of 9.0 to 9.5 Hz with an average amplitude of 25 to 50 µV. The runs of FIRDA and triphasic waves had vanished completely. One year later, she had no complaints and did not show any clinical evidence of recurrence of the HaNDL symptomatology.
We refer to the text for description of the electroencephalography (EEG). High-pass filter 0.100 Hz; low-pass filter 60 Hz; notch-filtered; bipolar montage; sensitivity 7 µV/mm; speed 30 mm/s.
Discussion
Our patient fulfilled all diagnostic criteria for the syndrome of HaNDL. The meaning of the HHV-7 PCR on CSF will be discussed here. In the literature, three etiological explanations are proposed for HaNDL: (I) a migraine with aura variant, (II) it develops secondarily to an infectious meningoencephalitis, or (III) it is the result of an autoimmune disease (6). It is suggested that HaNDL could be the result of an immune-mediated reaction after a viral infection (1,3,7). The hypothesis is that a viral infection triggers the activation of the immune system, secondarily inducing transient neurological symptoms by a spreading, depression-like mechanism and aseptic vasculitis (6). Approximately 25% to 50% of patients have symptoms of a viral illness or fever up to three weeks before the onset of neurological symptoms (1,3,6). In the study by Gómez-Aranda et al. (3), no evidence was found of a viral infection. HaNDL was once associated with a recent human herpes virus-6 (HHV-6) infection (7) with positive serology. In our patient, the HHV-7 PCR of CSF was positive and HHV-6 and -7 IgG were increased, suggestive of a recent HHV-7 infection. Previous data suggest that delayed primary HHV-7 infection can cause neurologic disease (8). The patient described here had recently started working with young children. If indeed she had not been infected with HHV-7 during childhood, the exposure to HHV-7 at work could explain the occurrence of a primary infection. Primary HHV-7 infection has been associated with exanthema subitum (ES) and the association with neurologic disease was provided by case reports of children with ES and encephalopathy (9), facial nerve palsy (10), and hemiplegia with febrile seizures (11,12). Also, aseptic meningitis has been associated with HHV-7 infection (13). Pohl-Koppe et al. (14) also found positive HHV-7 PCR in the CSF of children with aseptic meningitis, viral encephalitis, acute disseminated encephalomyelitis (ADEM), facial nerve palsy, vestibular neuritis and febrile seizure in the absence of ES.
We found a correlation between the patient’s symptoms and EEG abnormalities. In patients with the HaNDL syndrome, EEG abnormalities are scarcely reported in literature. Berg and Williams (1) described six patients, four of whom had at least one abnormal EEG. When combining these results with the reported patients in the literature, the authors found an abnormal EEG in 72% of cases (1). Bartleson et al. (2) found abnormal EEGs in five out of seven patients that showed focal and generalized abnormalities. Gómez-Aranda et al. (3) reported on 42 patients in whom the EEG was abnormal in 71% of the cases. Unilateral excessive slowing was found in 62% and bilateral slowing was found in 10% of the cases. After the symptomatic period, the EEG became normal in the tested patients (3,7). To our knowledge, the findings of detailed serial follow-up EEG examinations, as in our patient, were not previously described in the literature. Moreover, recurrences of the clinical symptoms of the HaNDL syndrome in our patient correlated with the EEG findings.
In conclusion, at the moment there is no definitive proof that HHV-7 infection is associated with HaNDL. The possible role of a (prodromal) HHV-7 infection in the etiology of HaNDL is discussed. Serial EEG studies showed that clinical symptoms of HaNDL correlated with the asymmetrical generalized slowing of the EEG, FIRDA, and frontal triphasic waves with a dilation lag, which have not been reported previously in the literature. The EEG changes in combination with the symptoms could raise the clinical suspicion of HaNDL in patients with new-onset headache and fluctuating neurological symptoms; however, one should be aware that the EEG abnormalities as described above are non-specific.
Clinical implications
In patients with new-onset headache and fluctuating neurological symptoms, asymmetrical generalized slowing of the electroencephalography (EEG), frontal intermittent rhythmic delta activity (FIRDA), and frontal triphasic waves could raise the clinical suspicion of headache and neurological deficits with cerebrospinal fluid lymphocytosis (HaNDL). However, one should be aware that the EEG abnormalities are non-specific.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.