
Abstract
Aim
The aim of this study was to examine the prevalence of household food insecurity in individuals reporting migraine within a large population-based sample of Canadians.
Methods
The Canadian Community Health Survey (CCHS) uses a stratified cluster sample design to obtain information on Canadians ≥12 years of age. Data on household food insecurity were assessed for individuals who reported having migraine or not, providing a current point prevalence. This was assessed for stability in two CCHS datasets from four and eight years earlier. Factors associated with food insecurity among those reporting migraine were examined and a logistic regression model of food insecurity was developed. We also examined whether food insecurity was associated with other reported chronic health conditions.
Results
Of 48,645 eligible survey respondents, 4614 reported having migraine (weighted point prevalence 10.2%). Food insecurity was reported by 14.8% who reported migraine compared with 6.8% of those not reporting migraine, giving an odds ratio of 2.4 (95% confidence interval 2.0–2.8%). This risk estimate was stable over the previous eight years. The higher risk for food insecurity was not unique to migraine and was seen with some, but not all, chronic health conditions reported in the CCHS.
Conclusions
Food insecurity is more frequent among individuals reporting migraine in Canada.
Introduction
Food insecurity and obesity are the most significant food-related public health issues. There has been less awareness of food insecurity, which is defined as limited or intermittent access to nutritionally adequate, safe and acceptable foods, accessed in socially acceptable ways (1). Approximately 30% of Canadians in low-income households are food insecure (2) and almost 13% of Canadian households experienced some level of food insecurity in 2012 (3). Food-insecure households are more likely to include children with acute infections, chronic illness, and both developmental and mental health problems (4,5) and adults who experience stress, depression, and anxiety (6). People with threatened food security are more likely to omit or reduce the size of meals, to have less variety in their diets, and to eat less fruit, vegetables, dairy products, and vitamins (7). Food insecurity is associated with numerous health issues, including hyperlipidemia, hypertension, and obesity (8).
Migraine affects approximately one in six individuals (9) and its prevalence is inversely related to household income (10). We hypothesized an association between migraine and food insecurity within a Canadian population-based health survey.
The objectives of this study were to:
examine whether individuals reporting migraine are more likely to report household food insecurity; determine whether this association is stable; explore which factors are associated with reported household food insecurity within the population of individuals reporting migraine; determine whether reported migraine continues to be associated with food insecurity within a parameterized model of food insecurity for the entire population (migraine and freedom from reported migraine); and whether this effect is unique to reported migraine or is seen within other health conditions.
Methods
The Canadian Community Health Survey (CCHS) is a cross-sectional survey that collects information related to health status, health care utilization, and health determinants for the Canadian population. A stratified cluster sample design is used to obtain information on Canadians ≥12 years of age living in private dwellings in the ten provinces and three territories, exclusive of people living on First Nations Reserves or Crown lands, residents of institutions, full-time members of the Canadian Armed Forces, and residents of certain remote regions. Information was collected every two years until 2007 and annually since then (11). The response rate for the most recent iteration of the survey (2013) was 76.6% at the household level and 66.7% at the person level (12).
Our analysis was primarily based on the 2013 CCHS (data collection January–December 2013), but also made use of the 2009 and 2005 datasets to examine the prevalence of food security over time. Within these surveys there are common question sequences addressed to all respondents and sections that are addressed to specific subpopulations, generally to residents of specific provinces or health districts. All respondents were given the question: “I’d like to ask about certain chronic health conditions which you may have. We are interested in ‘long-term conditions’ which are expected to last or have already lasted 6 months or more and that have been diagnosed by a health professional. Do you have migraine headaches?” (13). Household food insecurity was subsequently assessed using the Canadian Food Security Status Module (14), which was adopted from the US model of food security status published by the US Department of Agriculture in 2000 (15). A summative assessment of household food security was derived from 18 questions indicating whether household members were able to afford the food they needed in the previous 12 months. The questions ranged in severity from worrying about running out of food, through the unavailability of nutritious food, to children within the household not eating for the whole day. Ten of the 18 questions were specific to the experiences of adults within the household or the household in general, while the remaining eight were specific to the experiences of children in the household (16). The module yielded a score based on which households could be classified as food secure, moderately food insecure and having severe food insecurity. For this study, we collapsed the two food insecurity classifications to give a binary scale: food secure or food insecure.
Eligible respondents were ≥12 years of age and resided in the Canadian provinces and territories, with the exception of British Columbia, Manitoba, Newfoundland and Labrador, and Yukon Territory, which did not participate in the food security question in 2013 (78.5% of all survey respondents). Our analysis was limited to individuals with non-missing responses for reported migraine (99.9% of all survey respondents) and household food security (96.4% of all survey respondents).
The primary analysis was to describe the prevalence of food security within the population of people reporting migraine compared with the population not reporting migraine. We assessed whether the prevalence of food insecurity remained stable by examining prevalence in four-year intervals culminating with the current dataset.
Factors assessed for association with food insecurity.
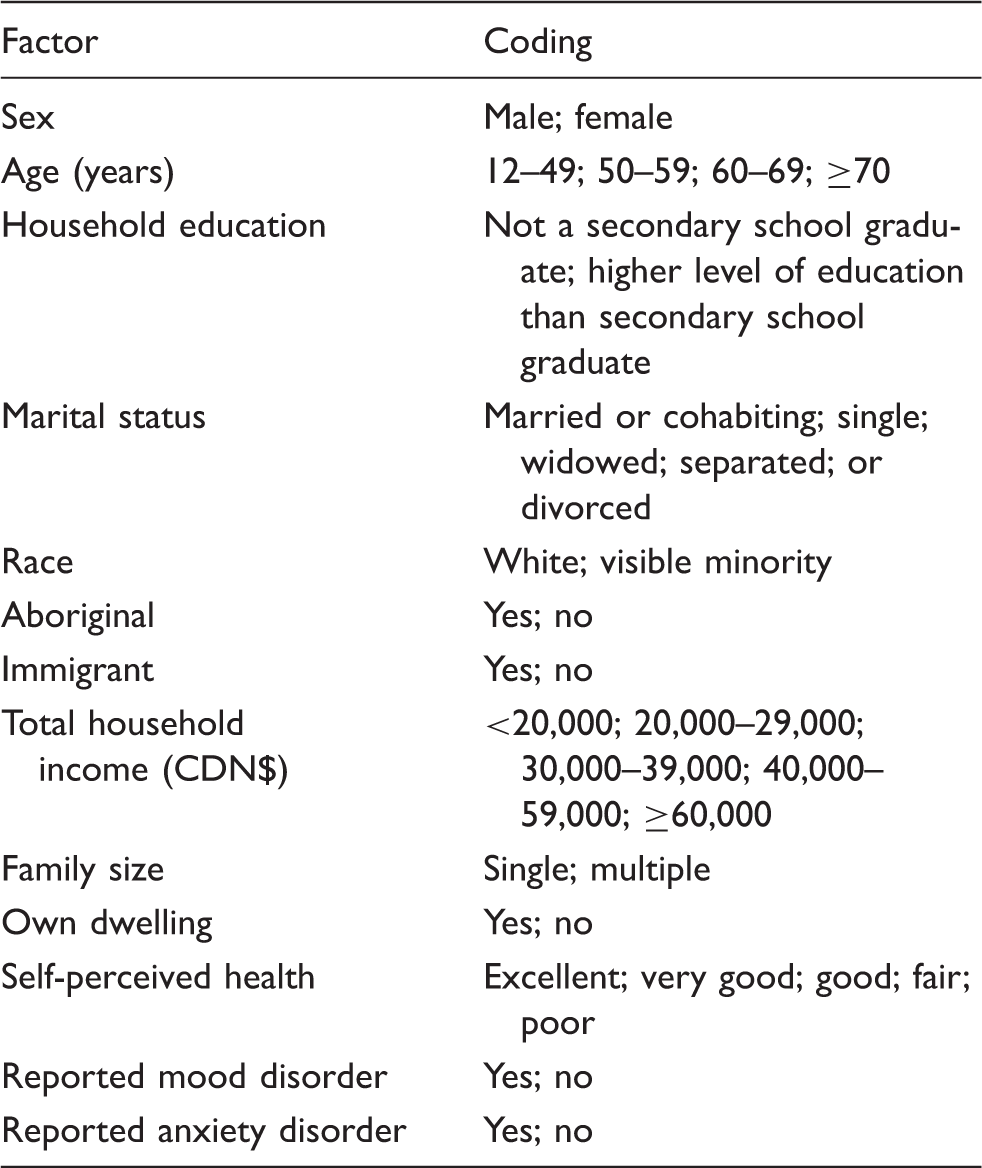
Variables in the univariate analysis that appeared to be related to the description of food insecurity by individuals reporting migraine were used to develop a multivariable logistic regression model of food insecurity within this population. The multivariable model was developed interactively using backward elimination, with testing of all eliminated variables simultaneously. In alignment with the requirements of Statistics Canada, variables with coefficients of variation >16% were also removed (18). Goodness of fit statistics and the area under the curve for the receiver-operating curve were used to assess the adequacy of the model.
To determine whether food insecurity was unique to people reporting migraine or was also associated with other chronic medical conditions, we identified a number of reported medical conditions within the CCHS that were persistent, highly prevalent within the population, and affected the entire age spectrum. Using these criteria, we elected to examine asthma, arthritis, bowel disorders, and diabetes. We developed a multivariable logistic regression model of food security within the complete population using identical methodology, then assessed the impact of adding reported migraine and then the other reported conditions (asthma, arthritis, bowel disorders, and diabetes).
The data were analyzed using Stata/SE 12 (19). Weights were recoded to reflect the sample size (an average weight of 1). Measures of associations are reported as odds ratios (OR) with 95% confidence intervals. All statistics given are for non-missing data. Estimates were obtained using sampling weights provided by Statistics Canada to account for design effects and non-response bias; standard errors were estimated using a bootstrapping procedure.
Results
Within the 2013 CCHS, a total of 48,645 respondents answered affirmatively or not to whether they had migraine diagnosed by a health professional and had evaluable responses as to whether they resided in a food secure household or not. Household food security was available across all respondent ages. The rates of missing data by the variables examined (Table 1) were low (range 0–3.2%).
Having migraine was reported by 4614 individuals, accounting for a weighted point prevalence of 10.2% (95% confidence interval (CI) 9.8–10.7%), representing 2,399,300 young people and adults reporting migraine nationwide. This point prevalence appears relatively stable over the past eight years (10.7% in 2005 and 10.5% in 2009). A total of 7.6% of the sample was assessed as experiencing household food insecurity (95% CI 7.1–8.1%). Household food insecurity was considerably more likely to be reported among those reporting migraine compared with respondents not reporting migraine (14.8 versus 6.8%, respectively; OR = 2.4, 95% CI 2.0–2.8). The rates of reporting food insecurity within the Canadian population and specifically food insecurity within those reporting migraine does not appear to have substantively changed over the past eight years (Figure 1).
Reported food insecurity (%) for the Canadian population and those reporting migraine over the past eight years in the Canadian Community Health Survey (CCHS) 2005 (Canada, excluding Saskatchewan, Manitoba, New Brunswick, Newfoundland and Yukon Territory), CCHS 2009 (Canada, excluding New Brunswick and Prince Edward Island), and CCHS 2013 (Canada, excluding British Columbia, Manitoba, Newfoundland and Labrador, and Yukon Territory). Vertical bars reflect 95% confidence intervals for the population estimates.
Multivariable logistic regression model of factors associated with household food insecurity among individuals reporting migraine (n = 4,614) in the Canadian Community Health Survey 2013 (excluding respondents from British Columbia, Manitoba, Newfoundland and Labrador, and Yukon Territory).

Notes: a Total household income, cumulative <0.001. Area under the curve for the receiver-operating curve was 0.83 (95% CI 0.81–0.85). Model developed on 4590/4614 eligible cases (99.5%).
Association of reported health conditions with food insecurity in a multivariable logistic regression model (n = 48,645) in the Canadian Community Health Survey 2013 (excluding respondents from British Columbia, Manitoba, Newfoundland and Labrador, and Yukon Territory).

Notes: Adjusted odds ratios after adjustment for age, marital status, aboriginal status, total household income, family size, own dwelling, self-perceived health, reported mood disorder, and reported anxiety disorder.
Discussion
Food insecurity is reported by approximately 15% of US (21) and 13% of Canadian households (3). The factors that underlie food insecurity include poverty and difficulty in accessing appropriate grocery stores. Travel to stores with healthy affordable food can be challenging for those who live in rural or urban food deserts, where shopping is often dependent on being able to access a vehicle. Even when the challenge of accessing stores is overcome, budgeting for appropriate food must compete with escalating housing and medical costs. A lack of education, unawareness of appropriate food choices, or mental illness may also be related to food insecurity.
Using a representative sample of Canadians, we demonstrated an association between migraine and food insecurity. Among individuals with migraine, the risk was greater in those who were younger, female, lived with others, earned less than CDN$30,000 per annum, and did not own their own dwelling. Self-reporting a mood disorder and self-perceiving health as only fair or poor were also associated with food insecurity. At a population level, even after correcting for the known associations, migraine was still associated with food insecurity. This association is unlikely to be merely a reflection of having a chronic illness, as neither diabetes nor bowel-related disorders was related to food insecurity, but migraine, asthma, and arthritis were related to food insecurity. This may reflect the greater impact of these conditions on mobility and the ability to access healthy food.
Migraine and food insecurity share a number of associations. Both migraine (22) and food insecurity (23) are associated with anxiety and depression. Psychological stress and dietary habits, including missed meals and hunger, are among the most frequent precipitants of migraine (24,25). Migraine may contribute to a higher incidence of food insecurity by resulting in days of inability or reduced ability to perform normal household activities (26,27), including shopping and cooking. For many individuals with migraine, the occurrence of headaches may also preclude attendance at work (28), which results in costs (29,30) including lost income.
Stewart et al. (31) found a higher incidence of migraine as household income decreased, which they proposed supported a social causation hypothesis, as opposed to a social selection hypothesis. In the former, lower household income is associated with stress and other factors that increase the incidence and duration of an illness. Social selection proposes that a disease or illness can result in a decline in social status because the afflicted individual may underperform in their educational or occupational endeavors. We have demonstrated an association between food insecurity and migraine that persists after correction for income, in addition to other factors known to be associated with food insecurity. The directionality of this relationship appears to be as challenging as the relationship between income and migraine formulated by both the social causation and selection hypotheses. The cross-sectional design of our study does not allow a conclusion on the temporal order of food insecurity and migraine.
The CCHS is a nationally representative, population-based survey and is more likely to be truly representative of those living with migraine than clinic-based studies. Nationally representative health surveys are primarily designed to guide health policy. Their secondary analyses, as in this study, have the potential to pose and answer important clinically relevant questions.
The diagnosis of migraine in our patients was based on the reporting of a diagnosis by a health practitioner rather than on specific criteria. To our knowledge, the question about migraine used in the CCHS has not been validated. However, a similar question, “Have you ever had migraine?”, has been validated against a diagnostic telephone interview administered by physicians trained in headache diagnosis, with a sensitivity of 75.8% (95% CI 72.4–79.0%) and specificity of 86.4% (95% CI 84.3–88.3%) (32) and, when assessed within a clinical interview, with an associated κ of 0.77 (33). In an internet-based study of patients reporting migraine, after reviewing the patients’ narrative description of headache qualities, a neurologist assigned a high or moderate probability of migraine to 97% of patients, and also to 97% of patients using International Headache Society criteria (34). These studies suggest that the question used in the CCHS may be valid. In addition, our reported migraine prevalence was comparable with other similar Canadian studies that found a prevalence of 7.9% (35) and 8.3% (36).
The assessment of experience-based food insecurity has been measured by various questionnaires, most notably the 18-item Household Food Security Survey Module (14) and its precursor the Core Food Security Measurement (37). The questions asked within the CCHS are adopted from this US model of food security (38). The favorable psychometric properties of the Household Food Security Survey Module (14) have been reviewed (37,39).
The experience of food insecurity appears to be more frequent among individuals reporting migraine and some, but not all, chronic diseases. Clinicians who treat migraine should be aware that their patients are more likely to experience food insecurity.
Qualifier
The analysis presented in this paper was conducted at the Atlantic Research Data Centre, which is part of the Canadian Research Data Centre Network. The services and activities provided by the Atlantic Research Data Centre are made possible by the financial or in-kind support of the Social Sciences and Humanities Research Council, the Canadian Institutes of Health Research, the Canada Foundation for Innovation, Statistics Canada, and Dalhousie University. The views expressed in this paper do not necessarily represent the Canadian Research Data Centre Network or those of its partners.
Public health relevance
This is the first description of increased household food insecurity by individuals reporting migraine derived from a large national health dataset of Canadians. Food insecurity was reported by 14.8% of individuals reporting migraine versus 6.8% of those not reporting migraine (OR 2.4). In a multivariable model of food insecurity at the population level, after correcting for a number of known associations with food insecurity, migraine continued to have a modest association with food insecurity (OR 1.5).
Footnotes
Acknowledgments
The authors acknowledge the assistance of the staff at the Atlantic Research Data Centre.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the Social Sciences and Humanities Research Council of Canada RDC Access Granting Committee (grant number 14-SSHDAL-3854).