
Abstract
Background
Recent evidence shows that multidisciplinary treatment is effective in chronic pain syndromes, especially in headache disorders.
Aim
The aim of this review is to summarize current knowledge on integrative care concepts in headache patients regarding the optimal and necessary treatment parts, optimal duration and setting.
Methods
We present a narrative review reporting current literature and personal experience.
Results and conclusion
Based on current knowledge, multidisciplinary treatment programs appear to be reasonable and efficient in headache disorders. Sufficient controlled studies regarding the need for individual parts of the integrative care approach are missing as yet. Recommendations are therefore at least partly based on personal experiences. It seems to be unambiguous that patients should be referred to a specialized headache center offering such a program instead of being sent sequentially to various medical specialists. The extent and kind of required therapy (e.g. personal consultation versus group sessions) is not known yet. All patients should learn relaxation training, although it is unclear yet which training is the best for which patient. Physiotherapy with guidance on more activity and individual exercises should be used in all patients. Some patients might benefit from cognitive behavioral therapy. However, therapies often depend more on country-specific health care systems than on clinical needs or scientific data.
Keywords
Introduction
Multidisciplinary treatment concepts are generally accepted as the best available and efficient treatment option for chronic pain patients (1). During the last decades, such concepts have been established for the treatment of headache patients and the outcomes at some multidisciplinary pain clinics have been published previously (for review, see Diener et al. (2)). However, it is still enigmatic which particular treatment disciplines are necessary within this concept, which therapeutic approaches are mandatory parts for successful multidisciplinary care in headache patients and which treatment parts may be redundant or unnecessary. Components and team players of multidisciplinary treatment are shown in Figure 1. Furthermore, optimal treatment duration (especially minimal time needed) and setting (indication for inpatient versus outpatient treatment) is not yet known.
Reliable predictors of good outcome in such programs have thus far been missing. Results of multidisciplinary treatment have mainly been published regarding episodic and chronic migraine, tension-type headache (TTH) and medication-overuse headache (MOH). Only some data exist on multidisciplinary treatment on post-traumatic headache without revealing evidence for high efficacy of specific treatment concepts. Cognitive behavioral treatment failed to show superiority compared to a waiting list control group (3). However, based on general considerations a multidisciplinary treatment setting is recommended (4).
Patients suffering from rare headaches, like cluster headache, and patients with secondary headache may benefit from a multidisciplinary treatment approach, too. Studies regarding this topic have thus far not been conducted.
Definition, structure, and concept of multidisciplinary care
Multimodal pain therapy describes an integrated multidisciplinary treatment in (small) groups with a closely coordinated therapeutic approach. This is clearly more than just an uncoordinated mixture of different therapies. Somatic and psychotherapeutic procedures are combined with physical and psychological training programs that can be performed in an inpatient, outpatient or day clinic concept. Available settings depend on country-specific health care systems (for example: inpatient rehabilitation is well established in Germany but not available for pain therapy in the majority of countries) as well as on economic resources.
It is still not clear if diagnosis-specific groups are superior to groups of mixed diagnosis. Pain clinics are established for pain therapy in general (including headache patients) whereas some pain clinics are exclusively focused on headache patients without showing superiority of one of those concepts (6). One could argue that there are substantial pathophysiological differences between chronic pain syndromes like fibromyalgia or chronic low back pain and headaches that might need different treatment concepts. However, many patients suffering from chronic headaches have additional comorbid pain syndromes like chronic low back pain, which would support the concept of a broader approach (7). Based on our clinical experience, which is in line with published data, anxiety is an important comorbidity in headache sufferers, especially migraineurs. Epidemiological data showed that up to two-thirds of migraineurs suffer from anxiety disorders (8), whereas in patients with functional somatic syndromes such as fibromyalgia mood disorders are more frequent than anxiety disorders (9). This might be due to the nature of the disease occurring often in attacks that are unpredictable for the patients.
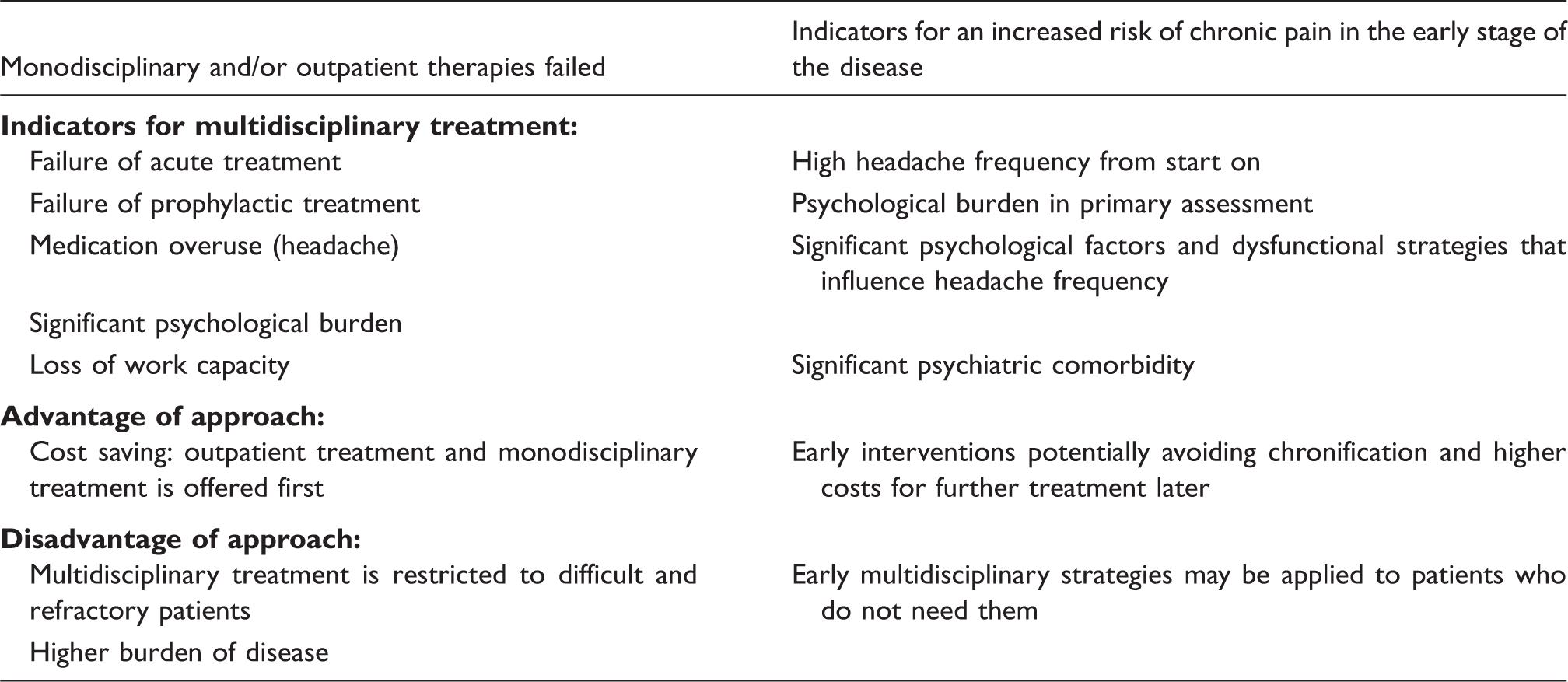
For chronic pain syndromes with complex somatic, psychological and social consequences, a therapeutic intensity of at least 100 hours is recommended (10,11). However, headache-specific day care with a one-week (36 hours of treatment) concept revealed acceptable outcome parameters regarding headache frequency and relapse to medication overuse, too (12). Comparison of different concepts from various countries showed high variability of frequency and overall number of treatment sessions (5).
Different approaches to indication of multidisciplinary therapy (concept adapted from Arnold et al. (10)).
Assessments
Data on the optimal assessment strategy within the integrated care concept are missing as yet. Based on our clinical experience as well as studies on assessments in chronic pain therapy (13), and published recommendations (14) an individually adapted therapeutic plan is mandatory for each patient, even though the underlying concepts are similar for the group of patients in general. Therefore, the assessment at the beginning of multidisciplinary therapy in our tertiary headache centers includes an analysis of individual burden of disease, aims of therapy from the patient’s and therapist’s view and assessment of psychiatric comorbidity. For headache patients, standardized assessment of headache symptoms and frequency, psychiatric comorbidity, burden of disease, and somatic illness are conducted. Using a headache diary should be standard to provide data on number of headache days, use of acute medication and loss of school or work days. Burden of disease and disability due to headache are measured using the Migraine Disability Assessment (MIDAS) (15), Headache Impact Test (HIT)-6 (16) or Headache Disability Inventory (HDI) (17). The Hospital Anxiety and Depression Scale (HADS) (18) has been used in the majority of headache studies for screening for depression and anxiety (e.g. COMOESTAS). However, there are numerous questionnaires that can be used as well. Each discipline within the team may add its own specific assessment as needed to get a complete impression of the participating patients. Findings from the complete assessments should be discussed in a case conference at the end of the analysis to determine specific goals of treatment for individual patients with respect to the individual patient’s wishes. At the end of the therapy, an outcome assessment is necessary to evaluate the treatment results, and to give individual recommendations for further treatment to the patients. Optimum would be a follow-up session some months after the multidisciplinary treatment to reevaluate and motivate the patient for further implementation of the contents of the treatment into daily life.
Components of multidisciplinary care
Pharmacological treatment
Optimization of drug treatment regarding acute and prophylactic treatment is a main part in therapy of headache disorders. Recently published data showed that inadequate efficacy of acute treatment of migraine attacks may result in an increased risk of new-onset chronic migraine. Therefore, optimizing acute treatment is an essential part of individual counseling of headache patients (19). In acute treatment, using different triptans and different types of application (oral versus nasal spray versus subcutaneous) to identify those with optimal efficacy or adding a long-acting nonsteroidal anti-inflammatory (NSAID) to the triptan might be helpful (20). Various substance groups are available for prophylactic treatment depending on headache diagnosis and headache frequency. However, individual treatment decisions are influenced by somatic comorbidity, psychological comorbidity and patient preferences. Especially information on the mechanism of action, particularly time of intake for acute medication and potential side effects, are important.
Patient education
Patient education is an important and effective part in multidisciplinary headache care (21). Patient education may enhance self-efficacy and influence locus of control. Motivation and adherence to non-pharmacological therapy (aerobic endurance training and relaxation training) as well pharmacological therapy may be improved by headache-specific patient education. A prospective cohort study over 1.5 years including 109 patients with chronic primary headache and medication overuse showed that simple advice regarding medication overuse led to a significant reduction of medication intake. The mean medication days per month were reduced from 22 to six, and 42% of patients were no longer suffering from chronic headache (22).
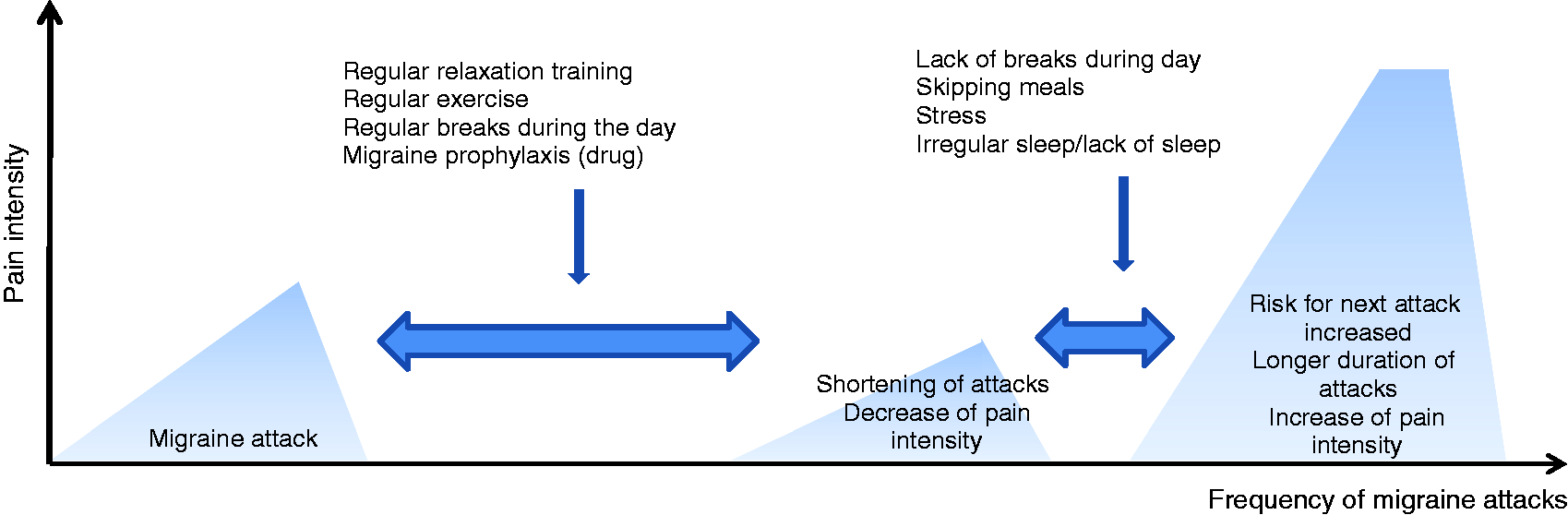
A figure that we use and discuss in patient education sessions is shown in Figure 2. The educational approaches result in increased quality of life, reduced disability and decrease of migraine frequency as shown in a recent meta-analysis of studies focusing on patient education (21). Patients with specific knowledge about their headache disorder and headache treatment may be more self-confident and successful in handling the headache disease.
Team players against headache: Multidisciplinary treatment of primary headaches and medication-overuse headache (modified from Gaul et al. (5)). Figure used for patients’ education and discussion about medical and non-medical migraine prophylaxis.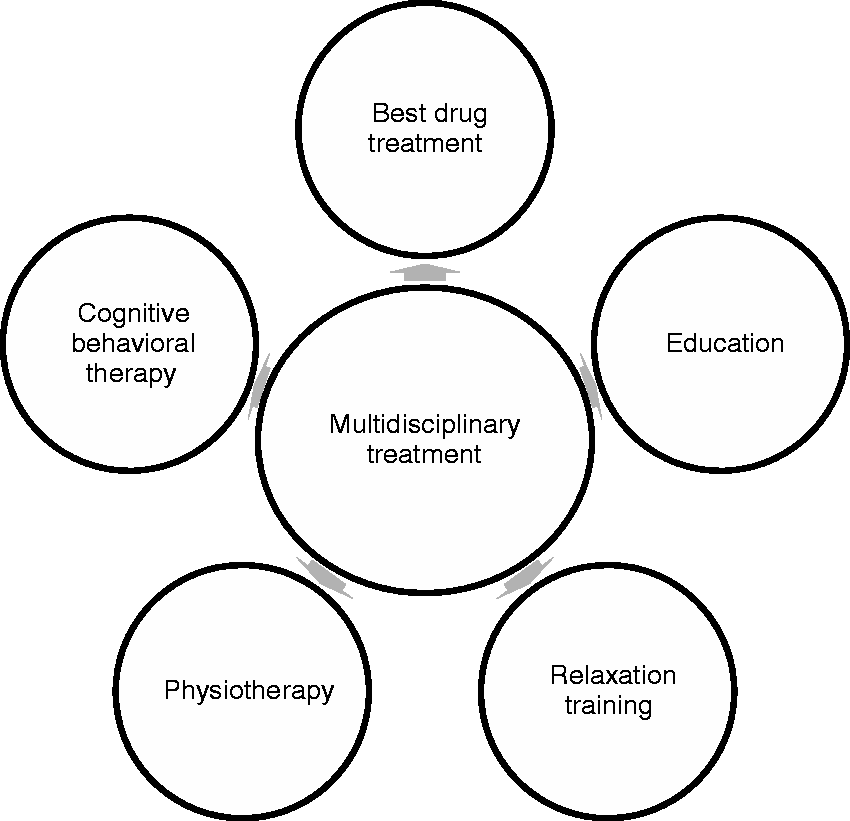

Content of non-medic patient education (adapted from Gaul (28)).

The interdisciplinary team
The interdisciplinary team consists of neurologists or pain specialists, headache nurses, physiotherapists, relaxation trainers and psychologists. Each has a unique specific role during the therapy. To avoid only a mixture of therapies, all members of the team should work based on the same model and use the same language to explain their approach to the patient. In our experience, a minimum of a weekly interdisciplinary team conference is necessary to discuss individual patient situations and further needs in the multidisciplinary therapy. Explanations given in individual sessions by each member of the team should fit the underlying pathophysiology and treatment explanations given to the patients in the education sessions (headache school) and be based on the biopsychosocial (BPS) (29) model with a uniform focus on self-efficacy. The BPS model states that biological, psychological and social factors play a crucial role in the underlying pathophysiology of headache disorders.
Neurologists and pain specialists
The physicians are responsible for the correct headache diagnosis according to the criteria of the International Headache Society (30). A clinical neurological examination should be performed in each patient. If needed, additional diagnostic work is necessary to exclude secondary headache. Furthermore, optimizing acute therapy and discussing options of prophylactic pharmacological treatment and of somatic comorbidity is a core role of neurologists and pain specialists on a multidisciplinary headache team. Psychiatric diagnosis and pharmacological treatment of psychiatric comorbidity is initiated in close collaboration with the psychologists. If necessary, additional medical disciplines (psychiatry, neurosurgery, internal medicine) are requested to add their input. The neurologist or pain therapist should explain the exact headache diagnosis to the patient and answer specific questions. The importance of the explanations to the patients cannot be overestimated; to accept and understand the headache diagnosis is a precondition for successful treatment afterward.
Headache nurse
The profile of a pain nurse has been established within the last decades. A headache nurse is specialist pain nurse focused on headache care. The roles of nurses in general are different across countries and different health care systems (31). Depending on the care system and the setting, the headache nurse will take a headache history, assess level of disability, provide and assess headache diaries, and provide follow-up to medical-clinical consultations, monitoring drug efficacy and tolerability. In some countries, the headache nurse even runs the educational headache schools. Overall there is a trend to move nurses’ training into an academic discipline. An internationally accepted curriculum for the education of headache nurses does not exist at the moment and may be different across countries. An important step forward is the continuous presence of headache nurses at national and international headache congresses. An international forum of headache nurses was established at The European Headache and Migraine Trust International Congress (EHMTIC) 2010 in Nice, France (5). At specialist units involved in research, the headache nurse is often responsible for parts of scientific work supported by study nurses. Nurses play a key role in direct contact with the patients, especially in inpatient units, as the primary contact person for the patients. Headache patients are often unsure in differentiating tension-type headache (TTH) from migraine and therefore acute treatment might be wrong or delayed, resulting in decreased efficacy. Together with the patient, the experienced headache nurse is able to distinguish between the headache diagnoses and may guide individual treatment behavior. In addition, the headache nurse can instruct patients in single or group sessions about useful non-medical treatment options or instruct cluster headache patients in the correct use of oxygen for attack treatment. Headache nurses can instruct patients on the use of noninvasive and invasive neuromodulation devices as well. In some countries in Scandinavia and the United Kingdom (UK), headache nurses give Botulinumtoxin injections and adjust med-therapy independently. Furthermore, they are responsible for programming of neurostimulators.
For some patients, the headache nurse will be the best at addressing patients’ queries on lifestyle issues and trigger factors. Overall, specialist headache nurses are likely to improve the patient’s experience and clinical organization because they are involved in all relevant areas of service delivery.
Physiotherapists
Neck pain is very common in headache patients and seems to be more associated with chronic than with episodic migraine (32,33). Furthermore, some patients report that the neck could act as a trigger for some migraines (34). As shown in studies, neck pain is a common symptom in TTH, too (35,36) and the development of myofascial trigger points with referred pain in the head can be a common sign. The convergences of nociceptive inputs from C1–C3 at the brainstem level into the trigeminal caudalis nucleus (37) (the so-called trigemino-cervical complex) might be the underlying mechanism of this. Based on clinical symptoms, patients are very open to physiotherapeutic interventions. Physiotherapy for the treatment of migraines and headaches requires a comprehensive assessment. Besides the headache anamnesis and some possible questionnaires (i.e. Neck Disability Index), the assessment contains an analysis of posture and functions. Helpful tests are the Craniocervical Flexion Test, the Flexion-Rotation Test, strength and extensibility tests, trigger points palpation and a manual joint palpation of the cervical spine (38,39). The aim of the assessments is to find and to improve restricted movements (i.e. thoracic extension), deviation of body position, muscle imbalances and malfunctions (i.e. dysfunction of the cervical spine) that may contain far-reaching consequences for the symptoms of headaches. An unphysiological posture with restricted thoracic spinal extension has to be counterbalanced by the muscles of the cervical spine and the shoulder girdle. In summation it results in overexerted muscles and joints. Different lengths of legs, for example, can cause pelvic obliquity and scoliosis. Both examples can maintain high muscular tension in the shoulder girdle and the cervical spine. The goal of physiotherapy should be the elimination of all contributory factors to prevent headache and migraines.
Other contributory factors for trigger points in daily life are unilateral stress, poor sight or permanent lifting of the shoulders. Without removing those contributory factors, the best therapy may still remain unsuccessful. In addition, many patients need intensive education and exercises for thoracic spine mobilization, antagonistic muscle strengthening and better body perception to control their posture. The therapeutic effect of exercises is strong in people with TTH (40), but there is still a lack of evidence in patients with migraine (40).
A recent systematic review and meta-analysis evaluated the efficacy of physiotherapeutic procedures in headache and migraine. Based on the results of this study, the current level of evidence regarding these therapies is low. Although data showed a significant reduction regarding intensity, frequency and duration in migraine, TTH and cervicogenic headache, the amount of reduction was often not clinically significant. Additionally, methodologically problems make it difficult to assess the efficacy of physiotherapy (41).
Passive methods like manual therapy, trigger point therapy or other physiotherapy methods should be used only in addition to active exercises but not as sole therapy. There is some evidence for the effect of manual therapy in people with primary chronic headache disorders (42). However, the passive methods are often the crux of the matter. Patients expect their therapists to solve their musculoskeletal problems. Therefore, it is important to repeatedly instruct patients (e. g. concerning the correlation between posture and neck pain) and to accurately explain the aim of every single treatment. It is important to strengthen the self-efficacy and self-reliance of every patient. Last but not least, physiotherapy seems to be more effective in combination with other treatments (43). To encourage patients with more active strategies, the education of patients should include those concepts and physiotherapy should be an integrated part of the multidisciplinary team. Physiotherapists as part of an interdisciplinary team provide information about patient motivation, attitude toward physical activity and physical status. Together with psychologists and physicians, their role is to overcome guarded movements or fear avoidance beliefs. Patients suffering from migraine attacks because of physical activity or endurance sports should be guided into physiotherapy driven by interval training or graded activity.
Psychologists
Psychological treatment is mandatory in a multidisciplinary treatment approach in headache disorders. Beside drug treatment and physiotherapy, behavioral therapy has been shown to be efficient in headache treatment to reduce frequency of headache attacks and lower burden of disease (44). The evidence-based forms of behavioral treatment can be categorized into a) relaxation therapy, b) biofeedback c) cognitive behavioral therapy and stress management and d) a combination of medical and behavioral therapy approaches (45). Overall, those behavioral treatments seem to be as effective as pharmacological therapy (46). Multidisciplinary care seems to be therefore more effective than monodisciplinary approaches in migraine as well as in TTH (47,48). Behavioral therapies are convincing regarding their long-term effects. Blanchard et al. showed that therapeutic success could be still shown in 78% of patients five years after treatment (49). Similar results could be detected in another study in which 65% of patients still had a benefit from behavioral treatment after four years (50). A study adding behavioral migraine management (compared to drug therapy alone) revealed that behavioral strategies can increase participants’ confidence in their ability to effectively self-manage migraine (headache self-efficacy). In addition, the study showed that behavioral migraine management also increased the belief that migraines can be influenced by one’s own behavior (internal headache locus of control) and decreased the belief that migraines are primarily influenced by chance or fate (chance headache locus of control) (51,52).
Indication for behavioral intervention is similar to the indication for pharmacological prophylaxis. Therefore, patients with frequent or chronic migraine and TTH as well as patients with MOH should get psychological treatment.
Patients with a high burden of disease, insufficient stress management and maladaptive cognitive and behavioral responses to headache (e.g. catastrophizing, fear-avoidance, endurance/over-activity) are especially strong candidates for psychological interventions.
Cognitive behavioral treatment strategies are appropriate for minimal-therapeutic settings that are characteristically for multimodal headache therapy within an integrated care concept. In the headache center Essen (Germany), psychoeducational group treatment consists of five sessions with about 10 participants and a duration of 1.5 hours each. Patients should learn to identify and modify patterns of behavior that promote and maintain headache. Additionally, disease acceptance and cognitive reorganization of avoidance strategies are encouraged (12).
Efficacy of multimodal therapy programs
Efficacy of multimodal therapy programs has been proven by several groups for different program types. Although the structure of the program and the participating occupational groups are quite similar, differences exist regarding pure ambulant, day care, stationary and rehabilitative programs (2). In a German study, 295 patients (210 migraine, 17 TTH, 68 combination of migraine and TTH, 68 further medication overuse) who participated in a day care program were re-assessed after 12 to 18 months. All patients suffered from highly chronified headache and common treatment had not led to improvement in the past. Mean headache frequency was reduced from 13.4 (±8.8) to 8.8 (±8.0) days per month. Forty-three percent of patients reached the primary end point, which was reduction of headache frequency by more than 50%. Sixty-five percent of patients reported a significant reduction of headache days. Initially, 102 of the 295 patients suffered from chronic headache (≥15 headache days per month). More than half of these patients (55%) changed to an episodic headache within the study. The more patients followed the therapeutic recommendations (adherence), the greater improvement could be observed. Only five of 56 patients (8.9%) showed renewed medication overuse or developed new medication overuse (4.4%), which is much less compared to previous study data. These study results confirm the efficacy of this treatment program, especially regarding headache chronification due to medication overuse (12). Good study results for multimodal treatment approaches have also been shown by other groups in Germany and Denmark (53,54).
Multidisciplinary headache care for all headache patients?
Not all headache patients need a multidisciplinary approach for treatment of their headache disorder. Individuals with episodic migraine and TTH with a low frequency of headache attacks, well-treatable headache attacks and a low burden of disease do not have to participate in an integrated care program, although they might benefit from the education part—especially regarding optimal medication and pathophysiology of the headache disorder—and from physiotherapy. Other headache disorders are accompanied by a high burden of disease and therefore may benefit from an early referral to multidisciplinary headache care to avoid further chronification. These headache disorders include high-frequent/chronic migraine, high-frequent TTH and MOH, which are responsible for almost all headache-related burden (55). Integrated headache programs might also be important in special treatment situations such as pregnancy or in patients with cluster headache, but data on this special topic are still missing. Experts estimate that 1–10% of headache patients need multidisciplinary headache care (55). In a UK general practice, 9% of headache patients were referred to a secondary care program (56).
Inpatient versus outpatient: How should headache patients be treated?
Only few data exist comparing inpatient and outpatient programs. Créac’h et al. compared the efficacy of inpatient and outpatient withdrawal programs for patients suffering from MOH (56). Eighty-two patients were recruited for this open-label prospective randomized trial. Seventy-one patients reported complete drug withdrawal (36 of the outpatient group, 35 of the inpatient group). No significant differences between the two treatment groups could be detected. The authors concluded that outpatient treatment programs should be preferred at least for uncomplicated MOH, as they seem to be as effective as inpatient programs but much less expensive. A recent Italian study compared the effectiveness of an educational strategy (“advice to withdraw alone”) with that of two structured pharmacological detoxification programs in patients with complicated MOH plus migraine. Inpatient withdrawal was significantly more effective than advice alone or an outpatient strategy for those patients with a diagnosis of co-existent and complicating medical illnesses, a current diagnosis of mood disorder, anxiety disorder, eating disorder, or substance addiction disorder, relapse after previous detoxification treatment, social and environmental problems and daily use of multiple doses of symptomatic medications (57). As a consequence of the lack of clear superiority of one setting or concept, an unquestionable recommendation could not be given.
Outcome predictors
Only few data are available about outcome predictors of multidisciplinary headache treatment. Multivariate analysis in a study by Jensen et al. revealed female gender, diagnosis of migraine, MOH (especially triptans) and headache frequency of 10 days/month as positive outcome predictors for ≥50% reduction in headache frequency, whereas TTH and overuse of simple analgesics were predictors for poor outcome (53). A three-year follow-up study of 150 patients who received inpatient treatment for MOH revealed that being single, unemployment, higher baseline intake of acute medication, less coffee consumption and some specific psychological variables are predictors of poor outcome of relapse of MOH (58). Our own study revealed the diagnosis of migraine and migraine with additional TTH as predictors of good outcome (12). In contrast to the Copenhagen study, a higher number of headache days per month (21–25 days) showed the strongest headache reduction. Regarding the therapy, patients who showed high adherence to lifestyle recommendations revealed superior outcome compared to non-adherent patients (12). Positive outcome predictors in another study were younger patients, patients with few lost days at work or school and patients who were familiar with progressive muscle relaxation (PMR) at baseline (59). However, future research on outcome predictors is strongly required to adapt therapy to patient needs, and to save costs for patients and for society. Probably, treatment outcomes will improve by choosing the optimal multidisciplinary treatment concept for the individual patient in regard to his or her headache disorder.
Conclusion
Integrated multidisciplinary care has been shown to be an efficient therapeutic option in headache disorders although the optimal organization of integrated care programs is still unclear. Multidisciplinary approaches may help to avoid further chronification of headache and treat/prevent development of medication overuse, especially in patients with chronic or frequent headache that goes along with a high burden of disease. Multidisciplinary care includes different occupational groups: neurologists/pain specialists, headache nurse, physiotherapists and psychologists. Distinct study data on the best structure for integrated multidisciplinary headache care are still scarce. Patient education plays a key part in this treatment approach. It focuses on strengthening patients’ self-efficacy and locus of control. Motivation and adherence regarding non-medical treatment options (endurance training, relaxation training) as well as drug treatment should be supported. Harmonization of all parts of a multidisciplinary treatment program is important to form a comprehensive concept. It seems to be important that patients take an active part in the therapy for successful treatment. Further research should focus on optimization of multidisciplinary treatment concepts considering individual patient needs as well as the headache disorder.
Clinical implications
Integrated multidisciplinary care has been shown to be an efficient therapeutic option in headache disorders. Patient education plays a key part in multidisciplinary headache treatment. Motivation and adherence regarding non-medical treatment options (endurance training, relaxation training) as well as drug treatment should be supported. It seems to be important that patients take an active part in the therapy for successful treatment.
Footnotes
Acknowledgment
All authors are employed in clinics providing multidisciplinary headache care.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.