
Abstract
Introduction
The relationship between migraine and coronary heart disease (CHD) remains controversial. We aimed to investigate the association of subclinical atherosclerosis and migraine with or without aura compared to a non-migraine subgroup (reference) in a large Brazilian multicentric cohort study, the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil).
Methods
Migraine diagnostic was based on International Headache Society criteria, and aura symptoms were validated by a medical doctor in a sub-sample of the ELSA-Brasil, who also underwent coronary artery calcium score (CAC) and carotid intima-media thickness (C-IMT) evaluations. Subclinical atherosclerosis indexes (CAC and C-IMT) were analyzed as dependent variables and migraine (all, with aura, without aura) as an independent variable in the linear and multinomial logistic regression models adjusted for possible confounders.
Results
Of 3217 ELSA participants free from CVD at baseline, we found a migraine frequency of 11.9% (5.1% with aura and 6.8% without aura). Overall, migraineurs were mostly women, younger and had lower frequency of CV risk factors, such as hypertension, diabetes and low HDL-cholesterol, compared to non-migraineurs. The strongest inverse correlation between migraine and subclinical atherosclerosis was verified with CAC score. However, all associations lost their significance after multivariate adjustment.
Conclusions
In this cross-sectional evaluation of the ELSA study, migraine was not associated with subclinical atherosclerosis, regardless of aura symptoms.
Introduction
The relationship of migraine, particularly migraine with aura (MA), and cardiovascular disease (CVD) outcomes including coronary heart disease (CHD), remains controversial (1–7). Two previous meta-analyses depicted some positive associations between CHD and migraine (1,2). The first one, which included data from nine cohorts (3,5,6,8–10), found an increased risk of having angina of approximately 30% in individuals with any migraine subtype in their polled analysis (1). The second and more recent meta-analysis, which included 15 studies (one case-control, one cross-sectional and 13 cohort studies), focusing on the relationship with migraine, ischemic heart disease (angina, myocardial infarction (MI), coronary revascularization) and associated mortality, also found positive associations for CHD outcomes and migraine (2). Particularly for the relationship between MA and MI, the risk estimation exceeded more than double (pooled adjusted effect estimation: 2.61, 95% confidence interval (CI) 1.86–3.65) (2). More consistent findings come from a prospective cohort of middle-aged women that reported migraineurs with aura symptoms with the highest relative risks (about two times) for MI, angina and cardiovascular mortality 10 years later (3,4). Additionally, a population based-cohort also evidenced MA associated with all-cause and CVD mortality after more than 25 years of follow-up, regardless of sex (11).
The putative underlying mechanisms linking migraine headache with CHD are not very elucidated but might be partially mediated by pro-inflammatory, coagulation factors (12) or classical cardiovascular risk factors (CVRFs) (13–18).
The evaluation of subclinical atherosclerosis using coronary artery calcification (CAC), which has more correlation with advanced atherosclerotic lesions (19), and carotid intima-media thickness (C-IMT), which would be an earlier marker of atherosclerosis by the detection of the average intima-media thickness in carotid arteries, could be useful exams to early identify migraineurs with potential risk of CHD (20).
Although several studies have evaluated C-IMT and migraine (21–28), none has studied the relationship between CAC score and migraine according to aura symptoms in a population without previous CVD. Thus, we aimed to investigate the relationship with migraine, particularly MA, and both subclinical atherosclerosis markers in a large Brazilian multicentric cohort study (The Brazilian Longitudinal Study of Adult Health: ELSA-Brasil) (29,30), in which the frequency of migraine have been reported as relatively high (17).
Methods
Study design and population
This a cross-sectional analysis based on a subset of the ELSA-Brasil, which is a prospective multicenter cohort study involving 15,105 middle-aged civil servants from six cities (Belo Horizonte, Porto Alegre, Rio de Janeiro, Salvador, São Paulo and Vitoria). Baseline assessment occurred between 2008 and 2010 and the first follow-up period (four years after baseline) is finishing. Further details of the ELSA-Brasil cohort are described elsewhere (29,30).
Of 5061 participants from the São Paulo center, 4369 underwent both CAC (measured only at this research center) and IMT measurements. Also, all of them have complete information about migraine headaches. As our focus is subclinical atherosclerosis, we excluded 257 participants who reported previous history of CVD (CHD, myocardial revascularization, heart failure and stroke) resulting in 4112 participants. In addition, we excluded 874 participants with probable migraine and 21 who had missing information for aura classification. Ultimately, we analyzed complete data on main outcomes (CAC, C-IMT and migraine) from 3217 participants: 383 with definite migraine (163 with aura and 220 without aura) compared to 2834 individuals without migraine. Approvals from all institutional review boards were guaranteed.
Subclinical atherosclerosis indexes definitions
CAC
All participants underwent an electrocardiographic (ECG)-gated prospectively acquired CAC, performed in a 64-detector computed tomography scanner (Brilliance 64, Philips Healthcare, Best, Netherlands). Images were acquired with 120 kV and mA adjusted to body habitus, and reconstructed with standard filtered back projection. Images were transferred to a dedicated workstation where the CAC score was measured using the Agatston score. The CAC score was analyzed as a continuous variable and categorized (0/1–100/ > 100) (31).
C-IMT
C-IMT corresponds to the mean value between the average of left common carotid artery-IMT values and the average of right common carotid artery-IMT values obtained from high-quality images for both common carotid arteries during three cardiac cycles. We used MIA™ software to standardize the quality control, reading and interpretation of carotid scans, centralized in the ELSA-Brasil investigation center in São Paulo (32,33). We used the average C-IMT values from both arteries combined as the main C-IMT variable for this paper, as adopted by others (34,35). We analyzed C-IMT as a continuous variable and dichotomized using a cut-off at the 75th percentile of the sample (0.68 mm).
Migraine definition
All participants who answered “yes” to the question “In the last 12 months, did you have a headache?” at the ELSA-Brasil baseline evaluation were invited to answer a detailed headache questionnaire based on the International Headache Society criteria (IHS-2004) (36) that was adapted, validated and previously used in Brazil (37). Briefly, it investigates pain frequency, duration, quality, location, intensity, triggering and accompanying symptoms, such as nausea or vomiting and the presence of aura. We classified individuals who answered “yes” to the question about headache and fulfilled all criteria for migraine as definite migraine. Based on this questionnaire, we classified participants as having definite migraine if they fulfilled criteria for IHS codes 1.1 (migraine without aura, MO) or 1.2 (MA). We classified individuals who answered “yes” to the question about headache and fulfilled all criteria for migraine but one as probable migraine. Participants with other headaches or without headache were considered as having no migraine.
Further, all participants with a diagnosis of migraine completed a telephone interview performed by a medical doctor with great expertise in headache classification, including aura symptoms, based on IHS criteria (36). According to IHS criteria, typical aura consists of visual and/or sensory and/or speech complaints that occur gradually over 5–20 minutes and last no longer than 1 hour.
Finally, we collected information about prophylactic medications for migraine based on the 2012 guidelines of the American Academy of Neurology levels as follows: level A: antiepileptic drugs (divalproex sodium, sodium valproate, topiramate), beta-blockers (propranolol, metoprolol, timolol) and level B: antidepressants (amitriptyline, venlafaxine) and beta-blockers (atenolol, nadolol) (38).
Study variables
Each participant underwent an interview at the workplace and during a visit to the research center for clinical exams according to standard protocols (39). The interview and examination were performed by trained personnel with strict quality control. Questionnaires addressed age that was evaluated here as mean (±SE), years of education (up to incomplete high school, high school or incomplete graduation complete graduation), self-defined race (Black, Brown or White), smoking status (never, former and current), physical activity at leisure time (low, mild or vigorous) using the International Physical Activity Questionnaire (IPAQ)-Long Form. Blood pressure (BP) was taken using a validated oscillometric device, the Omron HEM 705CPINT. Three measurements were taken at 1-minute intervals. The mean of the two latest BP measurements was considered as the value for high BP definition. Hypertension was defined as the report of use of medications to treat hypertension, a systolic BP ≥ 140 mmHg or a diastolic blood pressure ≥ 90 mmHg at ELSA-Brasil baseline assessment. Diabetes was defined as a medical history of diabetes mellitus, the report of use of medications to treat diabetes mellitus, a fasting serum glucose ≥126 mg/dl, HbA1c levels ≥ 6.5% or a 2-hour oral glucose tolerance test ≥ 200 mg/dl. Dyslipidemia was defined as the report of use of lipid-lowering treatment or a low-density lipoprotein (LDL) cholesterol level ≥ 130 mg/dl.
Statistics
Baseline characteristics and subclinical atherosclerosis indexes are presented according to migraine subgroups (non-migraine, MO, MA and all migraine). Categorical data were analyzed by Chi-square test and presented in absolute and relative frequencies. Continuous data were analyzed by analysis of variance (ANOVA) with Bonferroni correction or Student T test and presented as mean (± standard error). We calculated odds ratios (OR) and ß coefficients with respective 95% confidence intervals (95% CI) for the association between atherosclerosis indexes (CAC and C-IMT)-dependent variables and migraine status (non-migraine, MA, MO, all migraine)-independent variables using a linear regression model (GLM) and multinomial logistic regression model (40) (CA: 1–100 and CA > 100 versus CAC = 0 and C-IMT ≥ P75 versus C-IMT < P75). All models are presented as crude, age, sex, race and multivariate adjustments for other possible confounders (educational attainment, hypertension, diabetes, obesity, physical activity and alcohol consumption). For all analyses, p values less than 0.05 were considered as significant. The statistical analyses were performed with the statistical software SPSS, version 22.0
Results
Baseline characteristics of 3217 participants from the ELSA-Brasil (São Paulo site), according to migraine status.
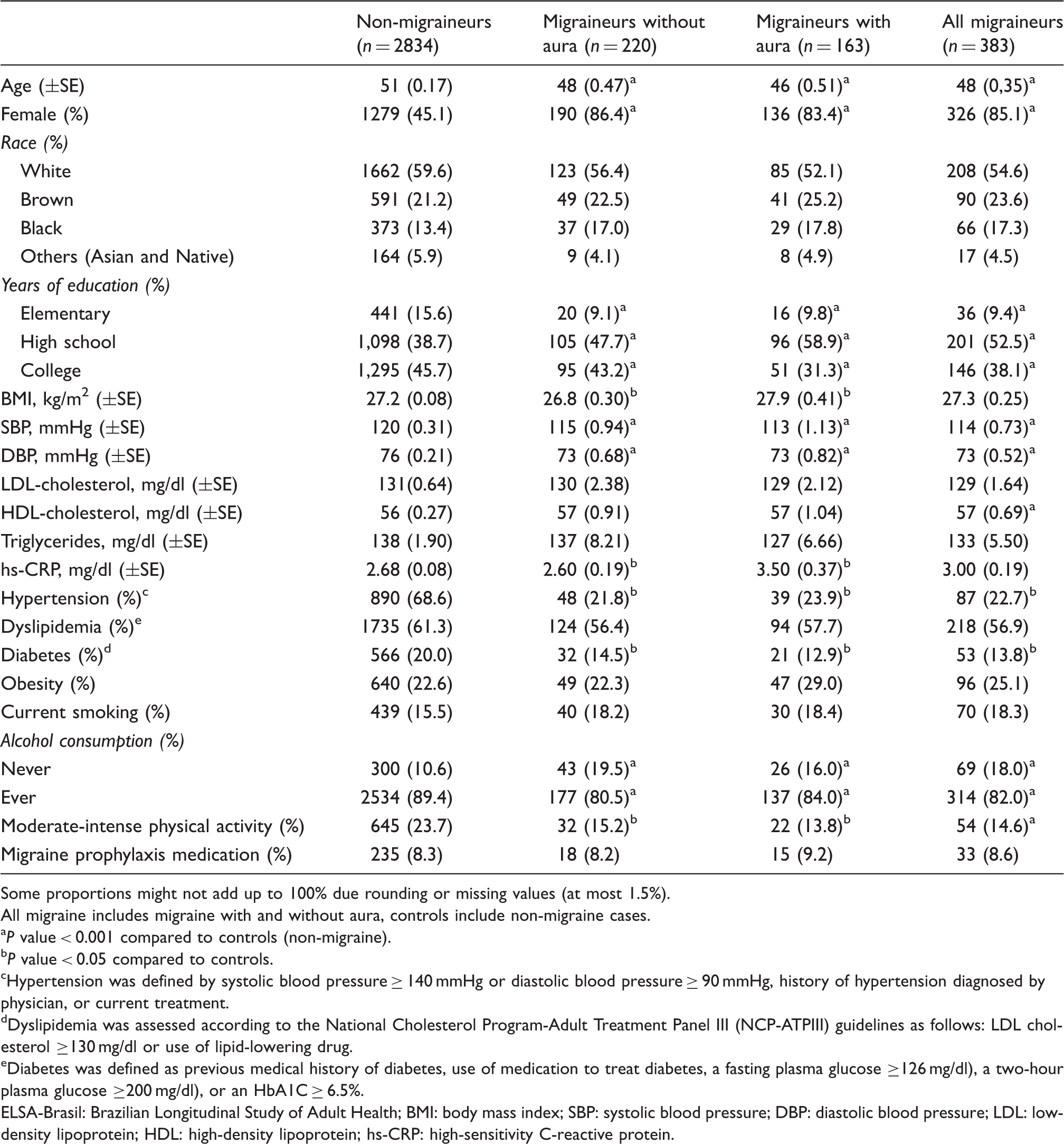
Some proportions might not add up to 100% due rounding or missing values (at most 1.5%).
All migraine includes migraine with and without aura, controls include non-migraine cases.
P value < 0.001 compared to controls (non-migraine).
P value < 0.05 compared to controls.
Hypertension was defined by systolic blood pressure ≥ 140 mmHg or diastolic blood pressure ≥ 90 mmHg, history of hypertension diagnosed by physician, or current treatment.
Dyslipidemia was assessed according to the National Cholesterol Program-Adult Treatment Panel III (NCP-ATPIII) guidelines as follows: LDL cholesterol ≥130 mg/dl or use of lipid-lowering drug.
Diabetes was defined as previous medical history of diabetes, use of medication to treat diabetes, a fasting plasma glucose ≥126 mg/dl), a two-hour plasma glucose ≥200 mg/dl), or an HbA1C ≥ 6.5%.
ELSA-Brasil: Brazilian Longitudinal Study of Adult Health; BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; LDL: low-density lipoprotein; HDL: high-density lipoprotein; hs-CRP: high-sensitivity C-reactive protein.
Atherosclerosis subclinical measures in the 3217 participants from the ELSA-Brasil (São Paulo Center), according to migraine status.

All migraine includes migraine with and without aura, controls includes non-migraine cases.
P value < 0.001 compared to controls (non-migraine). bP value < 0.05 compared to controls.
Comparisons between migraineurs with aura, without aura and non-migraineurs were estimated by ANOVA with Bonferroni post hoc test.
Comparisons between all migraineurs and non-migraineurs were estimated by Student T test.
ELSA-Brasil: Brazilian Longitudinal Study of Adult Health; CAC: coronary artery calcium score; C-IMT: carotid intima-media thickness; ANOVA: analysis of variance.
General linear model for the relationship between migraine, coronary artery calcium score and intima-media carotid thickness in the 3217 participants from the ELSA-Brasil (São Paulo Center), according to migraine status.

P value < 0.001 compared to controls (non-migraine). bP value < 0.05 compared to controls.
All multivariate analyses were adjusted by age, sex, race, educational level, smoking, hypertension, diabetes, obesity, physical activity, and alcohol consumption.
ELSA-Brasil: Brazilian Longitudinal Study of Adult Health; CAC: coronary artery calcium score; C-IMT: carotid intima-media thickness; OR: odds ratio; CI: confidence interval. 95% CI.
Odds ratio (95% CI) for the relationship with migraine, coronary artery calcium and intima-media carotid thickness in the ELSA-Brasil (São Paulo Center).

P value < 0.001 compared to controls (non-migraine). bP value < 0.05 compared to controls.
CAC = 0 was considered as the reference group.
C-IMT < 75th percentile was considered as the reference group.
All multivariate analyses were adjusted by age, sex, race, educational level, hypertension, diabetes, obesity, physical activity and alcohol consumption. ELSA-Brasil: Brazilian Longitudinal Study of Adult Health; OR: odds ratio; CI: confidence interval.
Discussion
In this cross-sectional evaluation, neither coronary calcification, which is a marker of more advanced atherosclerosis process (27) nor C-IMT, which is an early marker of subclinical atherosclerosis (20), were associated with migraine, regardless of aura symptoms.
CAC and migraine
The relationship between CHD and migraine has been described by several studies with divergent results (3,5–10). However, the association between subclinical coronary atherosclerosis and migraine in a population without previous CVD (MI, angina, revascularization, heart failure and stroke) has not been studied.
In the Women’s Ischemia Syndrome Evaluation (WISE), the presence of coronary artery atherosclerosis was evaluated by angiography among 905 middle-aged women with suggestive complaints of myocardial ischemia and answered positively to a simple migraine questionnaire, without aura information (10). Similar to our findings, in the WISE study, migraineurs were younger and with lower burden of CVRFs compared to non-migraineurs (10). In addition, migraineurs presented lower frequency of coronary artery disease by angiography (≥ 70% of stenosis in at least one coronary) compared to women without migraine even after multivariable adjustment. Of note, there are important differences between the WISE study and ours. First, our sample consisted of individuals without overt CVD, while in the enrollment of the WISE study the presence of chest pain or suspected ischemia was required. Therefore, we focused on subclinical atherosclerosis, and in the WISE study the evaluation of migraine was performed in a population with established CHD. Although both samples are not nationally representative of the population, we can argue that our sample is closer to a typical migraineur population. Moreover, migraineurs were much younger (mean age 48 versus 58 years old, respectively) with lower frequencies of cardiovascular risk factors at baseline compared to the WISE study population (10). In addition, our findings bring some additional information on MA symptoms, which were validated by a medical doctor according to IHS (20) in a sample that included both sexes.
C-IMT and migraine
Regarding carotid thickness and migraine, several previous studies depicted divergent results for this relationship (12,21–28).
Two prospective population-based studies performed in middle-aged and elderly migraineurs demonstrated inverse associations between C-IMT and migraine compared to non-migraine individuals (21,22). In the Epidemiology of Vascular Ageing (EVA) study’s cohort of 1373 people (59–71 years old), an inverse relationship between the highest C-IMT stratum (at baseline) and migraine (multivariate OR: 0.56; 95%CI: 0.34–0.93) (21) was demonstrated. Some limitations in this study such as age and the diagnosis of migraine, which was based on lifetime symptoms, asked four years later after the baseline assessment could add some recall bias. In the Bruneck study, another cohort performed in 574 individuals (55–94 years old), carotid atherosclerosis was not significantly different across subgroups of migraine (MA and MO) compared to a non-migraine subgroup. In fact, they found a trend of lower C-IMT (p = 0.029) among migraineurs than non-migraineurs after five years of follow-up. Finally, differently from our study, both mentioned studies did not exclude participants with previous CVD from their analyses and their populations were older than ours (31,32).
There are two studies with small and selected samples of participants with migraine-evidenced positive associations between C-IMT and migraine headache (23,24). In a matched case-control study performed in a restricted sample of 40 individuals without classical CVRFs, higher C-IMT values were described in the migraine subgroup compared to controls. In this study, no aura symptoms were reported (23). In the Hammed et al. study, among a small sample of 25 young migraineurs (MA: 14 and MO: 11) selected from a headache clinic who were free from CVD, diabetes, smoking and alcoholism, an increased OR for the association between C-IMT above the mean (> 0.71 mm) and overall migraine (OR: 2.20; 95 %CI: 1.10–4.40) was detected. However, they did not show multivariate ORs for subgroups of migraine (MA and MO) (24).
Similar to our findings, most studies that reported C-IMT as an arterial thickness measurement found no relationship with migraine, regardless of aura symptoms (25–28). Three of these studies were retrospective and composed of selected and small samples with approximately 20–30 migraineurs paired by controls, all free from CVD, diabetes or hypertension (25–27). The largest one, which evaluated a subsample of 360 migraineurs in a case-control nested in a population-based study, the Erasmus Rucphen Family study, found null association between C-IMT and migraine (28). In the Erasmus study, sample size of definite migraineurs (according to IHS criteria) was very similar to ours (36). However, ELSA participants were free from CVD, and in the Erasmus study participants with previous CVD or CVRFs were not excluded from their analyses.
Strengths
To the best of our knowledge, the evaluation of CAC score with migraine, including aura symptoms, is a novelty that has never been published before. Besides that, our population has a relatively high number of migraineurs with CAC score and C-IMT information (all migraine: 364; MO: 209 and MA: 155), who are prospectively followed regarding CVRFs, CAC score, some inflammatory biomarkers and migraine status.
Finally, we considered all medication about migraine prophylaxis in our multivariable analyses, including drugs such as beta-blockers and antidepressants that could influence some cardiovascular outcomes (41).
Limitations
Even though ELSA-Brasil is an ongoing multicentric prospective cohort, here we present cross-sectional baseline data from a subset of one single center in which was collected additional information on CAC score and MA symptoms. Thus, we cannot make causal inferences about the relationship between subclinical atherosclerosis and migraine.
Despite the fact that our descriptive results are not based on population data, our one-year migraine prevalence is quite similar to those previously reported by others (42–50). Prevalence of definite migraine during the last 12 months reported by previous Brazilian population-based studies varies from 10.7% to 22.1% (42–48). Also, some specialized clinical settings reported migraine prevalence rates about 30% (49). A recent non-systematic review based on six international population-based studies (50) confirmed these findings, reporting a slightly higher (prevalence of definite migraine in the last 12 months about 16%) compared to our rate (11.9%).
Although we cannot rule out the possibility of some bias in our study, aura symptoms were validated by a medical doctor specializing in this area, thus the possibility of misdiagnosis bias is unlikely. Moreover, the frequency of aura symptoms was about 40% for the total sample of migraineurs in our study, which is high but within the range described by other studies worldwide (51–55). Regarding national data, there is scarce information about aura characteristics performed in small and selected samples of very young migraineurs (42). Queiroz et al. evaluated 122 Brazilian and American young migraineurs, all with aura symptoms, in order to investigate aura characteristics and they found that more than 80% had visual aura symptoms (56).
Additionally, our study population is relatively young with low frequencies of CVRFs and consequently a low burden of atherosclerosis in the coronary and carotid arteries. However, data available from the follow-up of ELSA-study should be adding further information about this complex causal relationship.
Conclusions
Despite aura symptoms, migraine was not independently associated with subclinical atherosclerosis evaluated by CAC or C-IMT in a middle-aged Brazilian sample.
Clinical implications
The routine investigation of subclinical atherosclerosis is not indicated in migraineurs. Aura symptoms might not represent additional risk for the development of atherosclerosis in individuals with migraine.
Footnotes
Acknowledgments
The authors thank the research team of the ELSA-Brasil study for their contributions. The ethics committee of each ELSA-Brasil center approved this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The ELSA-Brasil baseline study was supported by the Brazilian Ministry of Health (Science and Technology Department) and the Brazilian Ministry of Science and Technology (Financiadora de Estudos e Projetos and CNPq National Research Council) (grants 01 06 0010.00 RS, 01 06 0212.00 BA, 01 06 0300.00 ES, 01 06 0278.00 MG, 01 06 0115.00 SP, 01 06 0071.00 RJ).