
Abstract
Context
The classification of headache disorders has improved over the years, but further work is needed to develop and improve headache diagnosis within headache subtypes. The present review is a call for action to implement laboratory tests in the classification and management of primary and some secondary headaches.
Background
In this narrative review we present and discuss published tests that might be useful in phenotyping and/or diagnosis of long-lasting headache disorders such as migraine, tension-type headache, trigeminal autonomic cephalalgias, trigeminal neuralgia and persisting secondary headaches.
Aim
The palpometer test, quantitative sensory testing, nociceptive blink reflex and autonomic tests may be valuable to phenotype and/or diagnose subforms of migraine, tension-type headache, cluster headache, trigeminal neuralgia and medication-overuse headache. Provocation tests with glyceryl trinitrate (GTN) and calcitonin gene-related peptide (CGRP) may be valuable in subclassification of migraine and cluster headache. Lumbar pressure monitoring and optical coherence tomography may valuable tools to diagnose and follow patients with chronic headache and raised intracranial pressure.
Finding
A number of laboratory tests in headache research are presently available, but have primarily been performed in single research studies or a few studies that differ in methods and patient groups. At present, there is no evidence-based strategy for implementing diagnostic tests, but this could be achieved if well-reputed tertiary headache centers commence developing and implementing laboratory tests in order to improve the classification and treatment of headache patients.
Keywords
Introduction
The classification of headache disorders improved greatly with the advent of the International Classification of Headache Disorders, first, second and third editions (1). The headache classification criteria have good inter-observer reliability (2), and diagnoses are made in a relatively uniform way throughout the world. Few other fields in neurology have unambiguous diagnostic criteria available for all entities, and few can show a similar high number of translations into the most important languages of the world. One might therefore think that the headache field is in an excellent position diagnostically, and that no further initiatives are needed to improve primary and secondary diagnostic criteria.
The same could be argued for the classification of psychiatric disorders, the Diagnostic and Statistical Manual of Mental Disorders (DSM), which is used in most parts of the world and has greatly improved psychiatric diagnosis. Nevertheless, the National Institute of Mental Health in the United States launched the Research Domain Criteria (RDoC) project to transform diagnosis by incorporating genetics, imaging, laboratory-based evaluations and other levels of information to lay the foundation for a new classification system (3). In the neuropathic pain field scientists likewise argue that diagnostic criteria need to be based on objective tests, such as quantitative sensory testing (QST) (4). To develop and improve headache classification, we believe it is necessary to move forward from a purely clinically based diagnosis to a diagnosis supported by laboratory tests. Routine tests such as computed tomography (CT), magnetic resonance (MR), electroencephalogram (EEG) and other neurophysiological tests have primarily been used to rule out secondary causes of relatively short-lasting headaches (5), and there are excellent reviews pointing out that these tests are often not necessary in clinically obvious cases of primary headache (5,6). Our present review has a different scope. We want to present and discuss published tests that can already be applied now relatively easily at headache centers and might be useful for the phenotyping and diagnosis of long-lasting headache disorders such as migraine, tension-type headache (TTH), trigeminal autonomic cephalalgias, trigeminal neuralgia (TN) and persisting headaches of secondary causes. Based on this narrative review, we suggest which laboratory tests may be ready to use in tertiary headache settings because they may help differentiate subtypes of headaches.
Diagnostic tests of headache patients
Palpometer test
It is of great interest to investigate the degree of myofascial tenderness in primary headaches, particularly in TTH. In the new revision of the ICHD third edition beta (ICHD-3 beta) (1), frequent episodic (eTTH) and chronic TTH (cTTH) is subdivided into patients with or without pericranial tenderness, which is not based on patient reporting, but on manual palpation by the examiner. In 1994 Bendtsen et al. (7) presented the so-called palpometer, which consists of a force-sensing resistor (FSR) connected to a voltmeter. The FSR is a thin polymer film device that is attached to the fingertip by means of thin adhesive tape (7). The device allows manual palpation with a defined and constant pressure, so called pressure-controlled palpation (PCP). Unfortunately, only four studies have so far used PCP. Bendtsen et al. (8) showed that using conventional palpation even among experienced observers the interobserver variation was 25% and the intraobserver variation was 7%. However, using the PCP reduced the interobserver variation to 7% and the intraobserver variation to 3% (8). Thus, the large interobserver variation using conventional manual palpation is likely to result in over- or underdiagnosis of TTH with pericranial tenderness (1) depending on the investigator. PCP also demonstrated increased pericranial myofascial tenderness in cTTH (9), which was confirmed in a later study showing increased pain sensitivity in cTTH patients over the trapezius muscle, but not over the anterior tibial muscle (10). Using the PCP method, it was shown as expected that the stimulus-response function recorded from the trapezius muscle in healthy controls was best described as a power function (i.e. pain intensities increased in a positively accelerating fashion with increasing pressure intensities) but, unexpectedly, the relation between pressure and induced pain was linear in the highly tender muscles of cTTH patients (9). The same pattern was seen when comparing the most tender cTTH group (linear pattern) to the least tender cTTH group (power function pattern) (9). Later, Ashina et al. also showed increased pain sensitivity in the trapezius muscle in cTTH using PCP (10). PCP may thus be a useful approach to study the status and the effect of treatment in eTTH with cTTH patients. Whether increased pericranial myofascial tenderness exists in other primary headache conditions remains to be studied with PCP. The principle of using FSR for palpation was patented before the above-mentioned studies. The inventors never studied the equipment and never produced a palpometer for commercial use. This unfortunate situation has hampered widespread use of PCP in headache clinics. The method is, however, ready for implementation in headache centers that may have a copy of this relatively simple equipment made locally. In routine use it can help in subdividing TTH patients into those with and those without muscle tenderness, but it may also be useful in subtyping other primary headaches and cranial neuralgias. PCP has not been tested in migraine, but may be useful in assessing those with a possible muscle component as a trigger of the pain. Furthermore, PCP may be effective as a tool to monitor changes over time and a way to measure the effect of pharmacological and non-pharmacological treatment.
Neurophysiological studies
From a diagnostic perspective, it is of great interest to study differences between headache subtypes using neurophysiological tests. A vast amount of studies investigated functional changes between attacks and differences between migraineurs and healthy controls (11). Unfortunately, only a few studies have investigated differences between migraine and other headaches.
Steady-state visual-evoked potentials (SSVEPs)
SSVEPs measure photic driving, which is the ability of cortical neurons to synchronize their firing with the frequency of visual stimuli. A mixed population of migraine patients, at low stimulation frequencies of 20 Hz or above, had a more pronounced photic drive than healthy controls (12), the so called “H-response” (abbreviated from headache). The H-response was consistent interictally and ictally and was sustained, even in patients who became headache free (12). It had 86% sensitivity and 98% specificity in migraine without (MO) and migraine with aura (MA) (13) and a high inter-test reliability in MO patients (14). One study showed an H-response in MO, but not in MA patients (15), whereas another study showed that migraine subtype, duration of illness, side of pain and frequency of migraine attacks did not correlate with the H-response (16). Furthermore, decreased photic drive interictally, which increased pre-ictally, was reported in MO patients (17). The H-response showed no difference between MO and TTH patients (18). Thus, the use of the H-response in terms of discriminating between migraine subtypes, headache subtypes and time of the migraine cycle needs to be further evaluated.
EEG phase synchronization
A method to study the dynamic interactions between brain areas and their modulation in the presence of stimuli is EEG phase synchronization. Recently, a group observed a decrease of effective connectivity in the beta band in MA, but increased functional connectivity in the alpha band in MO patients (19). The basis of these differences is not clear, but MO and MA may have different neurophysiological phenotypes that are measurable using phase synchronization. Further studies are needed, and it is uncertain if this method will ever be useful.
Visual-evoked potentials (VEPs)
Numerous studies have demonstrated that episodic migraine (EM) patients show a habituation deficit interictally, which reverses ictally (20,21). Visual-evoked responses to left hemifield checkerboard reversals have been recorded in EM patients and chronic migraine patients (CM) (interictally). Only EM had a habituation deficit interictally. Habituation was normal in CM and EM ictally (22). Interestingly, this habituation pattern changed in CM patients who remitted to EM after prophylactic topiramate treatment (23). To investigate possible central nervous system (CNS) generators of photo- and phonophobia, Sand and Vingen investigated if VEP or auditory evoked potential (AEP) amplitude correlated with light and sound discomfort thresholds in 21 migraine patients, but the study was negative (24). TTH showed no habituation deficit in VEPs, neither for eTTH (25,26) or cTTH (26). The same negative results were shown in cluster headache (CH) during and outside a cluster period (25). Blinded studies of the sensitivity and specificity in separating different types of headache are needed for these methods to be considered in the clinic.
Nociceptive-specific blink reflex (nBR)
All primary headaches are likely caused by activation and sensitization of the trigeminal nerve and/or the upper cervical nerves (27,28), which innervates the skull, eyes, nose and dura mater. It may therefore be diagnostically important to test the function of the trigeminal nerve. The trigeminal reflexes include the blink reflex, the masseter inhibitory reflex, the cornea reflex and the jaw reflex. The blink reflex is probably the most widely used in headache research. Its afferent leg is the trigeminal nerve and the efferent leg is the facial nerve with synapses in the brainstem. Following electrical stimulation of the supraorbital nerve, three components are detected: an ipsilateral early R1 component (onset latency 11 ms) and two polysynaptic bilateral medullary components R2 and R3 (onset latencies 33 and 84 ms) (29). A concentric surface electrode was developed (30) that produced a pin-prick-like pain. It preferentially stimulated nociceptive A-delta fibers without co-stimulation of non-nociceptive A-beta fibers and therefore mediated a nociceptive R2 response. The nociceptive R2 component was attenuated by local anesthetics (30) and central analgesics (31) and was therefore believed to be nociceptive specific. This nBR has been tested in migraine (32), TTH (33), CH (34) and TN (35).
Blink reflex migraine.

MO: migraine without aura; CTRLs: healthy controls; FHM: familial hemiplegic migraine; eTTH: episodic tension-type headache; nBR: nociceptive-specific blink reflex; MA: migraine with aura.
Blink reflex tension-type headache.
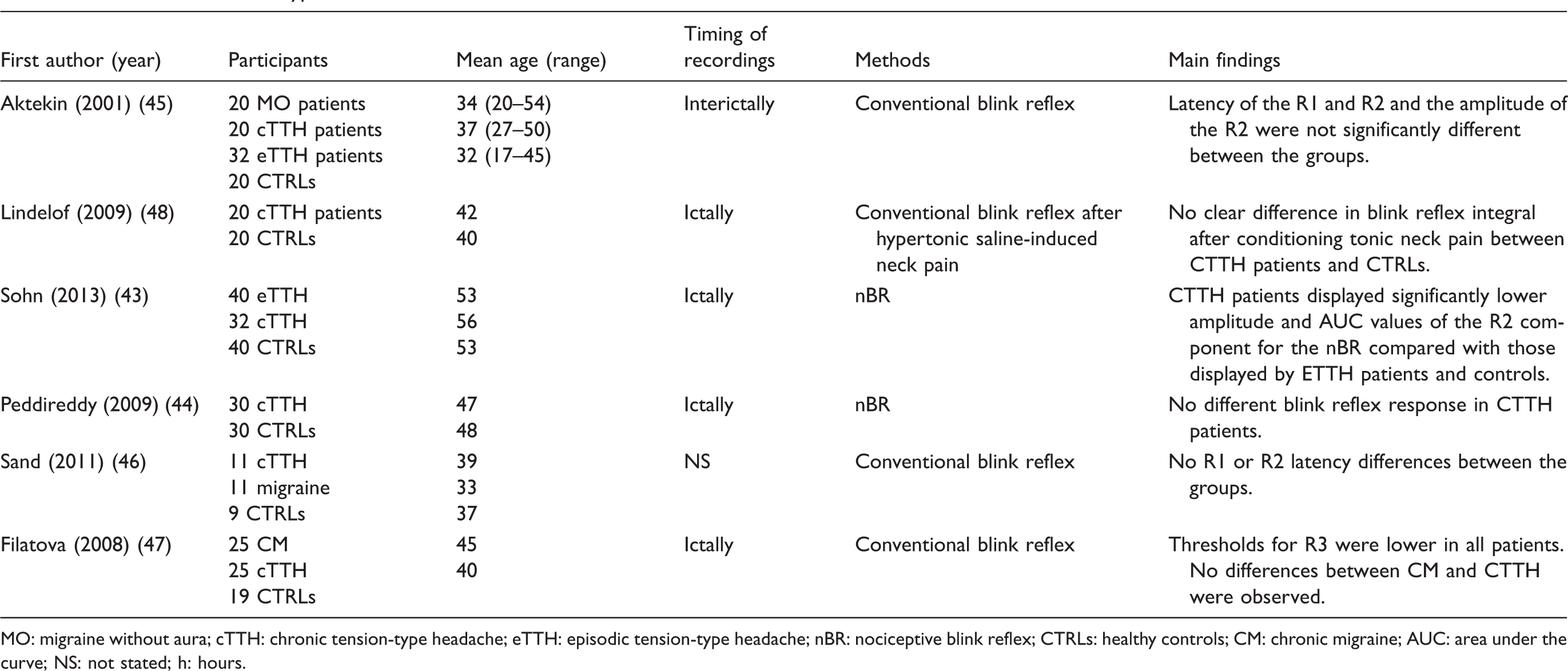
MO: migraine without aura; cTTH: chronic tension-type headache; eTTH: episodic tension-type headache; nBR: nociceptive blink reflex; CTRLs: healthy controls; CM: chronic migraine; AUC: area under the curve; NS: not stated; h: hours.
Blink reflex and cluster headache.

CH: cluster headache; ECH: episodic cluster headache; CCH: chronic cluster headache; CTRLs: healthy controls; nBR: nociception-specific blink reflex; MO: migraine without aura; NS: not stated.
Blink reflex trigeminal neuralgia.

TN: trigeminal neuralgia; nBR: nociception-specific blink reflex; CTRLs: healthy controls; NS: not stated; h: hours.
Overall, the nBR seems to give most valuable information only in migraine, CH and TN. If an increased R2 amplitude and decreased R2 latency is a sign of central sensitization, it is surprising that it has not been demonstrated clearly in TTH. The blink reflex may be useful in migraine and TN as a way of subclassifying patients, but whether this will have clinical and therapeutic consequences remain to be investigated.
Spontaneous EEG recordings
According to EFNS guidelines, EEG is not useful in the routine evaluation of headache patients (5) unless an underlying epilepsy disorder is suspected. However, EEG may be useful as a diagnostic tool to investigate neurophysiological phenotypes in primary headache. Three independent groups showed that MA patients interictally have interhemispheric asymmetry in frequency and power in the alpha range primarily in the occipital region in comparison to normal individuals (56–58), but MO patients did not (56). Repeated recordings in the same participants over the migraine cycle showed that the asymmetry increased in the preictal phase (<3 days before headache) (57). Other studies failed to reproduce these findings, but demonstrated instead interictal bilateral increase in theta power in the parieto-occipital regions (59) or globally (60) in mixed groups of MO and MA patients. The increase in theta power was positively correlated to headache intensity, but negatively to age and headache history (60). In the delta range power increased 36 hours (h) before the next attack compared with the interictal period (61).
At present, the overall understanding and clinical usefulness of EEG in headache disorders is non-existent. It remains to be shown whether high-density EEG with advanced computer analysis may improve the situation. So-called pharmaco-EEG has not yet been applied to headache studies.
QST
Quantitative sensory testing migraine patients.

eTTH: episodic tension-type headache; cTTH: chronic tension-type headache; CTRLs: healthy controls; MOH: medication-overuse headache; EM: episodic migraine; CM: chronic migraine; h: hours.
Quantitative sensory testing other primary headaches and trigeminal neuralgia.

MOH: medication-overuse headache; CTRLs: healthy controls; CCH: chronic cluster headache; ECH: episodic cluster headache; TN: trigeminal neuralgia; QST: quantitative sensory testing; NS: not stated; h: hours.
The pivotal study by Burstein et al. (63) employed repeated measurements of mechanical (via calibrated von Frey hairs) and thermal (via a thermode) pain thresholds of periorbital and forearm skin outside and during migraine attacks. In 79% of the patients, migraine attacks were associated with cutaneous allodynia occurring either within the referred pain area on the ipsilateral head, or within and outside the ipsilateral head (63). The authors suggested that non-allodynic patients have peripheral sensitization, whereas allodynic patients have central sensitization of second-order brainstem trigeminal neurons as well. Later, the Burstein group (68) examined the effect of sumatriptan (subcutaneous injection), rizatriptan and zolmitriptan in patients with or without allodynia, using the same methods. This was performed since it is well established in several clinical trials that taking triptan early, when pain is mild, is more effective than waiting until the pain is moderate or severe (64). The study showed that within 2 h of triptan treatment, patients were pain free in 15% of allodynic attacks vs 93% of nonallodynic attacks (68). Treating migraine attacks 1 h or 4 h after the onset of pain was equally ineffective in inducing a pain-free state in the presence of allodynia, and equally effective in the absence of allodynia. The finding was later challenged in a multicenter, double-blind pilot study (69) that evaluated the prevalence of self-reported brush allodynia and its relative influence on the efficacy of almotriptan 12.5 mg combined with either aceclofenac 100 mg or placebo in 112 migraine patients. The study showed that allodynia numerically reduced treatment success overall, but this effect was not significant for the primary outcome measure, and multivariate logistic regression analysis confirmed that headache intensity at treatment intake, rather than allodynia, significantly influenced most outcome measures. Furthermore, another study showed that migraine headache intensity can be reduced within 1 h by zolmitriptan nasal spray in spite of the presence of early cutaneous self-reported allodynia (70). And in another study (71) allodynia (based on a questionnaire) did not influence the efficacy of almotriptan.
Cutaneous pain thresholds (CPTs) in trigeminal innervated areas are lower in migraine, eTTH, cTTH and MOH in comparison to healthy controls (65,72). Migraine patients interictally had lower pain thresholds for mechanical stimulation, higher pain scores in a temporal summation test and increased summation of pain for repeated mechanical and electrical stimuli compared to controls (72). Schwedt et al. (73) tested thermal and mechanical pain thresholds in 20 EM, 20 CM and 20 healthy controls. Thermal pain thresholds and thermal pain tolerance were lower in migraine patients than in healthy controls, but there was no difference between EM and chronic migraine. This is in contrast to a study investigating EM and chronic migraine using QST in eight locations interictally (bilateral ophthalmic, maxillary, C4/posterior neck, and forearm) that revealed that CM patients had lower pain thresholds than EM patients on the neck, arm and maxillary region (74). Interestingly, it has been demonstrated that there is a positive correlation between the time to next headache and low heat pain threshold at the head and arm (75). Nociceptive threshold decreases in healthy individuals following infusion of nitroglycerine, a donor of the signaling molecule nitric oxide (NO) (76), which is known to induce migraine in migraine patients (77) and is likely involved in migraine pathophysiology. This may reflect central facilitation of nociception by NO in migraine, but warrants further studies.
A recent study showed that MOH patients had lower cephalic/extracephalic pressure-pain thresholds, higher cephalic supra-threshold pressure-pain scores than controls and higher extracephalic supra-threshold pain scores for electrical stimulation than controls (78). Twelve months after successful detoxification, cephalic supra-threshold pain scores decreased in MO patients. Furthermore, temporal summation was not found in MOH patients before withdrawal, in contrast to controls, but after detoxification temporal summation normalized (78). Interestingly, MOH patients had significantly lower CPTs in the temple and cheekbone areas in comparison to the other headache groups (65), which suggests pronounced central sensitization in MOH patients.
In a mixed group of 25 CCH and ECH patients during active cluster periods and during remission, thermal and mechanical sensory function in the periorbital region was compared to 60 healthy volunteers (66). Perception of heat and pressure pain were reduced on the cluster side compared to the contralateral asymptomatic side and compared to healthy controls (66).
In TN, nine TN patients without prior surgery were compared to healthy controls in all six trigeminal branches (67). For all six trigeminal branches, warm sensation and heat pain thresholds were increased and cold sensation and cold pain thresholds were decreased in comparison to controls (except cold sensation on the contralateral side) (67). As part of a huge study on different neuropathic pain conditions, Maier et al. (4) performed standardized QST on 94 TN patients. In 87% of TN patients, the detection thresholds were abnormal in the pain area, when compared to the reference range of healthy controls or the contralateral side. Patients with abnormal signs were distributed with decreased thresholds (30%), increased thresholds (19%) or a combination of these (38%).
Other approaches to sensory testing in headache patients are discomfort thresholds, which have been tested for visual (79,80) and auditory (80,81) stimuli. Thus, quantitative measurement of sound-induced discomfort showed that migraineurs were significantly more sensitive than controls both during and outside an attack, and there were no differences between MA and MO. Using quantitative thresholds for discomfort and pain with monocular and binocular light stimuli, migraine patients were more photophobic during attack than outside attack, and they were more sensitive to light than controls between attacks (79). Again, no differences in light sensitivity between MA and MO were shown. CH patients have also been shown to be more sensitive to light and sound-induced discomfort than controls, but only during cluster periods (80).
In summary, allodynia is a feature of the migraine attack, but it is also found in other primary and secondary headaches and there is no apparent difference between chronic and EH subtypes. The studies differ greatly in methodology, and even differ in the definition of allodynia, which makes it difficult to conclude. QST can detect subclinical sensory abnormalities in TN patients despite absence of clinically evident neurological deficits (1).
Headache provocation models
Provocation studies migraine.

CGRP: calcitonin gene-related peptide; PACAP38: pituitary adenylate cyclase activating peptide-38; MA: migraine with aura; MO: migraine without aura.
Glyceryl trinitrate (GTN)-induced migraine-like attacks in 80% of migraine sufferers but not in healthy participants (74). Migraineurs developed a delayed headache fulfilling criteria for induced migraine attacks peaking 5 h after end of the infusion compared to 10% after placebo (79). Other groups validated the model and found it to be reproducible and reliable (83,101). Using GTN provocation on two separate days, the maximal headache response differed in less than 50% and only one of 10 headache scores in 40% of healthy individuals (102). Furthermore, headache characteristics were also reproducible (102) and the ability of GTN to induce migraine did not vary according to the frequency of attacks in migraine patients (103). GTN was given sublingually (0.9 mg) to 168 MO patients, 22 MA patients and 57 healthy controls. The test sensitivity was 82% in MO, specificity 96% and accuracy 86% (82). In MA sensitivity was 14%, specificity 96% and accuracy 72% (101). However, with IV infusion 50%–67% of MA patients develop an MO attack (83,85). In FHM types 1 and 2, two very rare dominantly inherited subtypes of MA, GTN did not induce migraine attacks (86,87). Thus, GTN induced only delayed MO attacks in some migraine subtypes, which gives important information about migraine pathophysiology, but may also be useful as a diagnostic tool when investigating different migraine subtypes.
GTN has not been used to differentiate between TTH subtypes, but it caused both immediate and delayed headache (104). The delayed type resembled the TTH phenotype (104). Measurements of muscle hardness, myofascial tenderness and pain thresholds during the immediate type headache were not different after GTN compared to placebo (104), suggesting that there was no peripheral or central sensitization during the immediate headache. Unfortunately, no measurements were taken during delayed headache.
CH attacks can be triggered during a cluster period using GTN and do not differ from spontaneous attacks (101,105,106). GTN sublingually (0.9 mg) during the active phase had a sensitivity of 80.6%, a specificity of 100% and an accuracy of 93%. If the CH group also included patients in remission phase, the sensitivity dropped drastically to 61.9% (101), Thus, GTN induces attacks predominantly during an active cluster period.
Calcitonin gene-related peptide (CGRP) is a potent vasodilator (107) in cerebral and extracerebral arteries (107). It can be released upon stimulation of the trigeminal ganglion (108). Lassen et al. (92) infused CGRP or placebo for 20 min in 12 MO patients in a double-blind crossover study. All patients experienced headache and three patients fulfilled ICHD-2 criteria for MO. Using newer criteria for migraine-like headache in experimental models (94), 50% experienced migraine-like attacks after CGRP compared to only one after placebo. The effect of CGRP in MA was later explored by Hansen et al. (91). CGRP induced MO attacks in 57% of MA patients (91). Just like GTN, CGRP does not induce FHM attacks (93,94).
Pituitary adenylate cyclase activating polypeptide-38 (PACAP38) is a vasodilator distributed in human sensory (109) and parasympathetic nerves and ganglia (110). In MO patients PACAP38 infusion induced migraine attacks in 58%–73% (97,98). Other signaling molecules and pharmacological substances well known to induce migraine in migraine patients are prostaglandin I2 (111), prostaglandin E2 (110), histamine (90), sildenafil (89) and cilostazol (101).
In summary, various pharmacological substances are able to induce primary headaches. It would be very interesting to investigate if these models can predict therapeutic outcomes and if they can be used to measure therapeutic responses. At the Danish Headache Center, we have a long tradition of conducting these infusion tests, which are done relatively easy with trained and skilled personnel, but we acknowledge that other countries may have challenges in performing these tests in terms of internal review board acceptance, approval of drugs for infusion and patient compensation.
Intracranial pressure (ICP)
In relation to secondary headache associated with cerebrospinal fluid (CSF) alterations, there are magnetic resonance imaging (MRI) signs associated with either idiopathic intracranial hypertension (IIH) or headache attributed to spontaneous low CSF pressure. However, in some case series 10% of IIH patients may have a normal MRI (112). A case series of 10 patients with IIH without papilledema (IIHWOP) investigated continuous CSF pressure monitoring (Pcsf) (113). All patients had normal resting Pcsf defined as ICP < 15 mmHg, but during sleep, all patients had B-waves and 90% had plateau waves or near plateau waves. Increased Pcsf was seen mostly during sleep and was intermittent, suggesting that Pcsf elevation may be missed by a single spot-check low pressure measurement. The similarity between IIHWOP and chronic daily headache (CDH) suggests that continuous Pcsf monitoring in CDH patients may have an important diagnostic role that should be further investigated.
In a case series of 40 patients with orthostatic headache and diffuse gadolinium pachymeningeal enhancement, 18% had opening pressures that were within normal limits (7–14 cm H20) (114). It has been suggested that a head-down tilt could be an accurate screening test for low CSF pressure in patients with daily headache (115). This would be an easy, inexpensive, noninvasive method that could be used before lumbar puncture with pressure measurement, radioisotope cisternography, CT or MR myelography or dynamic CT. A decrease in headache intensity during a 20-degree head-down tilt was seen in patients who had low CSF pressure (115).
Hannerz et al. investigated patients initially diagnosed with cTTH in three separate studies and found that 41%–68% had opening lumbar pressure of 20–25 cm H2O (116–118), which could point to headache attributes to IIH in non-obese patients according to the ICHD-2 criteria, but not the latest ICHD-3 criteria. CTTH patients in general had an increase in headache intensity following a 15-degree head-down tilt (116–118). In a recent study a surprisingly large number (43%) of patients diagnosed with medically refractory chronic migraine with normal MRI and no papilledema showed an opening pressure above 25 cm H2O (119). In 85 CM patients, 12% had increased ICP without papilledema, transient visual obscurations or visual fields (120) and in another study 61 CM patients, 5% had increased ICP without papilledema (121). Thus, some patients with chronic migraine may actually have unrecognized headache attributed to low or high CSF pressure. Furthermore, some patients with chronic headache may have normal fundoscopy but nevertheless an increased ICP (119).
In conclusion, measurement of ICP is very important in patients suspected of having IIH or low-pressure headache. A reasonable body of evidence suggests that it may also be worthwhile in patients with chronic headache, as some have increased pressure without papilledema. Monitoring pressure continuously improves such measurements, but this needs further validation.
Optical coherence tomography (OCT)—use in IIH
Headache may, but usually but far from always, remit after normalization of CSF pressure. Patients with IIH are normally followed by ophthalmologists who evaluate changes in visual field, degree of papiledema and changes in the optic nerve head (ONH) (122).
OCT is a noninvasive technique obtaining cross-sectional images of the internal retinal structures by measuring their optical reflections, as the nerve fiber layer (NFL) and retinal pigment epithelium (RPE) are highly reflective and thereby identifiable. Quantification of layer thickness is possible using computer algorithms. Various measures can thus be obtained such as peripapillary retina fiber layer thickness (RNFLT) and total peripapillary retinal thickness (TRT).
The diagnostic value of OCT was tested as a marker for CSF opening pressure in 20 newly diagnosed IIH patients and 21 long-term IIH patients who had previously been treated (123). OCT elevation diagrams showed that in 60% of newly diagnosed IIH patients and in 10% of long-term IIH patients, 50% or more of the OCT scans (TRT and RNFLT) were above normal. In a larger multicenter study comprising 126 IIH patients, RFNLT was more than 95% of normal controls in 90% of the IIH eyes (124). It has also been shown that RFNLT is associated with increased ICP in newly diagnosed IIH patients, but not in long-term IIH patients (123). The intraclass correlation between two scans on one day was 0.99 (125). RNFL thickness and visual field sensitivity losses was tested in 22 IIH patients with mild papilledema at diagnosis and three, six and 12 months after presentation in comparison to healthy controls (126). At diagnosis, the RNFL thickness was greater than in control eyes and greater in eyes with papilledema as well as significantly correlated with visual field sensitivity losses. At follow-up, the RNFL thickness decreased significantly, whereas the visual field sensitivity improved. Thus, RNFL thickness abnormalities correlated with visual field sensitivity losses. Another longitudinal study evaluated the clinical presentation and monitored a three-month course of treatment using OCT, visual field testing and lumbar opening pressure measurements in 17 newly diagnosed IIH patients in comparison to healthy overweight controls (127). Total average RNFLT and TRT decreased significantly during the follow-up period and changes in RNFLT and TRT correlated with improvements in visual field mean deviation. In a one-year follow-up study of 35 IIH patients, papilledema decreased rapidly within the first two months of diagnosis and OCT measures had normalized after one year (128). Despite this, 43% reported sustained chronic headache after one year, which indicates that the mechanism of headache is more complex than ICP elevation alone, and that headache and OCT-measured changes do not necessarily change in parallel. It is possible that some OCT parameters are better than others. Hence, one study compared RNFLT and peripapillary average retinal thickness (PART) measurements and showed that PART revealed the highest number of patients (n = 20) with optic disc abnormalities in either eye (90%) compared with 85%, 80% and 70% for RNFLT measurements, direct ophthalmoscopy, and fundus photography, respectively (129). It was suspected that increasing severities of papilledemas lead to an underestimation of RNFLT, which make PART more reliable. OCT still needs to be further analyzed and tested before it is accepted as a useful test in IIH patients.
Autonomic tests in primary headaches
In a German population-based sample an epidemiological study using questionnaires showed that 27% of migraine patients have accompanying unilateral autonomic symptoms (130). Several studies have shown dysfunction (both hypo- and hyperfunction) of the autonomic system in migraine patients, but no clear autonomic deficits have emerged from these studies (131). It would be of interest to compare migraine patients with or without autonomic symptoms using autonomic tests to elucidate whether they have different phenotypes, but, to our knowledge, this has never been performed.
The pupil dilates by sympathetic activity and contracts by parasympathetic activity. Miosis and ptosis during an attack indicate dysfunction of the sympathic innvervation, Horner’s syndrome. Seven out of 11 CH patients showed ocular signs of a postganglionic sympathetic lesion following an irritation test to the eye (120). Following corneal stimulation, ECH patients show reduced mydriasis bilaterally, but most pronounced on the pain side during but not outside the cluster period (132). Even with pain stimulation of extracephalic structures such as the sural nerve, pupil dilation was attenuated on the pain side during cluster periods but not during remission or in CCH (133). The cold pressor test (CPT) during and outside a bout showed absent miosis (134). Naloxone, an opioid-receptor antagonist, blocked miosis response in healthy controls but induced miosis in CH patients (134). This points to an oculocephalic sympathetic hypofunction in CH patients as well as an altered opioid neuromodulation (134). Thirty-eight ECH patients had significantly reduced average pupillary constriction velocity on the CH pain side compared to healthy controls. CH patients displayed bilaterally reduced pupillary average velocities, which indicates a bilaterally reduced cranial parasympathetic tone in CH patients in remission phase, with significant lateralization to the CH pain side (135).
Sweating can be measured by evaporimetry, by which water loss from the body surface can be measured rapidly and accurately (136). Thermoregulatory flushing and sweating are impaired on the pain side in CH patients (137), despite the fact that ipsilateral forehead sweating occurs during CH attacks (138). CH patients are also hypersensitive to acetylcholine analog pilocarpin on the ipsilateral side (137). Whether these findings may be useful in subcategorizing CH patients is not known.
Changes in heat loss can be measured by thermovision cameras as a marker of either sympathetic (cutaneous vasoconstriction, heat gain) or parasympathetic (cutaneous vasodilation, heat loss) changes. In 1984 thermography was recorded during 209 headache attacks both in migraine and TTH patients (135). During unilateral headache attacks, heat loss was found in the frontotemporal region on the pain side in patients with pain relief following superficial temporal artery (STA) compression. This thermographic asymmetry was abolished after pressure was applied over the STA. Throbbing headache was also associated with unilateral heat loss. Interestingly, 74% of patients with unilateral heat loss had headache response to ergotamine compared to 44% of patients without heat loss (139). No differences were found between migraine and TTH patients in terms of heat loss. Using thermography, it has been proposed that migraine patients have an area in the face with less heat loss on the pain side, which is also found interictally (140). This cold patch was later suggested to be a prognostic index marker in MA and CH patients as the cold patch was shown to be attenuated following successful treatment (141). However, a following validation study failed to show a similar pattern (142). In CH an ipsilateral heat loss in the orbital region in 63% of CH patients during attacks (143) was shown. Asymmetry in thermography seems to be a relatively sensitive but not a very headache phenotype-specific finding. Thus, in 1000 thermograms of headache patients, 85% of MO patients, 89% of MA patients, 86% of CH patients and 85% of post-traumatic headache patients had abnormal thermograms (defined as an arbitrary thermal difference of 0.5℃ between homologous regions of the face) compared to 13% of healthy controls (144). Based on the above, thermography does not seem to be of benefit in headache diagnostics, as the results so far have been unspecific.
Imaging in primary headaches
Over the last 10 years, imaging methods have been applied in primary headache research, especially MRI and positron emission tomography (PET). It is beyond the scope of this review to evaluate these methods in terms of phenotyping and diagnosis of primary headache using functional and structural imaging methods. PET and functional MRI studies have identified brain regions that might be responsible for mediating the onset of a migraine attack and those associated with migraine symptoms (145–148). Some resting-state functional connectivity MRI studies have identified brain regions and functional networks with atypical functional connectivity in migraineurs (149), but there is controversy as to whether these findings are truly specific for migraine (150). An interesting recent structural MRI study demonstrated that classifiers consisting of cortical surface area, cortical thickness and regional volumes were highly accurate for determining if individuals had migraine compared to healthy controls (68% accuracy) and whether migraine patients were episodic or chronic migraineurs (84% accuracy) (151). At the moment, these imaging methods cannot be easily applied as routine workup in the clinical setting, but it is possible that MRI could be implemented at tertiary headache centers and used to, on a single patient level, show specific biomarkers in primary headache, which could be valuable for diagnosis, prognosis and treatment response.
Discussion
We believe that headache classification and phenotyping should be enforced by laboratory tests, although it is still very early for such a new approach, and it has not yet been possible to demonstrate that it results in better patient management. This paper is therefore a manifesto and call for action to implement laboratory tests in the classification and management of primary and some secondary headaches. In the above, we have summarized current existing evidence about diagnostic tests that could be implemented in tertiary referral headache centers, and suggested how to start this development. At present, there is not an evidence-based strategy for implementing diagnostic tests, but this could be achieved if well-reputed tertiary headache centers start on developing and implementing laboratory tests.
Why are laboratory tests necessary? First of all, some tests already improve the classification of ICHD-3 beta headache categories. Most obvious is the genetic testing of FHM patients, even though the exact genetic diagnosis has not yet influenced the treatment of these patients. TTH is subdivided into a form with and a form without pericranial tenderness. This is recommended to be performed by manual palpation, as pressure dolorimetry has no proven value. With the existing knowledge discussed in this review, the distinction would be much better made if palpation were performed with PCP. Chronic headache may in some cases be caused by intracranial hypertension without papilledema. This diagnosis requires ICP measurement and, even better, ICP monitoring. The same is true of headache attributed to spontaneous intracranial hypotension. Secondly, primary headache disorders such as migraine and TTH are very prevalent and diagnoses are at present almost entirely based on the patient interview. Furthermore, the responses to acute and prophylactic treatment in these headache types are relatively low and variable (152,153). Migraine is known to be phenotypically quite heterogeneous, but despite this only MA is already subdivided into different types whereas MO, the clinically most frequent and important type of migraine, is not. MO is of complex inheritance. In addition, the high prevalence alone makes it very clear that MO is a heterogeneous disorder that should be subdivided. But how should this be accomplished? According to the presence or absence of autonomic symptoms, presence or absence of central sensitization, or according to response to provocation tests? We don’t know, but we must start to subdivide and analyze the differences between subgroups. A similar philosophy pertains to TTH. Also CH, new daily persistent headache, persistent headache attributed to traumatic injury to the head, MOH and TN would benefit from laboratory characterization and perhaps subdivision.
In this review we have not described genotyping of headache patients. So far, genome-wide association studies (GWAS) have not shown results that can be clearly tested in a clinical setting (154). Biomarkers such as levels of CGRP and PACAP and metabolomics may also be valuable, but results are not consistent and require in some cases sampling from the jugular vein and are therefore not suitable in a clinical setting. Patient symptom reporting instruments may also be valuable, but their use is outside the scope of this review as they can hardly be regarded as laboratory tests.
To perform laboratory tests requires resources and how to get them will vary widely among countries and regions as well as among publicly financed programs and privately insured patients. It seems unlikely that funding will be available in one place for the whole program suggested below. But we hope that some centers will evaluate one or more tests, while other centers may evaluate other tests. To commence this, there is a necessity for laboratory space, laboratory equipment and personnel to perform the tests. This requires hospital administrations to accept that this is a new way of analyzing headache patients, which takes some time and financial effort to be successful or else it must be funded by grants. This could perhaps be achieved in a multicenter collaborative consortium funded by the European Union (EU) or National Institutes of Health (NIH). Our ideal is that once the best facilities are in place, it should be possible to refer new patients for the lab tests suggested below, and that the tests will be described much like a radiological or a neurophysiological test.
The suggested disease-specific test programs are based on the review given above; we suggest the following tests be carried out in the following headaches:
Conclusion and recommendations
We conclude that several diagnostic tests may be ripe for implementation in academic headache centers. It is likely a lack of resources that prevents this from happening. We strongly urge that leading headache centers worldwide try to create facilities allowing such laboratory diagnoses to be made. Such laboratories also have to scientifically evaluate the suggested as well as other tests because the diagnostic value is not yet clear enough. We believe that laboratory-enforced diagnoses will improve the recognition of headache disorders as an important part of neurology and thereby increase interest in headache disorders among neurologists. At the same time, the further exploration of diagnostic and therapeutic tests for headache patients presents exciting possibilities for original research.
Key findings
The present review is a call for action to implement laboratory tests in the classification and management of primary and some secondary headaches. The palpometer test, quantitative sensory testing, nociceptive blink reflex and autonomic tests may be valuable to phenotype and/or diagnose subforms of primary headaches, trigeminal neuralgia and medication overuse-headache. A number of laboratory tests in headache research are presently available, but have primarily been performed in single research studies or a few studies that differ in methods and patient groups. At present, there is no evidence-based strategy for implementing diagnostic tests.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.