
Abstract
Nitroglycerin administration provokes spontaneous-like migraine attacks in migraine and cluster headache (CH) patients. Nitroglycerin-induced migraine-like headache has been used as an experimental model of migraine. In this paper, we evaluate the possibility of using the nitroglycerin provocative test (NPT) as a supportive measure in the diagnosis of primary neurovascular headaches by assessing its reliability on a large population and adopting strict criteria for rating the response as positive or negative. Our population consisted of 197 migraineurs, 42 subjects suffering from cluster headache and 53 healthy controls. In migraine without aura, the test sensitivity was 82.1%, specificity 96.2% and accuracy 85.5%, while in subjects suffering from migraine with aura, the reliability of the NPT was less satisfactory (sensitivity 13.6%, specificity 96.2% and accuracy 72%). In CH patients tested during the active phase of the disease the sensitivity was 80.6%, specificity 100% and accuracy 92.9%. NPT is an easy, low-cost and reliable method for supporting the diagnosis of migraine without aura and cluster headache.
Introduction
Administration of nitroglycerin, a nitric oxide donor, provokes spontaneous-like migraine attacks in migraine patients evaluated during an intercritical phase (1). In 1987, Sicuteri et al. (2), referring to their clinical practice over the years, reported two clinical types of headache response to nitroglycerin in migraineurs. The first response appeared a few minutes after nitroglycerin administration, was short-lived and characterized by diffuse pain, while the second occurred with a latency of several hours and presented with the same pain characteristics as spontaneous attacks. Some years later, nitroglycerin-induced headache was systematically evaluated in migraineurs and healthy controls in a double-blind placebo-controlled study, which substantially confirmed Sicuteri's practical observation (3, 4). Nitroglycerin-induced headache in migraine patients was also found to fulfil, in most cases (5), the diagnostic criteria of the International Headache Society (IHS) (6).
Several reports suggest that nitroglycerin induces spontaneous-like attacks in cluster headache (CH) patients, too (7–11). All of the above-mentioned studies were substantially in agreement as regards the capability of nitroglycerin administration to provoke headache attacks showing the same characteristics as the patient's primary headache (migraine or CH), in a considerable percentage of sufferers. However, since these studies were based on small populations, no consistent conclusions could be drawn about the reliability of the nitroglycerin test as a diagnostic tool for migraine or CH. In addition, only in the case of migraine were the characteristics of nitroglycerin-induced headache found to correspond to the IHS criteria for the disorder (6).
In the present report we evaluated the headache response to nitroglycerin in a large population of migraineurs, CH sufferers and healthy controls. Strict criteria were adopted for rating the response as positive or negative, and the reliability of the nitroglycerin provocative test (NPT) as a diagnostic tool for primary neurovascular headaches was calculated in terms of its specificity, sensitivity and accuracy.
Materials and methods
Subjects
One hundred and ninety-seven patients suffering from migraine (175 without and 22 with aura) and 42 patients with CH (29 episodic and 13 chronic) fulfilling the respective IHS criteria were included in the study. Fifty-three healthy subjects were evaluated as controls (Table 1).
Population characteristics
Consecutive first-referral patients were recruited at the outpatient headache clinic of the Headache Centre of the University of Pavia, IRCCS ‘C. Mondino’ Foundation Institute of Neurology. All underwent a general physical examination and a neurological examination. They were asked to keep a diagnostic headache diary over a 12-week run-in period. The diagnosis was made by an experienced clinician. The nitroglycerin test was performed at the end of the 12-week run-in period by a trained neurologist, who was blind to the diagnosis.
For migraine without aura, the inclusion criteria were: the occurrence of at least two attacks/month in the last 3 months; the ability to distinguish between migraine and tension-type attacks, if both headaches were present; the absence of medication overuse for headache. Given the sporadic occurrence of attacks in patients suffering from migraine with aura (12), patients with this latter form of migraine were not required to have a precise monthly or yearly attack frequency in order to be included in the study, only that their history include at least two attacks fulfilling the IHS criteria for migraine with aura. The monthly frequency of attacks (± sd) in our headache population is shown in Table 2. Five of the migraine with aura patients enrolled in the study also suffered from migraine without aura. In these 5 patients, the monthly frequency of attacks of migraine without aura was lower than that observed in the group of patients suffering from ‘pure’ migraine without aura (migraine with and without aura: 3.1 ± 2.7 attacks/month; pure migraine without aura: 6.7 ± 5.5 attacks/month; P < 0.001).
Frequency of attacks in our headache population (mean ± sd). Frequency was calculated on the basis of attack occurrence during the last three months for migraine without aura (MO), the last year for migraine with aura (MA), the last month for chronic cluster headache and the last active period for episodic cluster headache

Thirty-six patients in the migraine group also suffered from tension-type headache, episodic in 22 cases, chronic in 14. These 36 migraineurs were perfectly able to distinguish between the two types of headache they suffered from. No analgesic overuse for headache was present in any of the patients suffering from both migraine and tension-type headache. The healthy subjects had never had a migraine or a CH attack and experienced fewer than 6 headache days/year. These occasional headaches were very infrequent tension-type headaches or secondary forms related to a transient cause, i.e. fever, hangover, cold stimulus, etc.
All the subjects gave their informed consent to participate in the study, which was approved by the local Ethics Committee and conducted in accordance with the declaration of Helsinki.
Procedures
The tests were started between 0800 and 0900h at the headache centre's day hospital facility. Before the provocation test, patients and controls were informed that there was the possibility that the drug they were going to take might induce a headache attack, whose characteristics would have been recorded at serial time-points on a questionnaire.
For a period of 20 min, during which the subjects became acquainted with their surroundings, the patients/controls rested comfortably in supine position in a silent room. They then received nitroglycerin sublingually (0.9 mg, Pharmafar srl). The participants stayed at the hospital for at least 8 h after nitroglycerin administration. Headache characteristics were noted on an ad hoc report form at 15-minute intervals during the first hour and then at 30-minute intervals for the following 7 h. This report form made it possible to compare the usual characteristics of spontaneous attacks, as reported by the patients, with the characteristics of nitroglycerin-induced headache (pain location, quality and intensity, and associated symptoms) at each time point. If headache occurred, the patient was asked to state whether it was identical to his/her spontaneous attacks. In addition, he/she was asked to climb a few stairs in order to investigate the possibility of headache aggravation by routine physical activity. Arterial blood pressure was measured at 15-min. intervals for the first 1 h.
At the time of the test, patients had to be pain-free. Analgesic or triptan intake was discontinued at least 24 h before testing in migraine patients, and at least 12 h before testing in cluster headache patients. A low percentage of patients (2%) were on prophylactic treatment at the time of their clinical evaluation. In these subjects, the NPT was performed one month after the prophylactic treatment had been discontinued. In female patients suffering from perimenstrual attacks, NPT was performed at least 3 days before or after their menses.
Patients and controls who developed a moderate to severe headache were treated with nonsteroidal anti-inflammatory drugs, triptans and/or antiemetics after at least 4 h had elapsed since the headache onset.
Data analysis
The three possible clinical scenarios following nitroglycerin administration in patients and controls were: (i) no headache (ii) specific headache, and (iii) nonspecific headache.
In order to be rated specific, nitroglycerin-induced headache had to:
fulfil the IHS criteria for the patient's primary headache type (or for any type of primary neurovascular headache in controls);
be deemed (by the patient himself/herself) identical to spontaneous attacks;
occur within 8 h of nitroglycerin administration.
Non-specific headache, on the other hand, was defined as a headache that:
did not fulfil the IHS criteria for the patient's primary headache type (or for any type of primary neurovascular headache in controls) and;
was judged by the patient himself/herself to be different from spontaneous attacks.
Patients suffering from migraine with aura were analysed separately from the group of patients suffering from migraine without aura. The specificity of their response was matched first with the criteria for migraine without aura and second with the criterion for migraine with aura (fulfilment of the IHS criterion for aura).
Irrespective of their specificity, nitroglycerin-induced headache responses were additionally differentiated into two subtypes: immediate, when occurring within 60 min of nitroglycerin administration (13), and delayed, when appearing between 61 min and 8 h after nitroglycerin administration.
The NPT was considered positive when it induced an immediate or delayed specific headache, and negative when it induced no headache or a non-specific immediate and/or delayed headache.
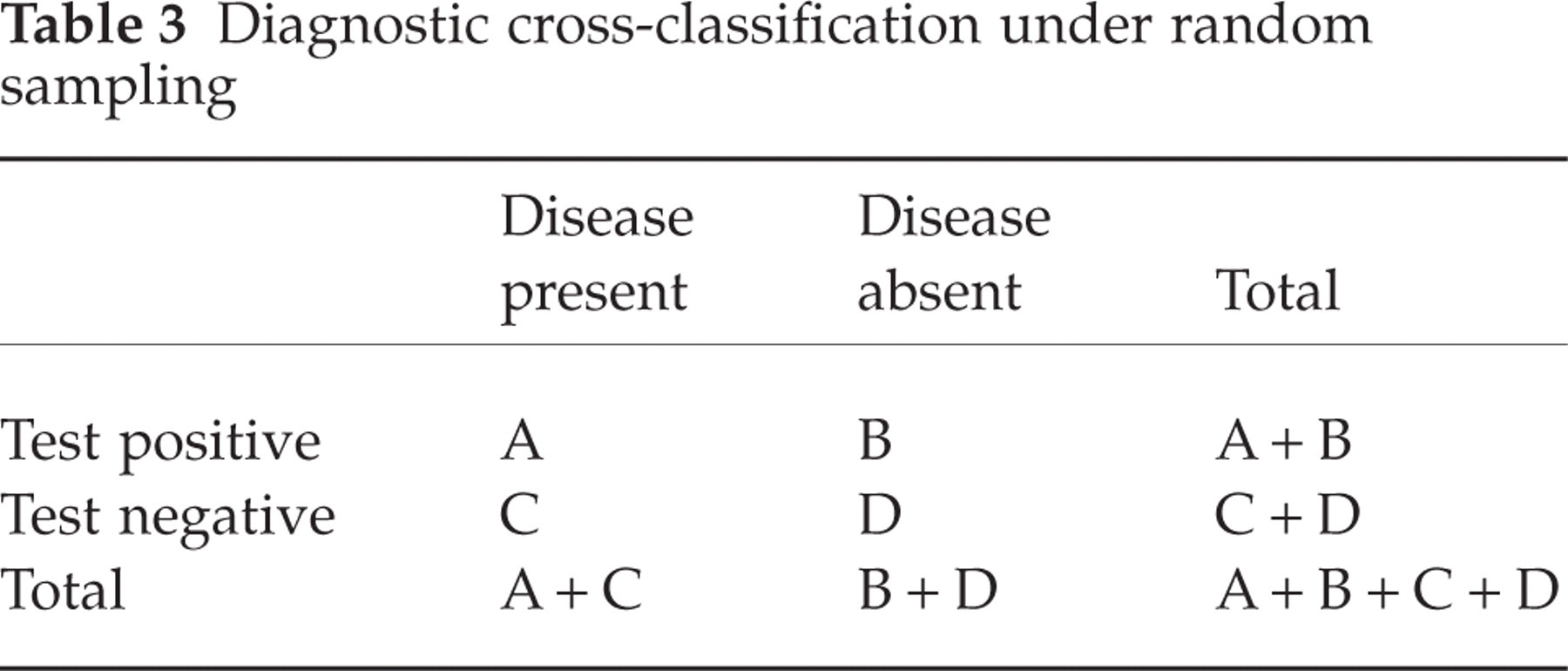
Sensitivity, specificity and accuracy of the NPT (Table 3) were defined using conventional definitions. The sensitivity of a test expresses the probability that it will be positive in a subject that is affected by a given disease. The corresponding formula is as follows: sensitivity = true positive/true positive + false negative = A/(A + C). Specificity expresses the probability that the test will be negative in a subject not affected by a given disease. The corresponding formula is: specificity = true negative/false positive + true negative = D/(B + D). The formula for accuracy is true positive + true negative/total tests performed = A + D/A + B + C + D.
Diagnostic cross-classification under random sampling
The time at onset of the specific headache response to nitroglycerin was recorded, and its distribution along the 8 h observation period evaluated.
Of the 175 tests performed in patients suffering from migraine without aura, 7 could not be included in the analysis due to lack of clinical and/or experimental data.
Results
Nitroglycerin was generally well tolerated by patients and controls. In just a few cases (2% of subjects), the drug induced a symptomatic reduction in recumbent systolic blood pressure, marked enough to cause prefainting symptoms within 30 min of its administration. In all cases, the symptomatology promptly disappeared upon leg raising.
Migraine without aura
During the first 60-minute observation period, 28 (16.7%) of the 168 patients suffering from migraine without aura did not develop any headache, 57 (33.9%) developed a specific response and 83 (49.4%) a non-specific headache. Over the following 7 h, 30 (17.9%) were headache-free, 131 (78.0%) continued to experience or developed a specific response and 7 (4.1%) had a non-specific headache. The total number of patients who developed a specific (immediate and/or delayed) headache in response to NPT was 138 (82.1%). The mean time to onset of the specific headache response was 136.4 ± 130.4 min Fig. 1a illustrates the distribution of the onset latency of the specific response in migraine without aura patients during the 8 h observation period.
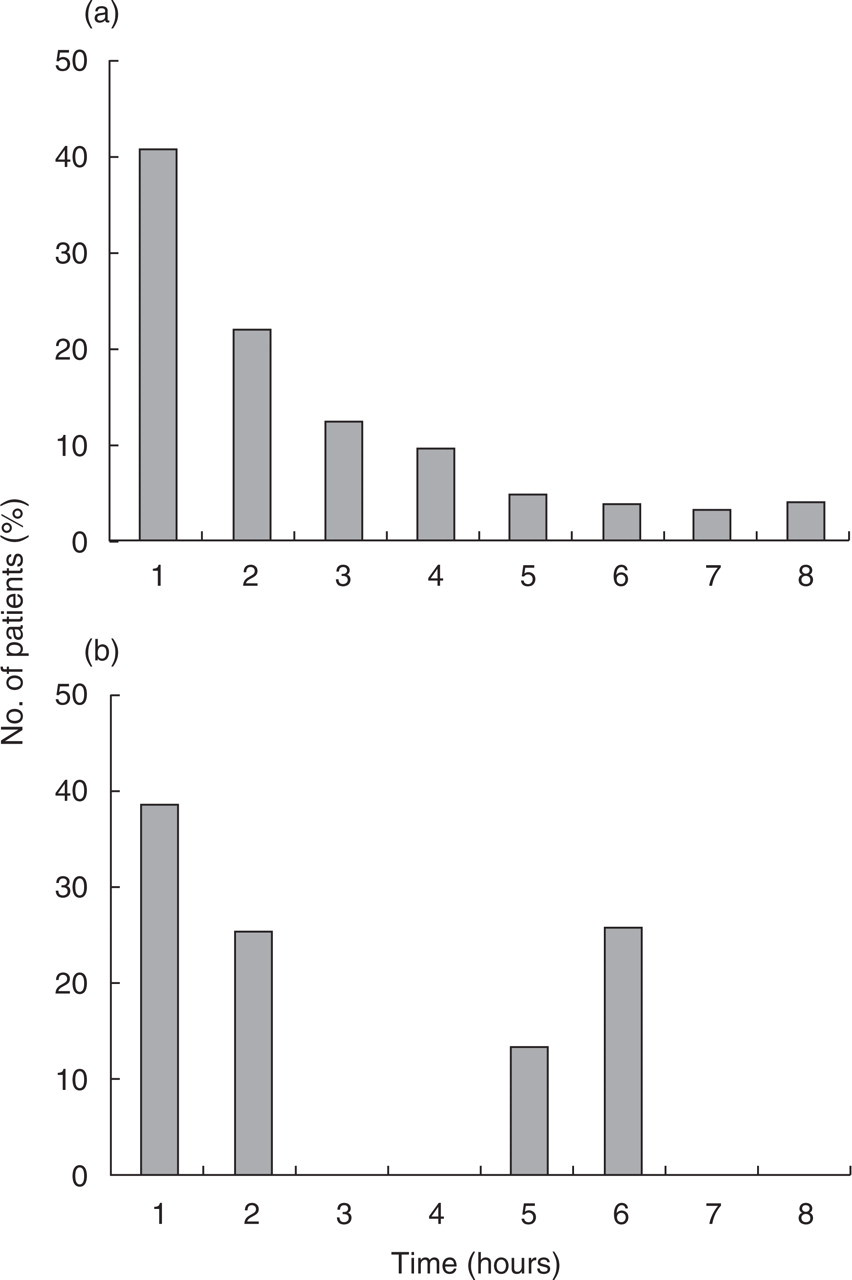
Time distribution of specific response to the NPT in patients suffering from migraine (a) without and (b) with aura. χ2 test: ns.
Phono- or photophobia was reported in 84% of patients with a positive response to NPT, moderate to severe nausea in 78%, and vomiting in 32%. Patients experiencing a specific response to NPT showed a higher monthly frequency of attacks compared to patients who developed a nonspecific headache or no headache at all (Fig. 2).

Monthly frequency of attacks in patients suffering from migraine without aura on the basis of their response to the NPT. Student's t-test: P < 0.01.
Migraine with aura
During the first 60-minute observation period, 10 (45.4%) of the 22 migraine with aura patients did not develop any headache, 4 (18.2%) developed a specific response for migraine without aura and 8 (36.4%) a nonspecific headache. Over the following 7 h, 13 (59.1%) did not develop any headache, 7 (31.8%) continued to experience or developed a specific response for migraine without aura and 2 (9.1%) had a non-specific headache.
The total number of patients who developed a specific (immediate and/or delayed) headache for migraine with aura in response to NPT was 3 (13.6%). The aura reported was of the visual type, consisting of phosphenes and/or scotomas, and in all cases it mimicked the spontaneous aura. Six additional subjects developed a specific response for migraine without aura (27.3%).
The mean onset latency of the specific headache response was 134.4 ± 133.0 min, which did not differ from the time to onset of the specific response observed in the group of patients suffering from migraine without aura. The distribution of the onset latency of the specific response is shown in Fig. 1b (migraine without aura vs. migraine with aura; χ2 test: ns). No relationship was found between positive response and frequency of attacks or time elapsed since the last attack.
Cluster headache
During the first 60-minute observation period, 21 (50.0%) of the 42 patients suffering from CH did not develop any headache, 18 (42.9%) developed a specific response and 3 (7.1%) a non-specific headache. Over the following 7 h, 34 (80.9%) did not develop any headache, 8 (19.1%) developed a specific response, while no patient developed a non-specific headache. The total number of CH patients who developed a specific (immediate and/or delayed) headache in response to the NPT was 26 (61.9%). However, if we exclude 11 of the CH patients, who were tested during a remission phase, and restrict the analysis to the group of CH patients evaluated during the active period, the rate of patients that developed a specific response rises to 80.6% (specific response in 25/31).
Of the 8 patients who developed a specific delayed response, one experienced a spontaneous-like headache 60 min, one 70 min, two 90 min, one 120 min, one 150 min and two 180 min after nitroglycerin administration. In none of these delayed attacks was the time at which the nitroglycerin-induced response occurred found to correspond to the typical timing of spontaneous attacks. The mean onset latency of the specific headache response was 65.4 ± 54.7 min, a period significantly shorter than the mean time to onset observed in the migraine group (Student's t-test, P < 0.0001).
Figure 3 illustrates the distribution of the onset latency of the specific response during the 8-h observation period.

Time distribution of specific response to the NPT in patients suffering from cluster headache (a) during the 8-h observation period and (b) during the first hour.
Controls
During the first 60-minute observation period, 37 (69.8%) of the 53 healthy controls did not develop any headache; no control subject developed a specific response for a primary headache, while 16 (30.2%) developed a non-specific headache. Over the following 7 h, 49 (92.5%) did not develop any headache, 2 (3.75%) developed a headache response that fulfilled the criteria for migraine without aura, and 2 (3.75%) developed a non-specific headache response. Of the two subjects who developed a specific migraine-type headache in response to the NPT, both (two males) had a positive family history of migraine (see genealogical trees in Fig. 4).

Genealogical trees of the two male control subjects (no. 3, upper panel and no. 11, lower panel) who developed a headache specific for migraine without aura in response to the NPT.
Sensitivity, specificity and accuracy of the NPT for primary neurovascular headaches
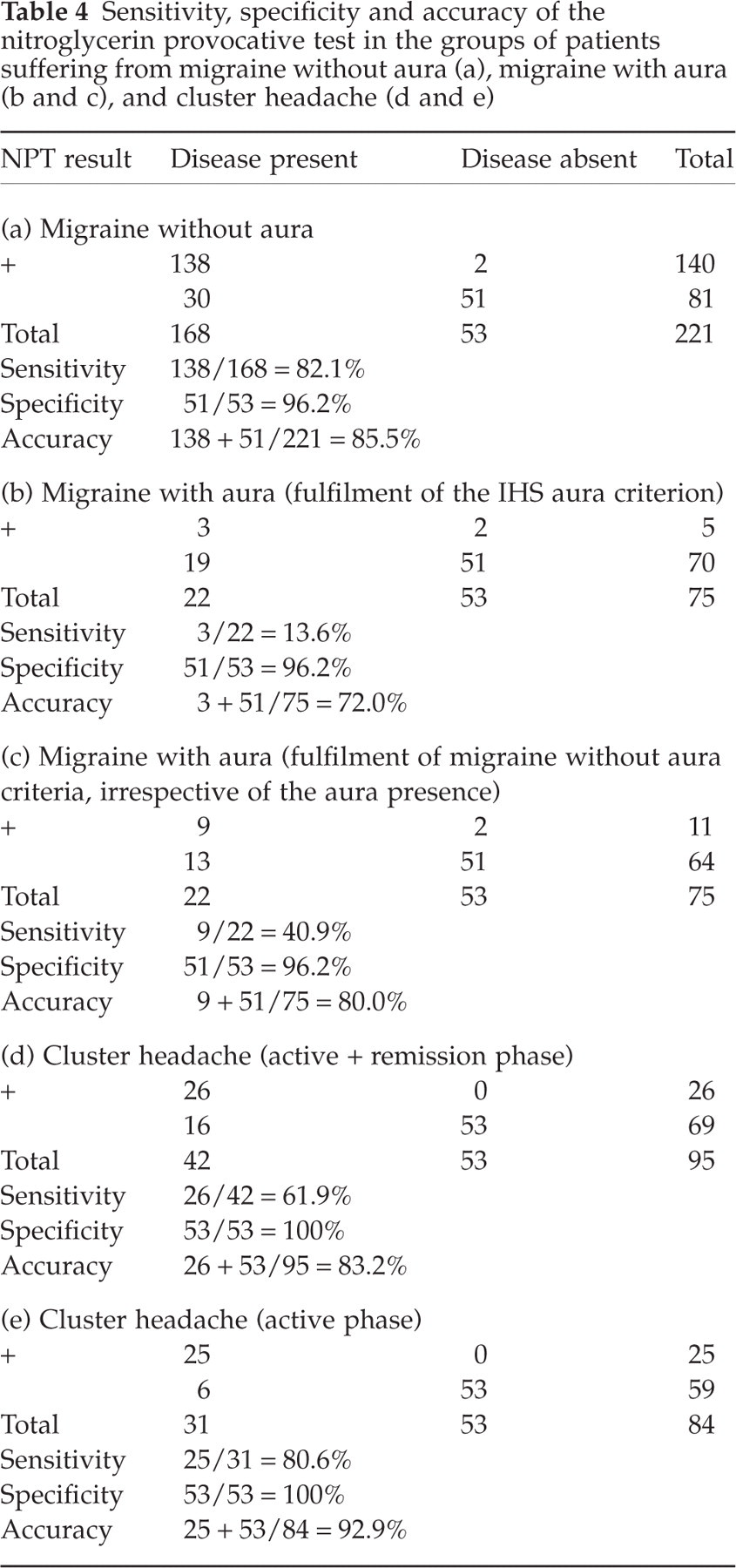
The sensitivity, specificity and accuracy of the NPT for the different types of primary headache evaluated, calculated on the basis of the results of the NPT in patients and controls, are illustrated in Table 4.
Sensitivity, specificity and accuracy of the nitroglycerin provocative test in the groups of patients suffering from migraine without aura (a), migraine with aura (b and c), and cluster headache (d and e)
Discussion
Migraine is a frequent disorder that is becoming an increasing part of the workload of neurologists, while CH is a rare disease that is frequently misdiagnosed. At present, diagnosis of these headaches is totally subjective, relying on fulfilment of IHS criteria, which are based on the patient's history, and on the exclusion of other known causes. There are as yet no gold standard objective tests for the diagnosis of primary headaches, nor any reliable biological markers.
Several reports, conducted on small numbers of patients, suggest that nitroglycerin administration consistently evokes spontaneous-like headache responses in patients suffering from migraine and CH (1–5, 7–11). In the present study, we evaluated a large population of primary neurovascular headache sufferers, matching them with a statistically comparable number of healthy controls. The findings obtained show that the NPT has a fairly high sensitivity for migraine without aura as well as for CH when patients are evaluated during a cluster period. Conversely, the sensitivity of the test was found to be poor in patients suffering from migraine with aura and in CH patients studied during a remission phase. In both migraine and CH, irrespective of the type (without or with aura) and the period (active or remission), the specificity of the NPT is very high: >96% for migraine and 100% for CH.
The higher specificity of the test observed in migraine without aura compared to migraine with aura patients is possibly related to the higher attack frequency in the former group. This hypothesis is further supported by the data reported in Fig. 2. If we add to this observation the demonstration that the NPT has, in agreement with previous reports (7, 9), a higher specificity in CH patients studied during an active phase, we can speculate that the closer the NPT is to the last attack, the more likely it is to be positive. This pattern would seem to fit in perfectly with the condition of central sensitization hypothesized by several authors.
In this study, we chose to enrol first-referral patients, which probably conditioned the inclusion of subiects with a low number of attacks in the group of migraine with aura. Indeed, migraine with aura usually presents with sporadic attacks and subjects experiencing painful attacks preceded by negative or positive neurological symptoms are likely to seek early medical help. It will be of considerable interest to determine the rate of positive response to NPT in patients with a higher frequency of migraine with aura attacks in future studies.
The present findings regarding the higher positivity of the NPT in patients with a higher monthly rate of migraine without aura attacks conflict with previous data by Christiansen et al. (13), where no difference in the occurrence of headache in response to nitroglycerin was observed between migraine without aura patients experiencing frequent attacks and those experiencing rare attacks. However, a direct comparison between the two studies is not warranted since the group of patients with frequent attacks in the population studied by Christiansen had a mean of 16.2 attacks/year, which is a much lower frequency than that observed in our migraine population.
The possibility that a portion of patients with a higher monthly frequency of attacks might have developed a spontaneous one must be taken into account. However, all precautions were taken to avoid the occurrence of a spontaneous attack: from the 24 h interval from the last analgesic/triptan intake (to avoid rebound headaches or recurrence) to the avoidance of the menstrual period in female patients with a perimenstrual recurrence of attacks. In the case of CH, the occurrence of spontaneous attacks seems less likely since, in most patients, the attack occurred within 60 min from nitroglycerin administration and in no case the nitroglycerin-induced attack occurred at the usual timing of spontaneous attacks.
The present findings unequivocally point to the capability of nitroglycerin to induce spontaneous-like attacks in both migraine and CH patients, and thus support the hypothesis that nitric oxide is an important common denominator in the pain mechanisms of both forms. The significantly different latencies of onset of the specific response, however, seem to suggest that a differential cascade of events is initiated by nitric oxide in these two neurovascular headache syndromes. Recently, Ashina et al. demonstrated that nitroglycerin is capable of inducing spontaneous-like attacks in patients suffering from chronic tension-type headache (14, 15), which suggests that nitroglycerin-derived nitric oxide may act by increasing a pre-existing central sensitization in tension-type headache, a mechanism similar to that already hypothesized for migraine and cluster headache (14, 16–21). Thus, it seems that nitric oxide is a common mediator of pain mechanisms in primary headaches. Conversely, the low sensitivity of the NPT in the induction of migraine aura, in agreement with previous findings (22), suggests that nitric oxide is unlikely to be involved in the initiating mechanisms of the aura phase.
It is noteworthy that the two healthy subjects who developed a specific response for migraine had a positive family history of migraine. This finding is in agreement with previous observations by Sicuteri et al. (2) and might represent an indirect demonstration of the ability of NPT to unmask not only the disease, but also simple predisposition to it.
On the basis of the present findings, the subdivision of the headache response to nitroglycerin into immediate and delayed is superfluous. In addition, no consistent support has emerged for the view that the specific response to nitroglycerin is the delayed one, as in many cases, the specific headache response appeared within the first 60-min period.
Two other important methodological issues have been addressed by the present data: the dose and route of administration. Several studies describing the headache response to nitroglycerin were based on the i.v. infusion of the drug (3–5). In these studies, the total drug dose varied from patient to patient, the infusion being discontinued when the headache developed. In other studies, a fixed, sublingual dose was administered (8, 11). In the present study, we opted, on the strength of decades of clinical experience accumulated (since 1969) at our headache centre, for the sublingual administration of a fixed dose of nitroglycerin. Another reason for this choice was the fact that a standardized NPT, with a fixed dose of a sublingually administered drug, seemed to provide a more simple and suitable tool for the potential widespread application of the test in hospital as well as outpatient settings. The findings regarding the sensitivity and specificity of the NPT confirm the appropriateness of both the dose and the route of administration adopted, although at this time we cannot rule out the possibility of a higher sensitivity of the test with other dosages and routes.
The implications of the present study are multiple and extend to several fields, from the clinical-diagnostic setting, to legal and work-related disputes. Migraine and CH attacks are characterized by specific signs/symptoms that are vital for a correct diagnosis. These accompanying features are nausea, vomiting, phono and photophobia in the case of migraine (23), periocular and/or nasal autonomic signs in the case of CH (24). The NPT proved able to evoke these associated symptoms, in addition to the pain component, in a high percentage of patients. In the case of migraine without aura, the percentage of patients with a positive response to NPT who developed nausea, vomiting, phono and photophobia is similar to the percentage of patients who report the same symptoms during spontaneous attacks (25). This is an indirect demonstration of the accuracy of the NPT. In the case of CH, 100% of patients with a positive response to NPT showed periocular or nasal autonomic signs. It follows that the test could contribute to the correct diagnosis of these two forms of primary headache, especially in patients who lack (or cannot recall) the necessary anamnestic information. In these cases, administration of the NPT could help to reduce the time to diagnosis and would eliminate the need to monitor, through the filling in of headache diaries for several weeks (26), the occurrence and characteristics of attacks.
Another important point regarding accompanying symptoms is that some of them can be witnessed objectively. The identification of a diagnostic test able to confirm the presence of a primary headache form by evoking objective features of the disorder will hopefully have positive repercussions for both the patient and the physician.
The capacity of the NPT to evoke consistently objective markers of the disease should prove useful in efforts to complete the delicate process of getting primary headaches ranked alongside other neurological disorders (thereby removing them from the ‘dumping ground’ of undefined and totally subjective disorders, where they have too long remained, and freeing them from the stigma that goes with this lack of status).
Finally, our data have important implications for the field of headache research. A considerable number of pathophysiological and therapeutic advances obtained in the last decade in migraine and CH research have been based on the study of attacks experimentally induced with nitroglycerin (27, 28) or on the use of experimental animal models of nitroglycerin administration (19, 29–37). The demonstration that nitroglycerin induces spontaneous-like attacks in a statistically significant population of neurovascular headache sufferers lends further weight to the evidence obtained through these human and animal models and will hopefully stimulate additional research in this direction.
In conclusion, the present findings indicate that the NPT is an easy, low-cost, safe and reliable method that offers high diagnostic accuracy, and as a result will prove helpful in supporting and confirming the diagnosis of migraine and CH. Its routine application could have positive implications for primary headache sufferers in health, social and work settings. The demonstration that nitroglycerin-induced headaches are actually identical to spontaneous primary headache attacks provides further clues as to the nature of the common pathophysiological mechanisms underlying migraine and CH.
Footnotes
Acknowledgements
This work was supported by a grant from the Italian Ministry of Health (RC 2002)