
Abstract
Background and objective
Unlike migraine and migraine with aura, little information exists regarding chronic migraine (CM) as a risk factor for cardiovascular disease. In this study we aim to determine whether an association between CM and endothelial dysfunction exists.
Methods
Individuals 18 years and older diagnosed with episodic migraine (EM) and CM according to ICHD criteria were studied. After an overnight fast and abstinence from vasoactive drugs, ultrasound studies were performed and blood samples taken from patients and matched controls according to internationally agreed on protocols.
Results
A total of 113 individuals were enrolled (35 CM, 37 EM, 41 controls). CM patients had a lower percentage of flow-mediated vasodilation (FMD; difference of means = 5.03%; p = 1.0E-6) and breath-holding index (BHI; difference of means 0.754; p = 2.0E-6), as well as increased carotid intima media thickness (cIMT; difference of means = 0.128 mm; p = 7.0E-5) than controls. The EM patients and controls comparison found similar, but less pronounced, differences: decreased BHI (p = 0.031), and increased cIMT (p = 0.028). Fibrinogen (r = 0.277; p = 0.006), C-reactive protein (r = 0.288; p = 0.003), and erythrocyte rate sedimentation (r = 0.298; p = 0.002) also correlated with cIMT, and inversely with BHImV and FMD.
Conclusions
Migraine is associated with systemic and cerebral endothelial dysfunction demonstrated by ultrasound studies and biological markers. The degree of these changes was strongly associated with the severity of migraine. Our data indicate that migraine may be a cerebral disorder with systemic endothelial damage.
Keywords
Introduction
Migraine is a common disease, affecting approximately 12% of the population, with a predominance of females affected. According to the World Health Organization, migraine was the 19th leading cause of years lived with disability for both sexes, and the 12th for women, irrespective of age (1). In our region (Cantabria, Spain), chronic migraine (CM) has an estimated prevalence of 2.5% in the general population and has a greater socioeconomic cost and burden for health care systems compared to other forms of migraine (2,3). The underlying mechanism for how episodic migraine (EM) leads to CM has not been elucidated, but some CM risk factors such as obesity (4), snoring and sleep apnea (5) and excessive medication use (6) have a common feature in that they may damage vasculature. The full pathophysiology of migraine is incompletely defined; however, the consensus is of the neurovascular hypothesis being the most likely explanation as it combines both neurogenic and vascular mechanisms.. The association between migraine and vascular disease is supported by numerous epidemiological studies that demonstrate migraine patients to have a higher risk of developing vascular events such as ischemic stroke and myocardial infarction (7). Furthermore, patients with migraine are subject to higher cardiovascular mortality (8). In recent years, it has been proposed that migraine patients have endothelial dysfunction (9), although it is possible that either cerebral or systemic endothelial dysfunction alone or both together are present in migraine patients. Likewise, the role that cerebral and systemic endothelial function plays in headache chronification remains unknown. The presence of endothelial damage in EM and CM patients, in the absence of clinical manifestations, has been suggested from ultrasonographic studies. There exist controversial results regarding cerebral arterial responses to different stimuli, as well as a possible association between systemic vasculature and migraine. The finding of fewer circulating endothelial-precursor cells in migraine patients when compared to non-migraine patients suggests the presence of broader vascular damage (10).
The aim of this study is to assess the association between migraine and cerebral and systemic endothelial dysfunction, as well as arterial stiffness. We hypothesize that the ultrasonography changes are more relevant and persistent in CM patients, and that these findings have pathophysiological implications for migraine. We analyzed serum inflammatory markers, as some are known to be increased in migraine patients (11), and therefore have the potential to function as markers of non-specific endothelial activation.
Methods
Study population
Initially, patients who fulfilled the International Classification of Headache Disorders, second edition (ICHD-II) criteria for EM and for CM (2006 revision (12)) were recruited from the University Hospital Marqués de Valdecilla in Santander, Spain, from March 2013 to January 2015. As this study coincided with the publication of the ICHD, third edition (beta version) (13), the criteria for migraine with (MwA) or without aura (MoA) and those for CM were re-applied. Individuals were selected from a patient database of more than 3000 migraine sufferers. All participants selected agreed to participate in the study. Healthy volunteers (controls) were recruited among the staff of the hospital and patients’ friends. Controls and EM and CM patients were matched according to sex and age (approximate proportion 1:1:1). This study was approved by the local institutional research and ethics committees, and all participants gave written informed consent.
The major exclusion criteria for patients and controls were: under 18 years or over 65 years, a body mass index (BMI) lower than 18 kg/m2 or higher than 35 kg/m2, a history of cardiovascular disease (including ischemic coronary artery disease, cerebrovascular accidents, peripheral arteriopathy or heart failure), Raynaud’s syndrome, systemic inflammatory conditions, a history of cancer, chronic kidney disease, pregnancy or lactation, diabetes mellitus, active hypertension or hypercholesterolemia, and heavy smoking (defined as smoking more than five cigarettes/day). Individuals with excess consumption of caffeine (more than three cups/day), analgesic (more than 15 days/month) or triptan (more than 10 days/month) were also excluded. People with prior hypertension or hypercholesterolemia were permitted to participate, provided the disease had resolved without medication. Additionally, patients and controls were required not to be taking statins, antihypertensives, nitrates or antiepileptic drugs, at the point of study entry. Smokers were instructed to avoid smoking at least 24 hours before ultrasonographic studies. The diagnosis of migraine subtype was corroborated in subsequent visits using a headache diary that recorded pain intensity, predominant pain side, presence of aura, nausea, vomiting, pulsatile quality, and abortive medication used. Twelve individuals were excluded from the analysis because of the absence of a temporal sonographic window.
Study protocol
All studies were performed between 8 a.m. and 11 a.m., after an overnight fast (>8 hours). Participants were free of exposure to vasoactive medications and caffeine intake at least 24 hours before. None of the patients were using prophylactic antimigraine medication for at least one week and none had taken analgesic drugs for 72 hours before examination. All studies were performed in a temperature-controlled room (22 ℃).
Measurement of blood pressure (BP) and the drawing of blood were performed at the moment of ultrasonographic study. To assess the levels of inflammatory markers, blood levels of C-reactive protein (CRP), lipoprotein A, apolipoprotein B, fibrinogen and erythrocyte sedimentation rate (ESR) were measured.
Methods for ultrasonographic studies
Ultrasonographic methods are described in detail in the Supplementary material. Briefly, the recommendations of the International Brachial Artery Reactivity Task Force (14) were followed for flow-mediated vasodilation (FMD), by measuring dilation in response to increased flow due to reactive hyperemia. Carotid intima media thickness (cIMT) measurements were performed using high-resolution B-mode ultrasound with a 10 MHz linear transducer, at 1 cm proximal to the carotid bifurcation in the posterior wall of the common carotid artery. Using a 2 MHz transducer placed on the temporal bone window, the middle cerebral artery (MCA) was insonated at a depth ranging from 50 to 55 mm, following a standard protocol, as well as for the basilar artery through the suboccipital window. The breath-holding index (BHI) was calculated as the percentage increase in mean blood flow velocity (MBFV) occurring during breath holding, divided by the time (seconds) for which the participant held breath. This method has recently been introduced and has been shown to be at least as effective as methods requiring CO2 inhalation (15).
Statistical analysis
Data are presented as mean ± standard deviation (SD). For comparisons among the three groups, one-way analyses of variance (ANOVAs) with the Bonferroni multiple comparison test were used for continuous values, and the χ2 test was used for categorical variables (α = 0.05). Mean values of cIMT, BHI and FMD were compared between pairs of groups using Student’s t test. For cIMT, BHI and FMD, univariate correlations with plasmatic endothelial markers, and clinical variables were analyzed using Pearson’s correlation coefficients. To identify independent predictors of cIMT, BHI and FMD, variables showing correlation p-values <0.10 were entered into a multiple linear regression model. SPSS software (SPSS 21.0, SPSS Inc, Chicago, IL, USA) was used for the analyses.
Sample size was calculated using means and SDs from BHI, FMD and cIMT, a 95% power and an α = 0.01. From this power calculation, 35 participants in each group were regarded as a requirement for this study.
Results
Clinical study (see Supplemental material and Table 1)
Epidemiologic, clinical, ultrasonographic, and biochemical data among clinical groups.

Ns: not significant; NA: not applicable; ApoA: apolipoprotein A; ApoB: apolipoprotein B; ESR: erythrocyte sedimentation rate; CRP: C-reactive protein; BMI: body mass index; cIMT: carotid intima media thickness; FMD: flow-mediated dilation or endothelium-dependent vasodilation; BHI: breath holding index; LDL: low-density lipoprotein.
Chi2 distribution with 2 degrees of freedom, except for preventives (1 df).
Not active.
Fewer than five cigarettes/day.
Ultrasonography study (see Table 1 and Supplementary material)
At the moment of this study, only two individuals showed abnormal BP (systolic BP > 140 mm, or diastolic BP > 90). No participants had smoked or taken alcohol during the 24 hours preceding ultrasonographic examination.
Large vessels findings
No differences were found in MBFV in the cervical vessels among clinical groups (see Supplementary material).
cIMT
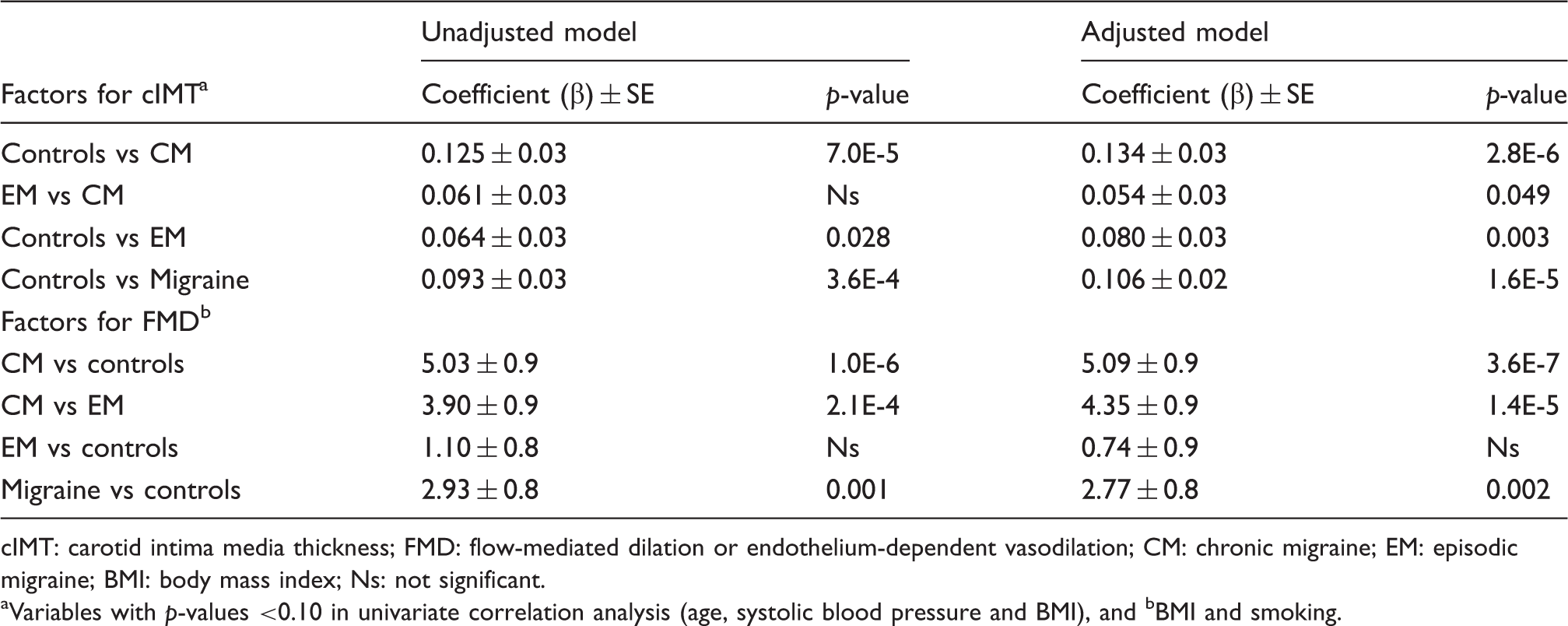
The cIMT was increased in migraine patients compared to controls (ANOVA F = 9.959; p = 1.0E-4) (Table 1). Table 2 shows the linear regression model. In the unadjusted model, the difference of means of cIMT between CM and controls was 0.128 mm (p = 4.6E-5), and between EM and controls was 0.075 mm (p = 0.030). The cIMT was lower in EM than in CM patients (p = 0.223), although this was not statistically significant (Figure 1(a)). The cIMT was significantly correlated with systolic BP (r = 0.200; p = 0.048), age (r = 0.280; p = 0.003) and BMI (r = 0.240; p = 0.013) but not with diastolic BP. Total cholesterol did not correlate with cIMT (r = 0.095; p = 0.337). In the model adjusted for systolic BP, age and BMI, the headache diagnosis was the best predictor for the cIMT (p = 1.3E-5) (Table 2). Based on marginal means, post hoc analysis revealed that EM (β = 0.080 ± 0.03; p = 0.030) and CM (β = 0.134 ± 0.03; p = 2.8E-6) were the best predictors for cIMT (power = 0.998; Table 2).
Box plots showing median, fifth, 25th, 75th and 95th percentiles from (a) carotid intima media thickness (cIMT) and (b) flow-mediated vasodilation (FMD), and (c) breath-holding index (BHI) among controls and headache groups. Plots show that the chronic migraine group displays the highest cIMT, and lower FMD and BHI. For comparisons among groups, corrected p-values are indicated. Significant predictors of cIMT and endothelial-dependent vasodilation (FMD), according to linear regression models, crude and adjusted for confounding factors. cIMT: carotid intima media thickness; FMD: flow-mediated dilation or endothelium-dependent vasodilation; CM: chronic migraine; EM: episodic migraine; BMI: body mass index; Ns: not significant. Variables with p-values <0.10 in univariate correlation analysis (age, systolic blood pressure and BMI), and bBMI and smoking.
Endothelium-dependent vasodilation
FMD was decreased in migraine patients compared with controls (ANOVA F = 15.625; p = 1.0E-6). FMD and cIMT showed an inverse correlation (r = –0.371; p = 0.0001). The unadjusted model showed that CM patients had decreased FMD values compared both to controls (β = 5.03 ± 0.9; p = 1.0E-6) and EM patients (β = 3.09 ± 0.03; p = 2.1E-4); FMD values in EM and controls did not differ. Univariate correlation analysis of FMD and vascular risk factors were not significant, although some trends were found for BMI (r = –0.178; p = 0.076) and smoking (r = –0.189; p = 0.054). FMD values inversely correlated with systolic BP (r = –0.285; p = 0.006) but not with diastolic BP. Therefore, these variables were entered into the linear regression model (Table 2). In the adjusted model, headache diagnosis was the best predictor for FMD (F = 15.1; p = 2.0E-6), and smoking remained significant (F = 5.5; p = 0.021), but not BMI. Post hoc comparisons among clinical groups revealed that CM patients had lower FMD value than controls (β = 5.09 ± 0.9; p = 3.6E-7) and EM patients (β = 4.35 ± 0.9; p = 1.4E-5. Table 2). Preventive treatment did not influence FMD among migraineurs (p = 0.20).
Cerebral vasoreactivity (CVR)
Comparisons of breath-holding index using ANOVA one-way statistic.

BHI: breath-holding index; MCA: medium cerebral artery; R: right; L: left; DF: degree of freedom; ANOVA: analysis of variance.
Subanalysis of participants with no classical vascular risk factors
The subanalysis was performed in 24 controls, 14 EM, and 22 CM patients who had no cardiovascular risk factor and cIMT values less than 1.0 mm. In this subset, comparisons among clinical groups were significantly different for cIMT (p = 0.001), BHI (p = 2.0E-4) and FMD (p = 6.7E-6).
Preventive treatment did not affect cIMT (F = 0.990; p = 0.323), FMD (F = 0.562; p = 0.456) or BHI (F = 0.001; p = 0.979).
Influence of aura in ultrasonographic results
No differences among EM and CM were observed for cIMT or BHI with respect to the presence or absence of visual aura. However, FMD was lower (difference of means = –3.24) in EM patients with visual aura compared to those without aura (p = 0.024).
Discussion
In this study, we focused on the endothelial damage in migraine patients, investigating both the cerebral and the systemic changes associated with endothelial dysfunction. Our main findings indicate that migraine is an independent factor for cIMT, FMD and BHI. Increased cIMT, the first step in atherosclerosis, correlated with the severity of migraine. Thus CM patients had higher cIMT values compared to EM patients and controls—although the difference was significant only when compared to controls. CM patients also had lower FMD values compared to EM patients and controls, suggesting that peripheral vascular reactivity is decreased in migraine with more disability. It is worth mentioning that FMD values did not differ between EM patients and controls. CVR, assessed by use of the BHI, was significantly decreased in migraine patients. CM patients also showed lower FMD and BHI than in EM patients. Therefore, we have observed that endothelial dysfunction is more frequent and severe in CM than in EM, regardless of other vascular risk factors. These common vascular risk factors were not present at the point of study entry. We permitted participants with occasional smoking habits and previous elevated BP or hypercholesterolemia only if these factors were controlled without medication.
We assessed CVR in the anterior and posterior cerebral circulation, and also vasoreactivity in the non-cerebral arteries. Systolic BP correlated with cIMT and FMD, but not with BHI. This suggests that, at least in young people with a normal BP, BHI in cerebral arteries remains independent of BP. The studies of BHI in MA or MoA patients have shown inconsistent results. Akgün et al. in 2014 found reduced BHI in CM patients in the interictal state, but only versus controls (16). Corretti et al. in 2002 did not find differences between controls and EM, but the BHI was lower (∼50%) in cases during the migraine attack than in the interictal period (14). Contrary to our results, studies performed by Dora et al. have shown hyperreactivity to hypercapnia was found in MwA only, in a study in which MwA and MoA showed increased MBFV versus controls before treatment (17), and in another study, with only MoA patients (18). Treatment with flunarizine demonstrated inconsistent results when measuring the BHI (18,19). Silvestrini et al. reported that only the basilar artery showed decreased BHI in MwA (20), which contrasts with the Arjona et al. study that showed that MoA cases had higher time-averaged mean velocity, but not BHI, than controls (21). Vernieri et al. found increased CVR in the predominant pain side versus the other side in migraine patients, as well as compared with controls; such a correlation also occurred with total hemoglobin content and oxygen saturation (22). Likewise, the number of T677 alleles of methylene-tetrahydrofolate-dehydrogenase inversely correlated with BHI in migraine patients (23). Just like in our data, in this study the presence or absence of aura did not influence BHI. Contrary to the observation that systolic BP inversely correlated with FMD in the latter study, our results suggest that CVR is independent of BP, at least at the normal BP range here explored.
The cIMT has extensively been used to identify subclinical atherosclerosis. We found a strong correlation between CM and cIMT. To the best of our knowledge, this is the first study that assesses the potential risk of developing high cIMT as an expression of atherosclerosis disease in CM patients. We have observed that cIMT strongly correlated with those parameters of vasoreaction both in the central nervous system and peripherally in the brachial artery. In migraine patients and controls without cardiovascular risk factors (including cIMT < 1.0 mm) Perko et al (24). did not observe any correlation between CVR to L-arginine in the MCA and FMD, and the posterior cerebral artery and FMD. Nevertheless, they found a higher rate of curve elevation in controls compared to migraineurs in the analysis of correlation between CVR and L-arginine. Therefore, they postulated as did Rajan et al. (25) that endothelial function in the cerebral circulation differs from systemic circulation under physiological conditions and in migraine. They also hypothesized that migraine is unlikely to induce an increase of cIMT. In contrast, we have used a different endothelial stimulus, sustained apnea. We also found a strong correlation between peripheral and cerebral endothelial function, and these variables were inversely correlated with cIMT. Altered functional arterial properties outside the brain in migraine patients indicate that migraine pathophysiology involves other non-neural mechanisms, e.g. decreased interictal endothelium-dependent vasodilation (26,27). Nevertheless, there are some discordant reports (28,29). In the latter study, FMD was similar in steady state and after infusion of calcitonin gene-related peptide (CGRP), serotonin and sodium nitroprusiate in a case-control study with a very low number of participants. These differences might be attributed to methodological issues. There are some factors that could modify vascular reactivity (i.e. smoking, diet, drugs, among others) and these must be taken into account when creating a regression model.
It is important to highlight the controversial theory suggesting that migraine is a systemic vascular disorder. Several studies have found not only higher cerebrovascular events in migraineurs, but also a higher frequency of coronary, retinal and peripheral vascular events (9). MwA has been found to be especially associated with cardio- and cerebrovascular events, but these studies included common vascular risk factors, and most of them did not assess cIMT (7,30). We adjusted our results for these common confounders, including cIMT, and we found consistent peripheral and cerebrovascular endothelial dysfunction associated with migraine in general, and especially with CM.
We have analyzed other nonspecific laboratory markers of inflammation such as ESR, CRP and fibrinogen, which correlated with higher values of cIMT, and lower values of BHI and FMD. Therefore, in this study, cerebral and systemic endothelial dysfunction may well be linked to inflammation.
It has been debated whether migraine is an independent vascular risk factor, or whether other factors commonly associated with atherosclerosis were more prevalent in migraineurs. In a population-based survey Bigal et al. (8) associated MA and MoA with both cardiovascular disease and common vascular risk factors. Our results agree with this observation since we observed that migraine is an independent factor for endothelial dysfunction. On the other hand, Stam et al. (31) failed to demonstrate an association between migraine and atherosclerosis, measured by means of cIMT, pulse wave velocity, and ankle-brachial index. Nevertheless, they found migraineurs more likely to smoke, to have diabetes mellitus and to exhibit decreased high-density lipoprotein (HDL)-cholesterol, which could mask the possible effect of migraine itself on cIMT or vascular parameters. However, in contrast to our study, the latter study corresponds to a population-based survey, in which EM patients were predominant. Moreover, our EM patients were selected from a headache unit, and they showed higher Migraine Disability Assessment (MIDAS) scores than expected in the general population.
There are other studies that have assessed the endothelial damage associated with systemic inflammation. González-Juanatey et al. (32,33) have indicated that cIMT inversely correlated with FMD in different clinical settings of rheumatoid arthritis (RA). However, progression of cIMT could depend on other clinical, predictable complications. This is the case in systemic lupus erythematosus (34). Current treatment of RA with anti-tumor necrosis factor alpha (TNF-α) monoclonal antibodies appears to have beneficial effects on the progression of atherosclerosis, suggesting that tight control of systemic inflammation may slow progression of the vascular disease (35). This issue could also account for migraine if we may prevent more effectively progression to CM.
Strengths and limitations of this study
Although we have matched the sample for sex and age, other variables with potential influence on the main variables could introduce bias, given the complexity of the study using three groups. Nevertheless, we have selected participants without active vascular diseases and who abstain from vasoactive drugs. We have used corrected p-values for multiple testing and calculated marginal means adjusted for confounding variables. The BHI possesses some limitations, especially in patients with learning difficulties, as some collaboration is required. Other authors preferred CO2 or nitric oxide (NO) donors to achieve the vasodilation. To avoid possible bias we instructed participants prior to entering the study to perform the apnea to a satisfactory standard. Furthermore, infusion of vasodilators can be problematic, as this can provoke headache, nausea or vomiting, and thus influence test results (36).
The lower BHI and FMD values, as well as the higher cIMT values in migraine patients compared to controls, lead us to conclude that migraine is associated with general (cerebral and systemic) endothelial dysfunction. These results were independent of blood lipids, BP, smoking habits and age. Interestingly, the degree of these vascular alterations was strongly correlated with the severity of the disease measured by MIDAS and by the frequency of attacks.
Article highlights
Chronic migraine patients have increased carotid intima media thickness independent of age, smoking habits, body mass index, and hypertension. Altered vasoreactivity was found both in intracerebral and systemic arteries in migraine patients, especially in chronic migraine. We found a strong correlation of endothelial dysfunction with erythrocyte sedimentation rate, C-reactive protein and fibrinogen, suggesting that our findings were related to inflammation.
Footnotes
Acknowledgement
We are indebted to Andrew Shala for style revision.
Funding
This work was supported by ISCIII-FISS Pi11/1232, Pi08/387, Novartis, and IDIVAL.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr A. Oterino has received honoraria for speaking from Allergan, Biogen Inc, Teva, and Merck. Dr Vicente González-Quintanilla has been awarded by IDIVAL the grant “Wenceslao-López Albo.” All other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.