
Abstract
The relationship between migraine and blood pressure is controversial. We studied the association between migraine and blood pressure in a population-based sample of elderly patients. Participants were 1373 subjects 59-71 years of age. Lifetime migraine was diagnosed according to the International Headache Society criteria by a headache specialist. Blood pressure was measured as well as the carotid intima-media thickness (IMT) which is a good marker of the long-term exposure to high blood pressure. Migraine during life was diagnosed in 140 participants. Mean systolic blood pressure was lower in subjects with migraine than in those without headache (128 mmHg vs. 137 mmHg). There was a significant trend of decreasing frequency of migraine with increasing blood pressure and also with increasing IMT. In this study, migraine was associated with lower levels of blood pressure and with smaller values of carotid wall thickness.
Introduction
The relationship between migraine and blood pressure is controversial. Several studies have suggested that there is an association between hypertension and headaches (1–4), although others, including two recent reports, found no association (5–10).
Most of these studies were done before the introduction of the International Headache Society (IHS) criteria for the diagnosis of migraine (11) or used a modified version of the IHS criteria (9). Furthermore, very few were performed on large population-based samples.
We studied the association between migraine and blood pressure in a population-based sample of elderly participants. We also studied the relationship between migraine and carotid intima-media thickness (IMT) which is a marker of blood pressure history.
Patients and methods
Study design and migraine assessment
The EVA (Epidemiology of Vascular Ageing) study has been described in detail elsewhere (12, 13). Briefly, it is a longitudinal study of cognitive and vascular ageing, which recruited men and women born between 1922 and 1932 from the electoral rolls of the city of Nantes, France. At baseline all participants were administered a standardized questionnaire used to collect information about demographic background, occupation, medical history, drug use and personal habits such as cigarette and alcohol consumption. Depression was defined as a history of depressive symptoms confirmed by a medical doctor and treated with antidepressant drugs (14). With respect to smoking behaviour, subjects were classified as never smoker, former smoker, or current smoker. Total daily intake of alcohol was estimated in millilitres according to the average number of millilitres of ethanol in a glass of each type of alcoholic beverage. Then, frequency of daily alcohol consumption was categorized as ‘never’, ‘less than 20 ml’, ‘20 ml or more’.
The migraine study was performed during the second follow-up visit, which took place 4 years after the baseline visit and involved 1188 participants. The participants were first systematically asked about recurrent attacks of headaches during their life as part of the general questionnaire. The participants who answered yes to the screening question had a phone interview with a headache specialist. Migraine assessment was performed with the use of a structured questionnaire reproducing the items of the IHS criteria (11). This questionnaire was previously tested and showed a high reproducibility (15). Instructions were given to the expert to obtain a lifetime history of headaches by asking participants questions about headaches in their young adulthood. The expert was blinded to all clinical and laboratory data concerning the participants. Written informed consent was obtained from all participants and the study was approved by the Ethics Committee of the Hôpital de Kremlin-Bicêtre in Paris.
Blood pressure measurement
Two independent measurements of systolic blood pressure (SBP) and diastolic blood pressure (DBP) were made with a digital electronic tensiometer (SP9 Spengler) after a 10-min rest and the means were used for analysis.
According to The Sixth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC VI) (16), participants with a SBP ≥ 140 mmHg or DBP ≥ 90 mmHg were classified as having high blood pressure. Those who had high blood pressure or were taking anti-hypertensive medication were considered as hypertensives. SBP and DBP were also studied separately as continuous and categorical variables. Categories of SBP and DBP were defined according to the JNC VI classification: <120 mmHg, 120–139 mmHg, and = 140 mmHg for SBP and <80 mmHg, 80–89 mmHg, and = 90 mmHg for DBP. Strata with higher values of SBP or DBP were not considered because they would include a limited number of patients with migraine.
Ultrasound examination
Details of the protocol have been described elsewhere (17). All measurements were made at the time of examination. It involved scanning of the common carotid arteries, the carotid bifurcation and the origin (first 2 cm) of the internal carotid arteries. The IMT was measured on the far wall of the mid and distal common carotid artery as the distance between the lumen–intima interface and the media–adventitia interface. Both near and far walls of all arterial segments were scanned transversally and longitudinally. The mean of the right and the left IMT was used in the analysis.
Statistical analysis
We first compared participants with migraine with participants without recurrent headaches on various demographic variables and vascular risk factors. From this univariate analysis we identified potential confounding factors. In multivariate analysis with logistic regression models we estimated the relationship between migraine, blood pressure, and IMT. Strata of SBP and DBP were defined according to current consensus on blood pressure and for IMT we used tertiles. Risk of migraine in patients with high blood pressure was also estimated in strata of various potential confounders in order to verify the consistency of the association. Because of the higher frequency of migraine in women, all analyses were adjusted for sex. Alternative strategies including stratification on gender were deemed inadequate because of the relatively small number of men with migraine. Five percent level of significance and 95% confidence intervals were used. All analyses were performed with the SAS® statistical package (SAS version 8.02 for Windows. SAS Institute, Cary, NC).
Results
Migraine was diagnosed in 140 participants, including 120 women and 20 men, and non-migrainous recurrent headaches in 93. Those who did not complain of having had recurrent attacks of headaches during their life (n = 946) were considered as headache free (Fig. 1). Participants with migraine had the same mean age, were more frequently women, had more frequently a history of depression, and were less frequently ex- or present drinkers than participants without recurrent headaches (Table 1). With regard to blood pressure, participants with migraine had a lower mean SBP than those without (128 vs. 137 mmHg; P = 0.002), a lower pulse pressure, and a lower mean DBP, although the difference was not significant for the latter. A high blood pressure was less frequently observed in participants with migraine, with a sex- and age-adjusted odds ratio (OR) of 0.59 [95% confidence interval (CI) 0.39, 0.89; P = 0.012]. The previous definition of high blood pressure (SBP ≥ 160 mmHg or DBP ≥ 95 mmHg) gave similar results (adjusted OR = 0.39, 95% CI 0.18, 0.86; P = 0.019). Anti-hypertensive drug use and frequency of hypertension were similar in participants with and without migraine (Table 1). Carotid IMT was lower in participants with migraine than in headache-free participants (6.8 mm vs. 7.1 mm; P = 0.008). Both groups had a similar frequency of carotid plaques. There was no significant difference between participants with migraine and those without recurrent headaches concerning other vascular risk factors like diabetes, tobacco consumption, total cholesterol, LDL- and HDL-cholesterol, fibrinogen, and C-reactive protein level (data not shown).
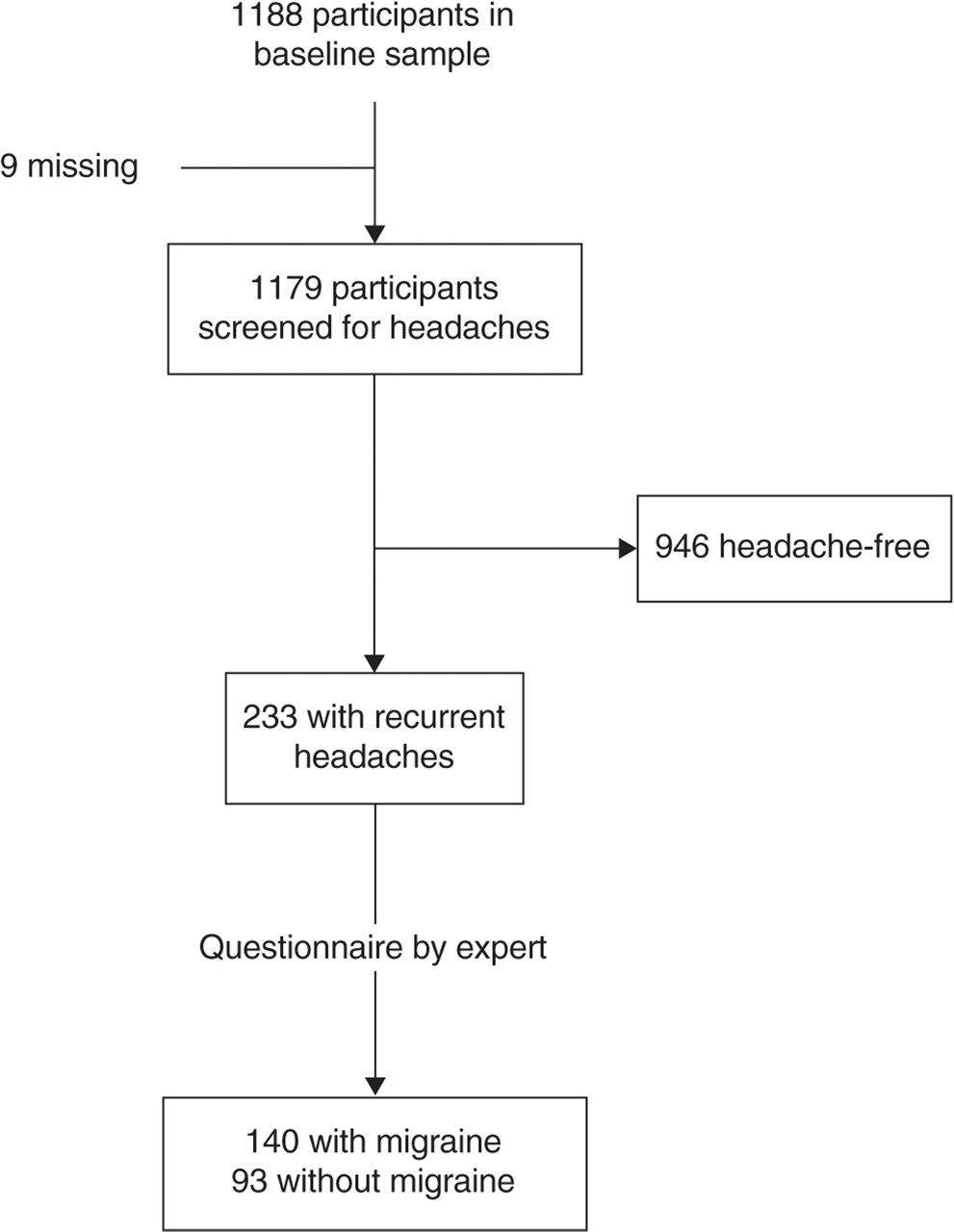
Flow chart of the diagnosis of migraine in the EVA study.
General characteristics of headache-free and migraine participants

∗Adjusted for age and sex.
†Body mass index computed as weight (in kg) divided by the height squared (in meters).
‡Defined as a systolic blood pressure> 140 mmHg or a diastolic blood pressure> 90 mmHg.
§Defined as patients with a high blood pressure or being under anti-hypertensive treatment.
To analyse further the relationship between migraine, blood pressure, and IMT, we compared the frequency of migraine in strata of these variables (Table 2). There was a highly significant trend of decreasing frequency of migraine with increasing SBP. After adjustment for sex, age, alcohol and history of depression, the risk of migraine was reduced by 56% in participants with a SBP = 140 mmHg compared with those with SBP < 120 mmHg (Table 2). With regard to DBP, the risk of migraine was lower in those with higher values of DBP, although the difference and the trend were not significant. There was a significant trend (P = 0.001) of decreasing frequency of migraine with increasing carotid IMT. After adjustment, the association with migraine seemed to be limited to the higher values of carotid IMT (Table 2).
Association between systolic blood pressure, carotid intima-media thickness and migraine

∗Adjusted for sex, age, alcohol consumption, and history of depression.
†Reference category.
Finally, we analysed the consistency of the relationship between migraine and a high SBP. For that we estimated the risk of migraine in high (SBP = 140 mmHg) vs. low systolic blood pressure (SBP < 140 mmHg) in strata of various variables which could act as confounders or effect modifiers: sex, age, alcohol consumption, history of depression, anti-hypertensive drug use and more specifically β-blocker use (Table 3). In all strata the risk of migraine in patients with a high SBP was lower than one, although not always significantly. There was no significant interaction between strata for any of these variables. The association between migraine and high SBP was apparently stronger in men, in the youngest, in never drinkers, in those without a history of depression, and in anti-hypertensive users.
Association between migraine and high blood pressure (SBP > 140 mmHg) according to potentially influencing variables

OR, Odds ratio; CI, confidence interval.
∗Age- and sex-adjusted.
Discussion
In this population-based study, we found that participants with migraine had lower values of SBP. The risk of migraine was more than halved in participants with a SBP = 140 mmHg compared with those with a SBP < 120 mmHg (adjusted OR = 0.44, 95% CI = 0.27, 0.75). Accordingly, participants with migraine had hypertension less frequently, although the difference with headache-free participants was not significant.
The relationship between blood pressure and headaches has always been controversial. Some previous studies suggested that there was a close relationship between headaches and high blood pressure (2, 18, 19), while there was no relationship for others (5–7). All these studies were done before the publication of the IHS criteria and most were based on self-report of high blood pressure and migraine. However, even more recent studies have also led to conflicting results (3, 4, 9, 10).
The present study has some major strengths. It has a population-based setting, participants were therefore not selected on the existence or type of headaches or on their blood pressure level. Great care was taken in the diagnosis of migraine, which was performed by a headache specialist blinded to all other aspects of the study (20). After screening, all participants with recurrent headaches were interviewed by the expert and migraine diagnosis was based on a validated structured questionnaire reproducing the IHS criteria. Blood pressure was measured in a standardized manner with automatic devices. These standardized procedures for the recruitment of participants, the diagnosis of migraine, and the measurement of blood pressure make very unlikely that the inverse relationship between migraine and blood pressure could be explained by selection or misclassification biases. Two recent studies with large samples have also suggested that headaches and migraine could be associated with low blood pressure (9, 10). One of these studies, performed in a population-based sample of 1174 individuals over 17 years of age carefully assessed with regard to headaches, also found a lower blood pressure in participants with migraine (10). However, the present study is the first in which consistent results on carotid IMT have been reported. IMT is a marker of vascular profile and, particularly, of long-term exposure to blood pressure (21). IMT was found to be lower in participants with migraine compared with headache-free participants, which is consistent with the observation that patients with migraine have a lower blood pressure. Compared with the simple point-estimate of blood pressure, this result on IMT provides strong evidence to rebut an association between migraine and hypertension and, conversely, to support the inverse relationship between migraine and blood pressure.
In this study we also had the opportunity to examine the role of potential confounders or risk modifiers such as sex, age, alcohol consumption, depression, and intake of anti-hypertensive drugs. All these variables have been found to be associated with migraine and with blood pressure. For example, alcohol consumption was, as expected, lower in patients with migraine. As alcohol consumption is associated with an increased blood pressure (22), it could be hypothesized that a lower blood pressure in patients with migraine could be due to a lower alcohol consumption in these patients. This was not the case, as the inverse association between migraine and high SBP was stronger in never drinkers (Table 3). Therefore, alcohol consumption could not explain the inverse relation between migraine and high SBP. Similarly, depression, which is more common in migraine patients, has also been found to be associated with a lower blood pressure (23). Again, the apparently stronger inverse association between migraine and high SBP in participants without a history of depression suggests that depression is not a strong confounding factor in this association. Similar conclusions apply for age, sex, and anti-hypertensive drug use, including β-blockers, which are often used as prophylactic treatment in migraine.
The present study has some limitations. The association described is cross-sectional and no temporal relationship between migraine and low blood pressure could therefore be inferred. It could be hypothesized that the pathophysiological mechanisms involved in migraine, which are still largely unknown, could lead to a lowering of blood pressure. As an example, the calcitonin gene-related peptide (CGRP) which has been involved in migraine (24) is also known to have major vasodilator and therefore hypotensive properties (25). It could also be hypothesized that people with low blood pressure are at higher risk of having migraine attacks or that both manifestations could share a common risk factor. By design, the present study is unable to discriminate between these pathophysiological hypotheses. To elucidate the question of the temporal relationship between migraine and low blood pressure, a possible approach would be to perform large cohort studies including young participants with blood pressure measured on several occasions during follow-up. Another potential limitation of the present study relates to the age of the participants. It could be argued that, because of their relatively old age, participants could have memory impairment leading to an underestimation of headache characteristics. However, participants were closely monitored with regard to cognition, as it was an important outcome of the EVA study and the overall cognitive level was high (12). Studying elderly participants has the advantage of obtaining a real lifetime frequency of hypertension. Hypertension often begins in middle-aged people and studying younger populations, which was the case in most previous studies, would ignore patients at risk of future hypertension.
These results have several implications. From a pragmatic point of view they confirm that headaches and migraine are not a reliable symptom of hypertension. Extreme values of blood pressure were uncommon in this study and an association between headache and very high values of blood pressure could not be ruled out. However, these data underscore that hypertension should be detected, diagnosed, and treated independently of the occurrence of headaches. From a pathophysiological point of view these results shed some light on the association between migraine and ischaemic stroke. This association, which has been observed mostly in young women in many studies (26), has received no clear explanation. The lack of positive association between migraine and hypertension observed in this study, but also in other studies with younger populations (9, 10), makes it very unlikely that blood pressure plays a significant role in the association between migraine and ischaemic stroke and suggests that other mechanisms should be considered and investigated. Finally, the observation of lower blood pressure in subjects with migraine, which does not seem to be explained by biases, raises the question of the underlying mechanism. Answering this question could make important progress in the understanding of the vascular component of migraine.
Footnotes
Acknowledgements
The EVA study was carried out under an agreement between the INSERM (Institut National de la Santé et de la Recherche Médicale), the Merck, Sharp and Dhome-Chibret Laboratories (West-Point, PA, USA) and the EISAI Company (Paris, France).