
Abstract
Background
Reduced endothelial function is associated with elevated risk of cardiovascular disease, but evidence on the association between migraine and endothelial function is conflicting. The aim of this population-based study was to examine the relationship between flow-mediated dilatation (FMD) and migraine with aura, migraine without aura and tension-type headache.
Methods
In the third Nord-Trøndelag Healthy Study (HUNT3) FMD was measured by ultrasound during reactive hyperaemia of the brachial artery in a sample of 4739 healthy adult participants, 3929 of whom answered headache questions. The cross-sectional association between different headache diagnoses and FMD was evaluated by logistic regression, using a categorical approach.
Results
Mean FMD did not differ between the headache groups and headache-free controls. In multi-adjusted analyses, no consistent association was found between FMD quintiles and headache groups.
Conclusions
There was no relationship between FMD and migraine or other headache diagnoses in this large cross-sectional study of otherwise healthy respondents including freedom from pulmonary and cardiovascular diseases.
Introduction
Migraine is a common primary headache disorder, affecting approximately 15% of the adult population, and is the sixth largest cause of disability worldwide (1,2). The condition is associated with an elevated risk of cardiovascular diseases, such as cerebral ischaemic incidents (3–5), myocardial infarction and claudication (6). Migraine with aura (MA) is associated with higher risk of ischaemic stroke (6) than migraine without aura (MwA), particularly in women (5,7–9). The mechanism causing the increased risk is currently unknown. Several explanations have been proposed, and a vascular hypothesis is currently discussed (10–12); specifically endothelial dysfunction (13).
Brachial artery flow-mediated dilatation (FMD) is the most frequently used non-invasive assessment of endothelial function (14). Individuals with decreased endothelial function have increased risk of cardiovascular events (15). Previous FMD studies in migraineurs have shown contradictory results; some clinical case-control studies with relatively small sample sizes have reported increased FMD (16) as well as decreased FMD in migraineurs (17,18), whereas most studies have reported no difference compared to controls (19–21).
The aim of the present study was to investigate the association between FMD and MA, MwA, tension-type headache (TTH) and unclassified headache in a large population-based cross-sectional survey, utilising comprehensive health-related information to adjust for possible confounding factors.
Methods
Study population
The third Nord-Trøndelag Health Study (HUNT3) was performed between October 2006 and June 2008. All inhabitants in Nord-Trøndelag County age 20 and older were invited to participate. Details of this study are described elsewhere (22). A sample of self-reported healthy participants who passed a brief medical interview, excluding those with pulmonary or cardiovascular disease, current antihypertensive or vasoactive treatment, cancer or physical impairment, were classified as the ‘Healthy HUNT3’ population, and candidates for the HUNT3 Fitness Study. The HUNT3 Fitness Study was one out of several sub-studies of the HUNT3 study. In addition to FMD (23), the HUNT3 Fitness Study also included measurements of peak oxygen uptake (24).
Of 94,194 invited adults, 50,795 individuals (54%) answered the initial questionnaire (Q1) and participated in a brief clinical examination, which included blood sampling and measurements of blood pressure, height and weight. A total of 39,690 answered the second questionnaire (Q2), which included headache questions (Figure 1). Characteristics of non-respondents have been described previously (25). In participants who answered Q1, 5633 volunteered to participate in the HUNT3 Fitness Study. Further exclusions were made, based on reports of dyspnoea in last 12 months, asthma or chronic bronchitis, cerebral or peripheral artery disease (including cerebral infarction), cardiac arrhythmias, current cholesterol-lowering treatment and pregnancy. In addition, 514 individuals withdrew during the test or were excluded because of low ultrasound image quality. FMD was measured in 4739 individuals, whereof 3929 also completed the headache questions, and were subsequently included in the present study.
Flowchart of the participants.
Endothelial function
Endothelial function was evaluated by brachial artery FMD, according to guidelines (26). All participants were asked to abstain from food, smoking and dipping tobacco during the last four hours pre-test, but this was not achieved in the majority of respondents since measurements were taken throughout the whole day. Thus, 47% reported drinking coffee, 75% reported food intake, and 13% of women and 22% of men reported tobacco use within four hours before the test. Further details of the investigation and the participants are described elsewhere (23). FMD was measured with the participant in the supine position, in a dark room with neutral temperature and minimal noise. Measurements were performed by 12 MHz ultrasonography (Vivid-i, GE Healthcare, USA) with three-point electrocardiogram (ECG) monitoring. The transducer visualised the left brachial artery in the longitudinal plane, above the antecubital fossa. After 10 minutes of supine rest, the baseline arterial diameter was measured. A temporary arterial occlusion was created by a cuff on the forearm inflated at 250 mmHg for five minutes, before being abruptly deflated. Blood flow was estimated by pulsed Doppler velocity 10 seconds after cuff deflation. Post-occlusion arterial diameter was measured 60 seconds after cuff deflation. All arterial diameters were recorded at the peak of the R-wave in the ECG, to avoid confounding for cyclic changes in the arterial dimension. Three measurements (intima to intima) were recorded using optical callipers with 0.1 mm resolution, and mean value was calculated. The difference in post-occlusion diameter and baseline diameter was used as maximum dilatation of the artery, yielding FMD expressed as per cent change from baseline. A widely accepted definition of endothelial dysfunction (ED) measured by FMD does not exist. In the present study, we focused on unadjusted FMD, because we previously have found that FMD adjusted for shear rate had the same pattern as unadjusted (23).
FMD measurements were performed by a team of six specially trained individuals. Because of high throughput of participants, we could not repeat measurements (23). Interobserver analysis of recordings was evaluated in a group of more than 80 HUNT3 participants, giving a mean difference ranging from −1.24 (95% confidence interval (CI) −5.38 to 2.90) to 2.25 (95% CI −1.35 to 5.85) using the Bland-Altman plot, with Pitman’s test of difference in variance ranging from r = 0.008 (n = 81, p = 0.94) to r = −0.85 (n = 82, p < 0.001) (23).
Headache diagnosis
Headache questions in the second questionnaire (Q2).

Potential confounders and effect modifiers
Among a wide range of health-related information included in HUNT3 (22), we have previously identified several important factors associated with migraine (30), headache (31) and FMD (23,32). We analysed data separately by gender and adjusting for age (continuous variable), because endothelial function differs strongly by these two factors (23). FMD was also evaluated separately among men and women in the two age groups 20–50 years and above 50 years. These groups were chosen because we have recently demonstrated an inverse relationship between headache and peak oxygen uptake restricted to individuals between 20 and 50 years of age (33). Furthermore, as endothelial function is influenced by cardiovascular risk factors (32), we adjusted for systolic blood pressure (categorical; <140 mmHg, 140–159 mmHg, ≥160 mmHg), body mass index (BMI) (categorical; normal <25, overweight 25–29, obesity ≥30), serum cholesterol (categorical; normal ≤5.20 mM, intermediate 5.21–6.19 mM, elevated ≥6.20 mM), non-fasting serum glucose (categorical; normal < 7.80 mM, intermediate 7.80–11.09 mM, elevated ≥11.10 mM) and smoking status (three categories: current, previously or never daily smoking). According to a pre-planned strategy the following variables were also included as potential confounders and effect modifiers: socioeconomic status (evaluated by work status in three categories; (a) full-time workers, (b) part-time workers or (c) unemployed, students or household workers), and alcohol consumption (five categories).
Ethics
The Norwegian Regional Committee of Ethics in Medical Research approved this study. The HUNT Study was also approved by The Norwegian Data Protection Authority.
Statistics
Comparisons of baseline characteristics were carried out using analysis of variance for continuous variables, and Pearson Chi square test for categorical variables. In multivariate logistic regression analyses, we estimated the prevalence odds ratio (OR) with a CI of 95% for the association between type of headache (MA, MwA, TTH and unclassified headache) and FMD, using a categorical approach. First, FMD was evaluated based on quintiles in accordance with our previous study (33). FMD scores within the upper quintile were used as reference. We initially adjusted for age and gender, and subsequently for predefined confounding factors. These factors were tested in the multiple logistic regression analyses separately or together, and were excluded from the final models if the OR changed less than 0.05. Potential interaction between two variables was evaluated by including the product of the variables in the logistic regression analyses, and the interaction coefficient was tested using Wald χ2 statistics. Serum glucose, serum cholesterol, systolic blood pressure and socioeconomic status stood out as important confounders, and therefore all final analyses were adjusted for these factors, in addition to age and gender. On the other hand, OR was changed less than 0.05 when we adjusted for BMI, smoking status and alcohol consumption, and were consequently not included in the final regression models. Participants with incomplete data for one or several variables were included (as a separate ‘missing’ category) in all analyses to reduce the impact of response bias.
To evaluate the probability of a linear relationship between FMD and prevalence of headache subtypes (dose-response relationship), we included FMD as a continuous variable in a two-sided test of trend. All data analyses were carried out using SPSS software (IBM Corp., Armonk, NY, USA, version 22.0).
Results
Baseline characteristics of the HUNT3 Fitness Study population compared to the total HUNT3 population and the ‘Healthy HUNT3’ population a .
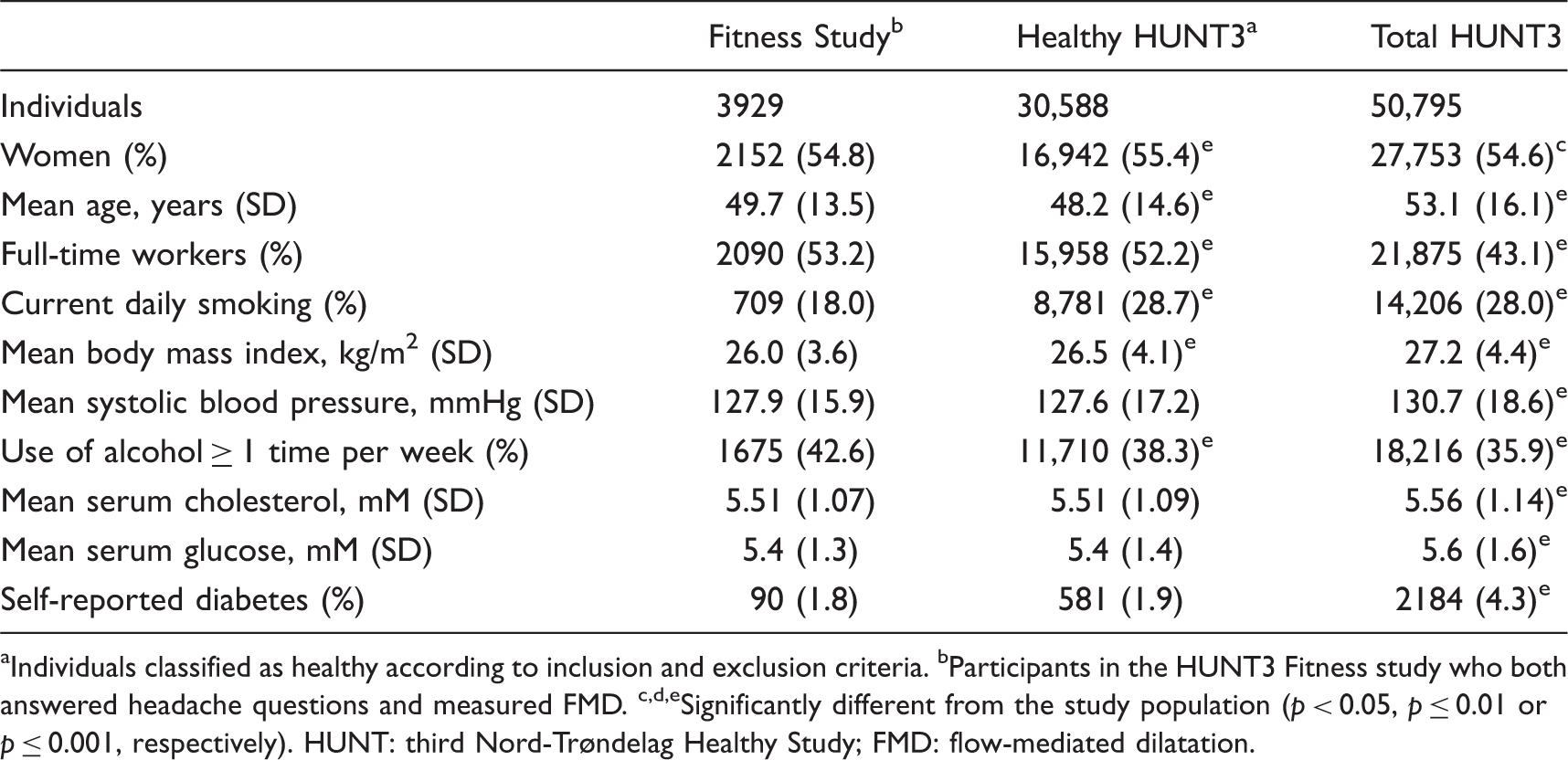
Individuals classified as healthy according to inclusion and exclusion criteria. bParticipants in the HUNT3 Fitness study who both answered headache questions and measured FMD. c,d,eSignificantly different from the study population (p < 0.05, p ≤ 0.01 or p ≤ 0.001, respectively). HUNT: third Nord-Trøndelag Healthy Study; FMD: flow-mediated dilatation.
Characteristics of the study population according to headache status.

MwA: migraine without aura; MA: migraine with aura; TTT: tension-type headache; BMI: body mass index; SBP: systolic blood pressure. Headache free versus any headache: a,b,cp < 0.05, p ≤ 0.01 or p ≤ 0.001, respectively.
FMD
As demonstrated by Figure 2, mean FMD did not differ significantly between headache diagnoses.
Mean flow-mediated dilatation (FMD) values with 95% confidence interval (CI) related to headache diagnoses (exact mean values with 95% CI below).
Odds ratio of headache related to quintiles of FMD.

Adjusted for age, gender, cholesterol, glucose, systolic blood pressure and work status. bAdjusted for same variables as in a, except gender. cFMD as a continuous variable, adjusted for the same variables as in a or b. FMD: flow-mediated dilatation; MwA: migraine without aura; MA: migraine with aura; TTT: tension-type headache; OR: odds ratio; CI: confidence interval.
Discussion
In this large cross-sectional population-based study with healthy individuals free from pulmonary and cardiovascular diseases, we did not find any association between FMD and MA, MwA or TTH. Therefore, the findings do not support the hypothesis that dysregulation of vascular endothelium is a factor associated to these headache diagnoses. However, our results regarding MA should be evaluated with caution because of the possibility of misclassification of migraine participants with MA and MwA.
Comparisons to other studies
In accordance with our results, a recent meta-analysis by Butt et al. (11) concluded with no clear association between FMD and MA. Furthermore, Perko et al. (19) found no alterations in FMD in migraineurs in general. On the other hand, Vernieri et al. (16) found increased FMD in individuals with MA, but not in those with MwA.
Several studies support the hypothesis of decreased endothelial function in migraineurs in general (17,18,34). However, all of them were based on small numbers, mostly evaluating fewer than 50 migraine patients. Few studies have performed analyses of FMD in MA and MwA separately (16,19–21). In addition, González-Quintanilla et al. (35) evaluated patients with chronic migraine, and found lower FMD in chronic migraineurs, compared both to controls and patients with episodic migraine. Vanmolkot et al. (34) evaluated only migraine of recent onset, finding lower FMD (normalised to peak shear rate) in migraineurs than in controls.
Interpretation
The mechanism linking migraine with cardiovascular disease is complex, but the present study does not support the hypothesis of abnormal endothelial function. Notably, in the present study we excluded those with cancer, pulmonary disease, cardiovascular disease and current antihypertensive treatment. In this way migraineurs with vascular disease may have been excluded, which may have biased our results. However, if reduced peripheral vascular function were an important factor in MA or MwA, this would have been detected in our large sample. Thus, assessing endothelial function by FMD does not contribute to the evaluation of migraine in an otherwise healthy population.
Strengths and limitations of the study
Major strengths of this study are the large sample size, the population-based design, and the use of validated headache diagnoses. In the multivariate analyses we were able to adjust for a large number of confounding factors. However, the possibility of residual confounding cannot be excluded in this observational study. Although the sensitivity was good and specificity high both for migraine and TTH (29), some misclassification may have occurred. This may have led to an underestimation of potential differences between migraine and TTH. Furthermore, the possibility of misclassification of participants with MA and MwA should also be highlighted because of the low sensitivity of the questionnaire concerning MA. Individuals who had sensory aura only were not included in the MA group owning to low specificity of the question about sensory symptoms prior to or during headache (29). Thus, the results regarding MA in the present study should be evaluated with caution.
Several other limitations should also be considered. First, results should be generalised with caution, partly because only 42% of the adults invited to HUNT3 answered the headache questionnaire, and partly because participants in the FMD study were free from cardiovascular disease and cancer. The HUNT3 Fitness Study excluded those who used antihypertensive medication, including migraine patients using beta-blockers or angiotensin receptor blockers for prophylaxis. The selection of the individuals without cardiovascular diseases may have led to exclusion of migraineurs with the worst endothelial function. This selection limits the applicability of our findings to otherwise self-reported healthy participants, and our results are not representative for the general population of migraineurs
Second, the compliance to the fasting regimen was poor; 47% reported drinking coffee, 75% reported food intake, and 13% of women and 22% of men reported tobacco use within four hours before the test. Among women, details about menstrual cycle and menstruation status were not available. Thus, testing conditions were not in accordance with the guidelines for most of the participants (26). This is a major limitation, because all these factors may affect FMD (26). However, there was no difference in FMD between fasting and non-fasting individuals in the 4739 participants in the HUNT3 Fitness Study (23). Furthermore, no significant association between FMD and headache was found among women aged below or above 50 years of age. Thus, indirectly, being postmenopausal or not did not influence the relationship between FMD and headache.
There is a lack of evidence for the correlation between peripheral and cerebral endothelial function (36,37). FMD is known to be associated with coronary endothelial function (38). Interestingly, although Rajan et al. (37) did not find any significant difference in FMD between migraineurs and healthy controls, they found an isolated impaired endothelial function measured in the posterior cerebral circulation.
Conclusion
This study of healthy individuals free from pulmonary and cardiovascular diseases did not confirm any difference in FMD between migraineurs and headache-free participants, and consequently did not support the notion that migraine is associated with systemic endothelial dysfunction. Thus, FMD is not a useful tool in the evaluation of migraine in otherwise healthy people. Our results regarding MA should be evaluated with caution because of the possibility of misclassification of migraineurs with and without aura.
Clinical implications
This population-based study of healthy individuals including freedom from pulmonary and cardiovascular diseases did not support the notion that migraine is associated with systemic endothelial dysfunction. Flow-mediated dilatation (FMD) is not a useful tool in the evaluation of migraine or other headaches in otherwise healthy people.
Footnotes
Acknowledgements
The Nord-Trøndelag Health Study (The HUNT study) is a collaboration between the HUNT Research Centre, the Faculty of Medicine at the Norwegian University of Science and Technology (NTNU); Norwegian Institute of Public Health, the Regional Health Authority of Central Norway, the Nord-Trøndelag County Council, the Ministry of Health and Care Services, and the Norwegian Council on Cardiovascular Disease.
JL and KH conceived of the study and performed the statistical analyses. JL, EAS, KH, UW, ØE, ML and LJS all participated in the design and drafted the manuscript. All authors read and approved the final manuscript.
A large number of partners founded HUNT3.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The main contributions came from The Ministry of Health, the Nord-Trøndelag County Council, and The Norwegian University of Science and Technology.