
Abstract
Background
The aim of our study was to estimate the one-year prevalence of primary headache disorders in three different social groups using the third edition beta of the International Classification of Headache Disorders (ICHD-3 beta).
Material and methods
The study population included a total of 3124 participants: 1042 students (719 females, 323 males, mean age 20.6, age range 17–40), 1075 workers (146 females, 929 males, mean age 40.4, age range 21–67) and 1007 blood donors (484 females, 523 males, mean age 34.1, age range 18–64). We used a semi-structured, validated face-to-face interview.
Results
The age-adjusted one-year prevalence of migraine in females was significantly higher (p < 0.001) in students (41.9%) than in workers (19.2%) and blood donors (18.7%). Age-adjusted prevalence of migraine among males did not differ among the three groups: 4.5% in students, 4.9% in workers and 4.5% in blood donors. Age-adjusted prevalence of tension-type headache (TTH) among females was almost the same in students and blood donors (68.8% and 66.7%) but female workers had a lower prevalence of TTH (57%). Age-adjusted prevalence of TTH among males did not differ significantly between students and blood donors (55.8% and 58.1%) but male workers had a significantly lower (p < 0.001) prevalence of TTH (30.7%). The prevalence of chronic headache in students (TTH and/or migraine) was 3% and of probable medication-overuse headache 3%, significantly more than in workers and blood donors.
Conclusion
Headache prevalence was high and differed markedly among the three social groups. It is important that headache epidemiology also focus on socially defined groups in order to target future preventive efforts.
Introduction
Lots of studies in many different countries have examined the prevalence of headache disorders (1–9). None of them have, however, used the newly published International Classification of Headache Disorders third edition beta (ICHD-3 beta) to diagnose the different types of headache (10). Furthermore, only a few studies have previously compared the prevalence of headache disorders in different social groups including sufficiently large samples in each social group to allow precise comparisons (11–17).
Our two hypotheses were that the results using ICHD-3 beta would be similar to results with ICHD-2 and that the prevalence of headache disorders would differ among social groups. We therefore conducted a professional direct interview using a validated semi-structured questionnaire in three different social groups: students, workers and blood donors. This diagnostic methodology is optimal for epidemiological studies but it is very resource demanding. Nevertheless, we included more than 1000 people in each group to allow sufficient statistical strength to document differences between groups, and we used ICHD-3 beta diagnoses for the first time in a large epidemiological study. We performed age- and sex-specific analyses of the data.
Materials and methods
Study design
This was a cross-sectional study that was conducted between September 2012 and August 2013.
Study populations
We included 3124 individuals who agreed to be interviewed and were able to give characteristics of headaches unless the following reasons for exclusion were present: patient had a history of stroke or transient ischemic attack (TIA), subarachnoid hemorrhage, intracranial aneurysm, intracranial hemorrhage, brain tumor, any operation on the brain, multiple sclerosis, epilepsy, encephalitis, meningitis, dementia, or other serious neurological or somatic disorder. Selection of the three social groups that were needed to test our hypotheses was based on feasibility. We had already used blood donors as controls in previous studies of saccular intracranial aneurysms and knew that they would have a high participation rate. Although they come from many different occupations, they still constitute a social group. This is defined as “two or more people who interact with one another, share similar characteristics and collectively have a sense of unity” or “a group is defined in terms of those who identify themselves as members of the group” (18). Workers could be studied as part of a compulsory health examination conducted by one of the authors that also ensured a high participation rate. Finally, we already had contact with medical students with an interest in headache, and discussion with class representatives indicated that also here we could have a high participation rate.
Data collection
All participants were interviewed using a semi-structured, validated face-to-face interview conducted by a neurologist or by trained senior medical students. The student interviewers were recruited after a postgraduate lecture on headache attended by especially interested medical students. Fifteen senior (last year of medical university) medical students accepted but only 11 completed the following program and completed the actual interviews. First they were given literature and personal teaching. Next they performed at least 10 supervised interviews that were not used in the actual study. The participation rate for students was 92%. We performed this interview in their classrooms when all lessons were finished at the end of the day. We included students at all semesters (1–12).
Workers at an oil and gas factory were recruited as part of a compulsory annual medical examination of all employees. Office workers were not included. Participation was 97%. The interview was performed in the room where a neurologist examined these workers during the annual medical examination. In some cases time did not allow us to finish the headache interview immediately but participants agreed to finish the interview by telephone.
Blood donors were recruited consecutively in association with their donation of blood. We included everybody who agreed to participate and met inclusion and exclusion criteria. Participation was 98%. The interview was performed in the room where donors donated their blood. Because of the high participation rate in all three groups, it was judged unnecessary to perform a non-participant analysis.
The semi-structured interview was modified and expanded from a previously validated interview (19). It included four parts: 1) personal data (age, sex, profession, telephone number); 2) detailed characteristics of headache; 3) information about possible risk factors for headache, and 4) previous consultation, diagnosis and treatment of headache. The latter two data sets will be published separately.
Our diagnostic procedure included three steps. The semi-structured face-to-face interview about headache in the previous year was first obtained from all three groups. Repeated interview by telephone was then performed by a neurologist (NRK) if participants had incomplete data for ICHD-3 beta diagnosis or if other important information was missing. We re-interviewed 2% of the participants. The headaches of each participant were then diagnosed according to ICHD-3 beta by ERL, NRK and JO. We did not include questionnaires if important data were missing and it was impossible to contact the participant. We excluded on this basis 125 participants and also excluded five participants according to our exclusion criteria. The total number of participants included in the study was 3124.
Statistical analysis
The outcome variables of the study were the crude and gender-standardized one-year prevalence of migraine without aura and with aura, probable migraine (all but one International Headache Society (IHS) criterion met, and not fulfilling the IHS criteria for TTH), episodic/frequent TTH, probable TTH (all but one IHS criterion for TTH met and not fulfilling the IHS criteria for migraine or probable migraine), cluster headache, chronic probable migraine, chronic TTH and probable medication-overuse headache. No participant overused triptans or other migraine drugs except analgesics (painkillers).
Age-specific prevalence of primary headache disorders in the three groups was calculated using the direct standardization method (20). The age structure of the total sample (donors, workers and students) was used as a standard. The sex-specific differences in headache non-adjusted prevalence among participants of the three different social groups were statistically examined by an unpaired t-test and chi-square test. Crude prevalence of headache disorders was calculated in percentages. Odds ratios (OR) and 95% confidence intervals (CI) were estimated using univariate and multiple conditional logistic regression models. We aimed to have power to detect differences between social groups in prevalence of migraine and TTH but not their subforms or differences in the prevalence of the rarer headache disorders. A two-tailed p-value < 0.05 was statistically significant.
We estimated that the average prevalence of migraine would be 12% (2,9) and that it would be 16% in females and 8% in males. With a p value of 0.05 and a risk of type 2 error of 20%, we estimated that the sample size would need to be 258. In order to have power to detect sex-specific differences and to have enough power if differences were somewhat smaller, we chose a sample size of 1000. For each item we used only participants with data on that item. Therefore the number of participants in these tables was sometimes less than the total number in each group.
Ethics considerations
The Medical Ethics Committee of the Urals State Medical University approved this study. All respondents were informed of the purpose of the survey. Written informed consent was obtained from all participants.
Results
Age and sex distribution of participants of three different social groups (blood donors, workers and students).

One-year crude prevalence of headache disorders according to ICHD-3 beta in blood donors, workers and students.
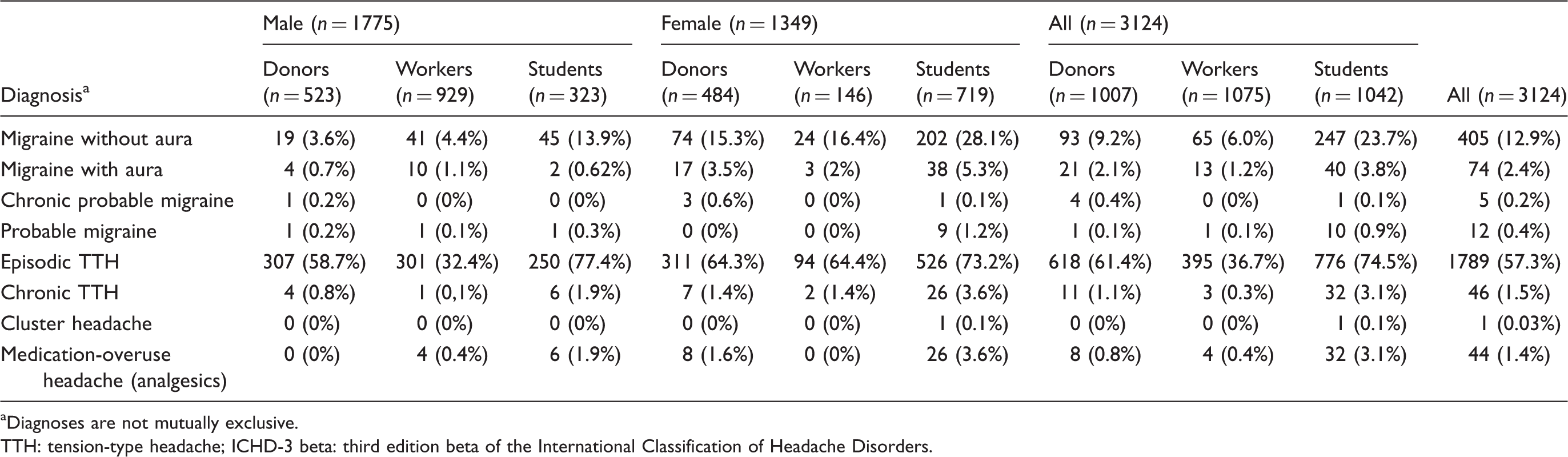
Diagnoses are not mutually exclusive.
TTH: tension-type headache; ICHD-3 beta: third edition beta of the International Classification of Headache Disorders.
Age-adjusted one-year prevalence of migraine in three different social groups according to age strata.

The prevalence of any headache varied among social groups (Table 2): In females it was 95.1% in students, 69.2% in workers, 74.5% in blood donors (p < 0.001); in males it was 87.9% in students, 38.3% in workers and 61.7% in donors (p < 0.001). The migraine prevalence was 15.9% overall. In females it was: 34.7% in students, 18.5% in workers and 19.4% in blood donors (p < 0.001); in males: 14.8% in students, in 5.6% workers, and 4.8% in blood donors (p < 0.001) (Figure 1(a) and (b)). The prevalence of TTH in females was: 76.7% in students, 65.7% in workers and 67.5% in blood donors (p > 0.05); in males: 79.2% in students, 32.5% in workers, 59.5% in blood donors (p < 0.001).We found that 51 participants (1.6%) out of 3124 had chronic headache. Five participants had chronic probable migraine (four females and one male); blood donors (0.4%) and students (0.1%) and no workers had chronic migraine. The prevalence of chronic TTH in students (3%) was higher than in donors (1%) and workers (0.3%), p < 0.0001, and it was significantly higher in females (3.6% in students, 1.4% in blood donors and 1.4% in workers) than in males (1.9% in students, 0.8% in blood donors and 0.1% in workers). Probable medication-overuse headache (analgesics ≥15 days per month) in students (3%) was higher than in blood donors (0.79%) and workers (0.37%), p < 0.001.
One-year crude prevalence of migraine and tension-type headache (TTH) in males (a) and females (b) in three different social groups.
Figure 1(a) shows crude headache prevalence (migraine and TTH) in percentage of males in three different social groups (blood donors, workers, students), and Figure 1(b) shows distribution of crude headache prevalence in females in three different social groups.
Age-adjusted one-year prevalence of TTH in three different social groups according to age strata.

Age at onset of primary headache in blood donors, workers and students.

Number of participants of three different social groups with tension-type headache (TTH) and migraine according to frequency of headaches in the previous year.
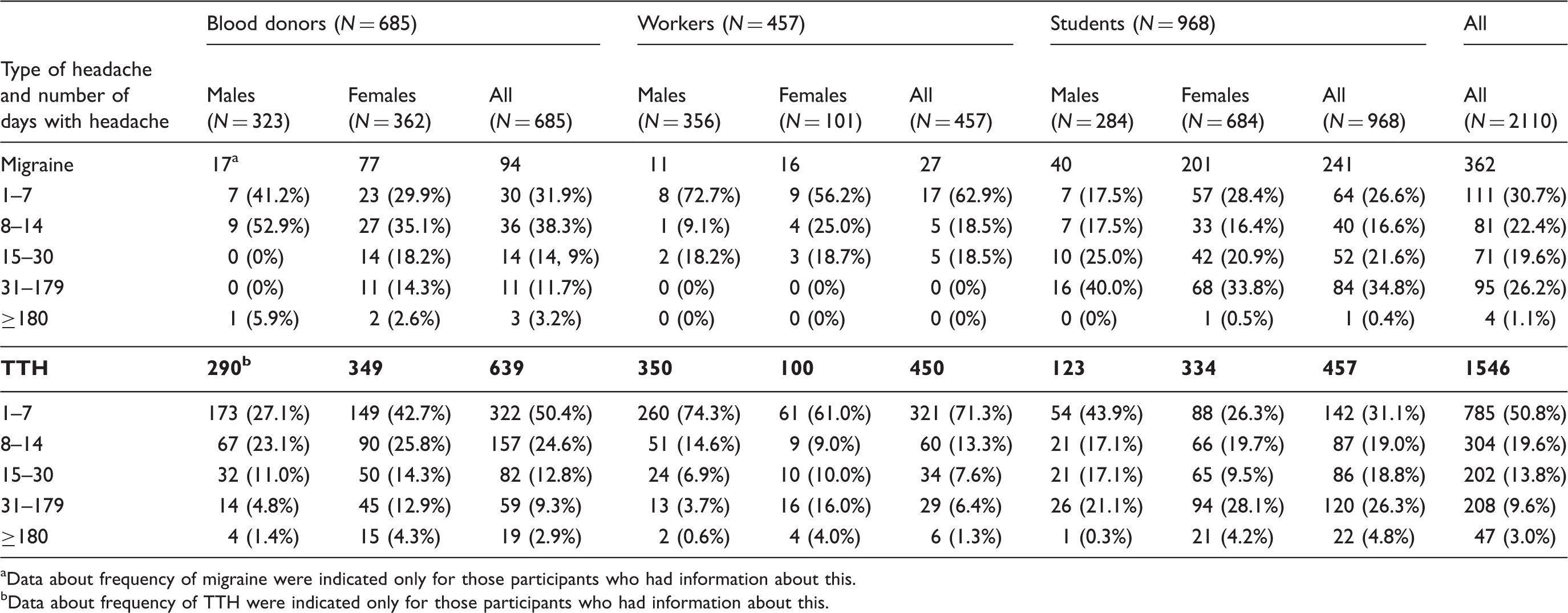
Data about frequency of migraine were indicated only for those participants who had information about this.
Data about frequency of TTH were indicated only for those participants who had information about this.
Discussion
We demonstrated a prevalence of primary headache disorders using ICHD-3 beta that is similar to previous studies using ICHD-2. We showed major differences in the prevalence of migraine and TTH among social groups. Groups with a high prevalence of a headache disorder also had a high frequency of attacks; for example, females had a higher frequency of attacks than males and students a higher frequency than workers.
One-year prevalence of primary headache disorders
Using ICHD-3 beta, our study demonstrated a high one-year prevalence of headache disorders in Russia (67.5%) in accordance with a recent Russian study and many international studies using ICHD-2 (2,21). One-year prevalence of headache in other studies varied from 4.7% to 80.8% (22–45). The highest one-year prevalence of headache was found in Brazil, Finland and Denmark (1,5,38). The lowest one-year prevalence of headache was found in China (41).
The one-year prevalence of migraine was 15.9% (males 7%, females 27.5%) in our study. This is in accordance with data from the Global Burden of Disease Study 2010 (14.7%) (46) and almost the same as in many other counties. The one-year prevalence of migraine with aura (MA) was 2.4% in our study. It was higher in Denmark 4% (5). The one-year prevalence of MA in other countries was almost the same as in our study and even lower: in Austria 2.3% (17), and in Ethiopia 2.6% (35). Many studies did not investigate the prevalence of MA at all.
Episodic TTH was the most prevalent primary headache in our study: 57.4% (71.6% in females, 49% in males, female/male ratio 1.5:1). It was higher than in the first epidemiological study of headache in Russia (30.8%). Our data are in accordance with Rasmussen et al. (5) in Denmark who found 74%. The lowest one-year prevalence of TTH was found in Ethiopia, China and Germany.
The one-year prevalence of chronic headache in our study was almost the same as in many other epidemiological studies in other countries. In Russia Ayzenberg et al. found, however, a significantly higher prevalence of chronic headache (10.5% vs our 1.7%) (21). In Georgia it was also higher (7.6%) (28). This difference can perhaps be explained by an almost total absence of participants from villages and from low social strata in our study.
Headache prevalence differs among social groups
Blood donors had prevalence in line with the general population in many previous studies as cited above. The lower prevalence of any headache in workers was because male workers had a lower prevalence of TTH. Students stood out with a higher prevalence of migraine but also of TTH. The above differences were strengthened by the fact that students also had a higher frequency of days with migraine and TTH while workers had a lower frequency. These results were largely unchanged by age correction using our own data. If we had used data published by others (47,48), the differences among social groups would have been even higher than the uncorrected values because the prevalence of migraine and TTH was shown to increase up to the age of 40. In our study workers were an average age of 40.4 while donors were age 34.1 and students 20.6.
The low prevalence of TTH in male workers may relate to their physical work and selection of the fittest for these highly paid jobs. We cannot exclude that male workers disregarded TTH as part of a macho attitude or because they would not consent to any weakness as part of the health examination that was paid for by the employer fearing consequences for their employment.
We can compare our results in workers with two studies among workers of a textile factory in Ethiopia (35). The one-year prevalence of migraine was 6.2% and of TTH 9%, almost the same as in workers in our study (7.3%), but the prevalence of TTH was significantly lower than in our study (37%). A low prevalence of headache in workers suggests that physical work may be associated with reduced prevalence of headache, especially TTH. However, heavy physical work may not alter the prevalence of TTH as the one-month prevalence of headache in heavy engineering workers in Turkey was 43.2% (11).
More striking was the very high prevalence of migraine, TTH and probable medication-overuse headache in students. Several previous studies of the prevalence of headache disorders in students showed prevalence of migraine in the range 6.4%–28.4% and of TTH in the range 18%–44.2%.The lowest prevalence of migraine was found in Nigeria (6.4%) and Norway (6.4%) (1,37) and the highest in Poland (28.4%) and Turkey (21.9%) (16,27). We found a prevalence of 28.6% in students. TTH was investigated only in a few studies in students. The one-year prevalence was 18% in Norway, 18% in Nigeria and 44.2% in Iran (1,37,40). In our study it was significantly higher: 74.5%. Our impression is that other studies may have missed the infrequent TTH individuals in whom TTH is really not a problem. In our study they accounted for 60% of all TTH cases.
Strengths and weaknesses of our study
A strength of our study was that we used the ICHD-3 beta for an epidemiological study for the first time. Furthermore, we used a direct interview and a validated semi-structured interview instead of a questionnaire. We studied different social groups and each group had a very large size for a direct interview study. The different age and sex distribution of the three social groups was impossible to avoid. This will be the case for all studies comparing social groups because age and sex distributions will always differ in contrast to classical population-based epidemiological studies. We compensated for the influence of age and sex by age- and sex-specific comparisons and present only such comparisons of social groups. A challenge is the low level of awareness of headache disorders in the Russian population causing difficulty eliciting a precise history in participants having more than one headache disorder. Our use of medical students for one-third of the interviews might also be a weakness. We used, however, only senior students and trained them carefully. Nevertheless their interviews were sometimes incomplete but in such cases we re-interviewed the participants. Our results cannot be generalized to the whole Russian population because we had almost no participants from villages or from low social strata.
Conclusions
We found that the prevalence of primary headache disorders using ICHD-3 beta was similar to previous findings in other countries with ICHD-2. Social groups have markedly different prevalence of migraine and TTH. Very high prevalence in university students merits further investigation and preventive efforts. Our findings underline that headache epidemiology in the future should focus on socially defined groups in order to target future preventive efforts.
Public health relevance
The prevalence of migraine and tension-type headache (TTH) according to the third edition beta of the International Classification of Headache Disorders (ICHD-3 beta) is similar to the prevalence with ICHD-2. There are major differences in the prevalence of migraine and TTH between social groups. Social groups with a high prevalence of a headache disorder also had a high frequency of attacks. Females have not only a higher prevalence but also a greater frequency of attacks. Headache epidemiology in the future should focus on socially defined groups in order to target preventive efforts.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Acknowledgments
We gratefully acknowledge the following doctors and students who participated in this study: T.S. Tsypushkina, P.A. Filimonova, K.I. Fljagina, N.I. Tsvetkova, E.A. Korzovatykh, A.N. Ruzaeva, V.V. Shirshova, A.D. Kozlova, T.A. Troshina, A.D. Malygina, A.M. Alent’ev, Ju. S. Drozd, Ju. V. Sarafanova, I.A. Dyachkov, P.A. Oshurkov and A.V. Dmitriev. We also thank Professor R.H. Jensen and Professor T.J. Steiner for valuable comments on our manuscript.