
Abstract

Dear Sir,
Painful cranial neuropathies are a group of entities causing pain in the distribution of one particular nerve (1,2). Some of them are well characterized while others have been identified only very recently. Apart from first-division trigeminal neuralgia, several neuropathies affecting the terminal branches of the trigeminal nerve may involve the orbital and periorbital area, including supraorbital/supratrochlear neuralgia (3), infraorbital neuralgia (4) and lacrimal neuralgia (5). Pareja et al. have recently described infratrochlear neuralgia in seven patients presenting with paroxysmal pain in the internal angle of the orbit (6). In each patient, the pain appeared in one of three different locations within the territory supplied by the infratrochlear nerve, namely, the medial half of the palpebra superior, the caruncula lacrimalis and the lateral aspect of the radix nasi. Although most of the patients (six out of seven) were treated with oral drugs, we advocate anaesthetic blockades as a safe and effective treatment for this condition. We aim to present a new case of infratrochlear neuralgia, as well as the result of the anaesthetic blockade of the infratrochlear nerve.
A 46-year-old woman with prior history of migraine without aura came to our office complaining of a new type of pain. She had paroxysms of pressing pain in the internal angle of the right orbit and the medial half of the right palpebra superior. The episodes roughly lasted 2 minutes and they ranged from mild (3 out of 10) to moderate (7 out 10) in intensity. She had been experiencing such a pain for 1 year with an average frequency of once per week. The patient could not identify any trigger. Between the paroxysms, she felt pain within the symptomatic area when gently touching it. Sensory examination demonstrated the presence of hyperesthesia and allodynia in the painful area. In addition, palpation of the medial edge of the right orbit just above the caruncula lacrimalis was extremely painful. This area matched the point where the infrathrochlear nerve emerges from the orbit. The pain evoked upon palpation did not increase with vertical eye movements. All ancillary tests, including routine blood tests, immunological screening and brain and orbital magnetic resonance imaging, were normal.
Considering infratrochlear neuralgia as the most reasonable diagnosis, we performed an anaesthetic blockade at the point mentioned above (Figure 1(a)). We injected 0.5 cc of bupivacaine 0.5% with a 30-gauge needle. After 5 minutes, we verified that the patient had developed an area of hypoesthesia in the whole area innervated by the infratrochlear nerve, including the medial palpebra superior, the caruncula lacrimalis and the lateral aspect of the radix nasi (dotted area in Figure 1(b,c)). After 2 weeks, both the allodynia and the hypersensitivity of the nerve had dramatically improved and the patient had only experienced a minor and brief painful episode. A second nerve block was then performed and the patient was completely asymptomatic over a subsequent follow-up of 4 weeks.
(a) Infratrochlear nerve block: the needle is inserted through the internal angle of the orbit just above the caruncula lacrimalis; the anaesthetic solution is injected at the emergence of the infratrochlear nerve; (b,c) topographic distribution of the anaesthetized area matching the whole skin territory of the infratrochlear nerve (dotted area): medial palpebra superior, caruncula lacrimalis and lateral aspect of the radix nasi.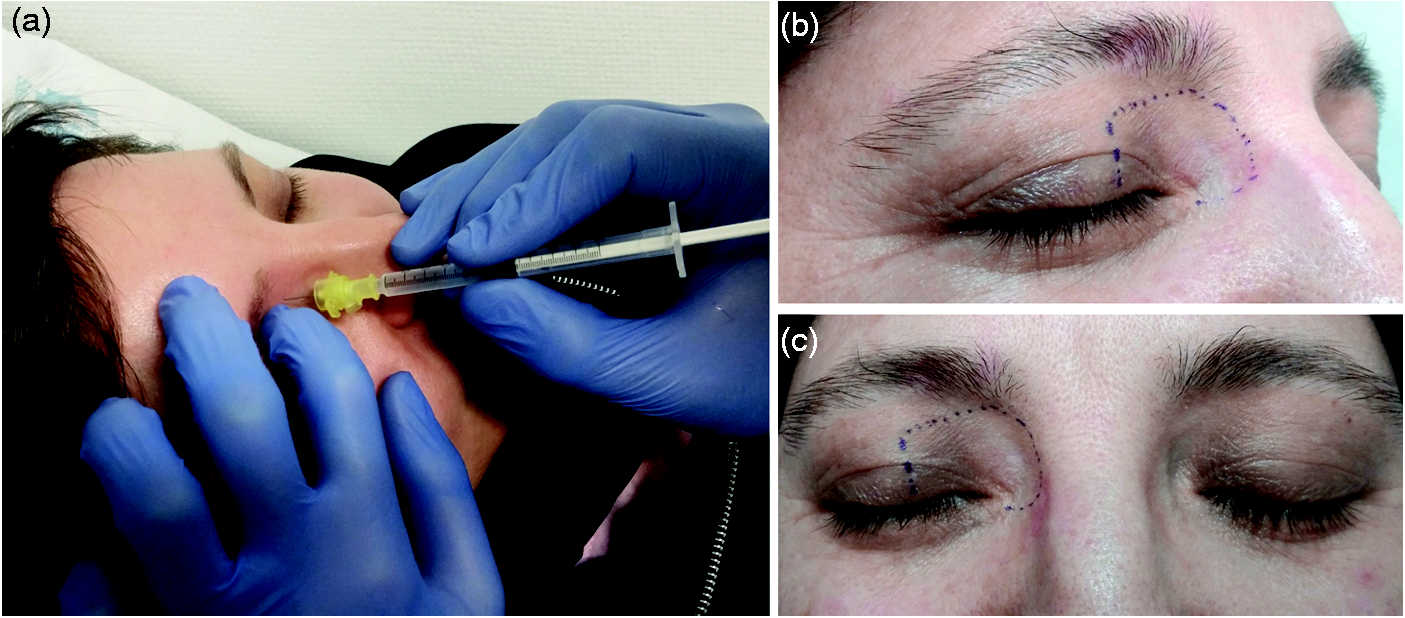
In conclusion, this is new evidence that infratrochlear neuralgia does exist. Indeed, the pain and the sensory symptoms in our patient were localized in one of the territories innervated by the infratrochlear nerve. Moreover, we accomplished a clinical response to the anaesthetic blockade, which was performed just at the point where the infratrochlear nerve emerges from the orbit. In addition, we confirmed that the anaesthetized area matched exactly with the whole skin territory supplied by the infratrochlear nerve. As in other terminal branch neuralgias, peripheral nerve blocks may be effective for infratrochlear neuralgia.
Footnotes
Conflict of interest
None declared.
Patient consent
Informed consent was obtained from the patient included in this letter.