
Abstract
Background
Sphenopalatine ganglion percutaneous radiofrequency thermocoagulation treatment can improve the symptoms of cluster headaches to some extent. However, as an ablation treatment, radiofrequency thermocoagulation treatment also has side effects.
Objective
To preliminarily evaluate the efficacy and safety of a non-ablative computerized tomography-guided pulsed radiofrequency treatment of sphenopalatine ganglion in patients with refractory cluster headaches.
Methods
We included and analysed 16 consecutive cluster headache patients who failed to respond to conservative therapy from the Pain Management Center at the Beijing Tiantan Hospital between April 2012 and September 2013 treated with pulsed radiofrequency treatment of sphenopalatine ganglion.
Results
Eleven of 13 episodic cluster headaches patients and one of three chronic cluster headaches patient were completely relieved of the headache within an average of 6.3 ± 6.0 days following the treatment. Two episodic cluster headache patients and two chronic cluster headache patients showed no pain relief following the treatment. The mean follow-up time was 17.0 ± 5.5 months. All patients enrolled in this study showed no treatment-related side effects or complications.
Conclusion
Our data show that patients with refractory episodic cluster headaches were quickly, effectively and safely relieved from the cluster period after computerized tomography-guided pulsed radiofrequency treatment of sphenopalatine ganglion, suggesting that it may be a therapeutic option if conservative treatments fail.
Introduction
Drug treatments have been the preferred therapeutic strategy for cluster headaches (CHs). However, the poor curative efficacy and the intolerant side effects of drug treatments have led to the consideration of other invasive therapies, including nerve blockade (1–3), nerve stimulation (4–6), neurolytic procedures (7–9) and deep brain stimulation (10). However, CH remains a rare disease with unsatisfactory therapeutic outcomes and risk of treatment-related side effects. The sphenopalatine ganglion (SPG) plays an important role in the pathology of CHs. Studies report that a steroid injection combined with a local anaesthetic to block the SPG (2,3), SPG electrical stimulation (4–6) and a neurolytic agent (e.g. ethanol) (7) or radiofrequency thermocoagulation treatments (8,9) to resect the SPG have improved the symptoms of CHs. In 2011, Chua et al. first applied a non-ablative pulsed radiofrequency to the SPG of three patients with a medical history of CHs for more than 10 years who had received conservative treatments but shown limited pain relief. In that study, two patients showed complete pain relief and one patient showed partial pain relief with no neurological side effects or complications after the pulsed radiofrequency treatment (PRFT) (11). However, the efficacy and long-term effects of SPG PRFT on CHs remain unclear.
Currently, SPG punctures can be completed under fluoroscopy. As an advanced imaging technology, computerized tomography (CT) provides a more effective guidance for SPG punctures. The objective of the current study was to accurately perform a SPG procedure under CT guidance to preliminarily evaluate the efficacy and safety of SPG PRFT in 16 patients suffering from CHs and to provide an additional treatment strategy for CHs.
Methods
We included 16 (14 males and two females, with a mean age of 44.6 ± 13.9 years, range 15–75 years) consecutive patients with CHs from the Pain Management Center at the Beijing Tiantan Hospital. This study was conducted between April 2012 and September 2013. The study was approved by the Medical Ethics Committee of Beijing Tiantan Hospital affiliated to Capital Medical University (No. kylw-2010-014). All patients provided written informed consent before taking part. The study is registered in the Chinese Clinical Trial Registry and the registration number is ChiCTR-ONRC-12002939.
Inclusion criteria
All the patients matched the classification system for CH diagnosis published in 2004 by the International Headache Society (12). Among the 16 patients in this study, 13 suffered from episodic cluster headaches (ECHs) and three suffered from chronic cluster headaches (CCHs). Each ECH patient was treated within 10 days after the onset of the first symptom of the cluster period (9). All patients received conservative treatments such as rizatriptan or other available drugs in China (verapamil, lithium or steroid) and steroid injections combined with local anaesthetic treatments of the SPG were also performed prior to PRFT. Patients whose numeric rating scale (NRS) scores (on a scale of 0–10, where 0 represents no pain and 10 represents the most severe and unbearable pain) during attacks decreased but were still higher than 7 after conservative treatments were considered intractable.
Exclusion criteria
Patients with abnormal results from routine blood and urinary examinations, kidney and liver functional examinations, blood glucose detection assays, chest X-rays, electrocardiograms (ECG), head magnetic resonance imaging, or head CT scanning were excluded from this study. In addition, patients showing a local infection at the puncture site, taking anticoagulants and/or anti-platelet drugs, carrying a cardiac pacemaker, having psychological disorders or having a history of narcotic drug abuse were also excluded.
Operation
Each patient was placed in a supine position on the CT scan bed with their head turned to the contralateral side (approximately 50°) and had their blood pressure, heart rate, ECG and pulse oximetry continuously monitored. A 21-gauge, 10-cm radiofrequency treatment trocar with a 5-mm active tip (PMF-21-100-5, Baylis Medical Inc., Montreal, Canada) was used for the SPG puncture. The puncture site was located below the ipsilateral zygomatic arch and 3–4 cm in front of the tragus. After local anaesthesia with 1% lidocaine and a small dose (0.05 mg/kg) of intravenous midazolam, the trocar was inserted vertically at an approximate 4 cm depth to reach the bone surface of the lateral pterygoid plate of the sphenoid. The needle was then withdrawn 2 cm and reinserted toward the upper middle third of the pterygopalatine fossa until the needle passed the front edge of the lateral pterygoid plate and was then continuously inserted to a 0.5 cm depth to enter the pterygopalatine fossa. The intraoperative use of thin-slice CT (SOMATOM SIEMENS Company, Munich, Germany) scans (2 mm/layer) multiple time points verified if the puncture needle was located in the correct position in the pterygopalatine fossa. The direction and depth of the puncture needle was adjusted according to the CT images (Figure 1) until it reached the SPG (13). The needle core was then removed and replaced with a radiofrequency electrode (PMK-21-100, Baylis Medical Inc.) connected to a pain management radiofrequency generator PMG-230 (Baylis Medical Inc.) to measure sensory thresholds using 50 Hz electrical stimulation. Electrical currents of 0.1–0.3 V could induce paresthesias of the nasal root, further confirming the accuracy of the puncture (9). The direction and depth of the puncture needle could also be properly adjusted according to the patient’s responses.
(a–f) Consecutive CT scans showing the infrazygomatic approach and the puncture needle gradually reaching the pterygopalatine fossa. The arrow indicates the puncture needle.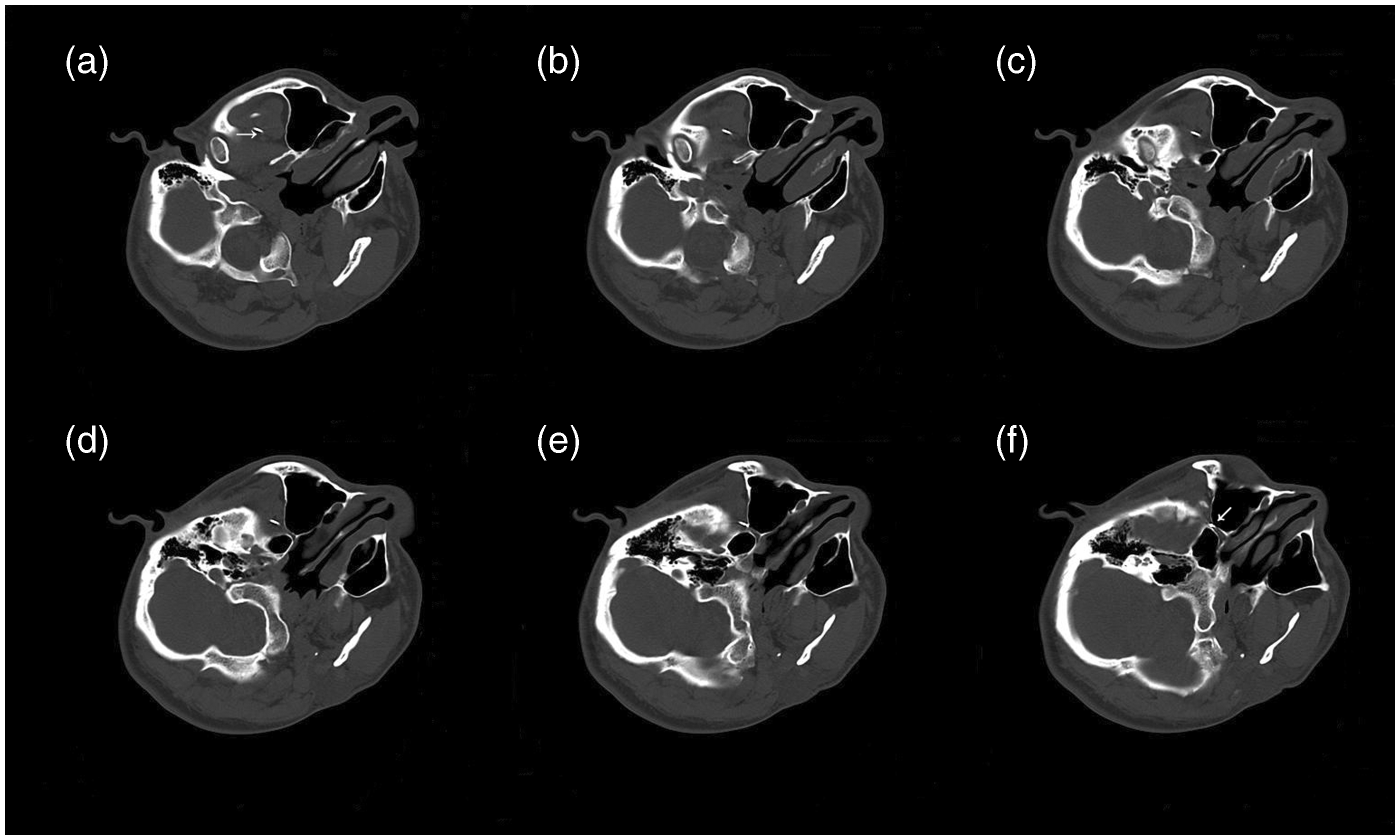
The pain treatment generator was set to pulsed radiofrequency manual mode with a maximum temperature of 42℃. The output voltage was gradually increased until it reached the pain tolerance level of each patient without obvious discomfort (the maximum voltage for the individual); patients were treated twice for 120 seconds each time (14). Following the PRFT, 1 ml of 1% lidocaine with 1 mg dexamethasone was instilled (15). After the PRFT, the dosage of the preoperative drug rizatriptan was adjusted according to the patient’s degree of pain without the use of a CH preventive drug.
Evaluation criteria
The standards for treatment evaluation included three categories. First, complete pain relief was indicated if the CH-associated NRS was 0 and the drug treatment was then terminated. Second, partial pain relief was indicated if the frequency of pain relapse decreased following the operation and the drug requirements were then reduced by 50% compared with the pre-operative dose. Third, no pain relief was indicated if the post-operative pain condition was at the same level as the pre-operative condition (9).
General patient demographics were collected prior to the operation and included sex, age, CH location (left or right), duration of headaches, duration of cluster periods, number of clusters per year, duration of each attack, NRS score during attacks, number of attacks per day and remission period duration. Intra-operative conditions recorded from each patient included the voltage of sensory stimulation, resistance before and after the treatment and intra-operative voltage output. Post-operative telephone follow-up calls with each patient were performed by a trained neurologist to record partial pain remission time, complete pain remission time, duration of this cluster bouts, side effects and complications. The post-operative telephone follow-up was performed on day 1, day 3, day 7, day 14, month 1, month 3, month 6 and year 1 post treatment and then on an annual basis to record the remission time up to finishing this article.
Statistical analysis
SPSS 21.0 statistical software (IBM) was used to perform the data analysis in this study. The normally distributed measurement data are presented as x ± SD, while the non-normally distributed measurement data are presented using median values (minimum to maximum). The cluster period and remission period of patients before and after the treatment were compared using Student’s paired t-test. P < 0.05 was considered to be significantly different.
Results
Clinical features and intra-operative conditions of the patients
Clinical features and corresponding parameters of the CH patients (n = 16) before and during the operation.

: not applicable; CH: cluster headache; NRS: numeric rating scale; PRFT: pulsed radiofrequency treatment.
Treatment effects
Variations in cluster and remission periods of ECH patients’ response to the PRFT.

ECH: episodic cluster headache; PRFT: pulsed radiofrequency treatment.
One ECH patient showed complete pain relief immediately following the operation and a pain relapse 9 months after the operation. Since drug treatment was ineffective with this patient and the patient refused to undergo a SPG blockade treatment, a second PRFT was performed. The symptoms of this patient were alleviated 1 day following the second PRFT and were completely eliminated 3 days after the PRFT. A second pain relapse occurred 11 months after the second PRFT. This patient then received a third PRFT and the pain was also rapidly relieved. At the time of this manuscript writing, the mean duration of the remission period post-PRFT of all the effective ECH patients was significantly longer than pre-PRFT (P < 0.05, Table 2) except those five patients on their first clusters.
Two ECH (15%) and two CCH (67%) patients were not responsive to the SPG PRFT after 1 month following treatment. The two ECH patients were treated with increasing doses of analgesic drugs and consecutive SPG blockades once per week for 4 and 5 weeks respectively and two CCH patients withdrew from the study and continued treatment in a different hospital.
Safety assessment
All patients underwent successful operations with no severe complications or any observable treatment-related side effects.
Discussion
In the current study, the average cluster period of patients suffering from ECHs prior to the PRFT was 2.3 ± 1.0 months and duration between onset of the symptoms and PRFT was less than 10 days, meaning that the cluster period could not end before the treatment. Following the SPG PRFT, 11 ECH patients and one CCH patient showed partial pain relief within 1.3 ± 0.6 days and complete relief within 6.3 ± 6.0 days; these patients were also able to discontinue the use of additional CH medications. These indicate rapid pain relief following PRFT. Specifically, all patients suffering from ECHs were able to rapidly control the pain during the cluster period and effectively promote the remission of the cluster period following PRFT except patients first suffering ECH.
All patients in this study showed poor therapeutic outcomes in response to oral medications or SPG blockades with mixed local anaesthetic and steroids. The majority of the ECH patients (85%) showed rapid pain relief after the PRFT, suggesting that PRFT may be a more effective treatment for ECH patients than more conservative treatments. PRFT is a non-damaging, minimally invasive and safe technique for percutaneous pain management interventions. One ECH patient showed pain relapse after the primary PRFT and refused SPG blockade treatment, yet accepted repeated PRFTs, suggesting that the PRFT may be readily accepted because it shows minimally invasive, safe and effective outcomes.
Drugs for CH prevention often have side effects. In the current study, patients did not take any preventative medication for CHs following the PRFT. During the 12–30-month follow-up period, 11 patients showed positive outcomes after PRFT. Only one of 11 patients (9%) showed pain relapse, at 9 months after the PRFT, which was rapidly relieved and showed significantly longer remission periods following repeated PRFTs. However, 91% of the patients had no pain relapses. Our results indicate that SPG PRFT extended the pain remission period of the majority of the ECH patients and that repeated treatments remained effective for pain relapses.
CHs are classified into episodic and chronic forms. ECH attacks last for several weeks or months and are followed by remission periods of several months or years. CCH attacks occur on an approximate daily basis and persist for more than 1 year without a remission period or with remission periods of less than 1 month. The incidence of CCH is lower than ECH and accounts for approximately 10–15% of CHs (16). The current study assessed only three cases of CCH, of which one showed complete pain relief and two showed no pain relief following the PRFT. Future studies addressing the efficacy of PRFT in CCH patients should be conducted using additional clinical cases.
Chua et al. was the first report of SPG PRFT to successfully treat three patients suffering from CHs (11), while the current study evaluated the efficacy and safety of PRFT for CH patients who showed negative outcomes from conservative treatments. Previous studies have reported that short-term post-operative nose bleeding and cheek hematomas occurred following SPG punctures (9). However, these bleeds did not occur in the current study, suggesting that CT-guided punctures may allow for an enhanced visual space that increases the accuracy of the puncture and avoids surgical-related complications. Destructive SPG therapies may inadvertently cause partial injury to the maxillary nerve in some cases, leading to palate hypoesthesia (9), which is primarily caused by injury to the susceptible maxillary nerve since the anatomically adjacent SPG. The current study used a non-ablative PRFT technique that caused no neurological injury.
The intra-operative imaging-guidance and pre-PRFT electric stimulation to ensure the accuracy of the puncture are crucial to improving the efficacy and reducing the side effects of PRFT. Currently, SPG punctures are primarily performed under the guidance of fluoroscopy. However, CT scanning images are more clear and accurate than fluoroscopy, providing increased accuracy in puncture location details. The current study was conducted using CT guidance to complete a SPG puncture in 16 patients, with a total of 18 intervention treatments and a 100% puncture success rate. The average voltage of the sensory electric stimulation was 0.1 V, indicating that the puncture location was highly accurate.
The mechanisms of SPG PRFT action on CHs remain unclear. The primary peripheral aetiology of CHs is considered to be associated with the SPG (17). A neurolytic agent (ethanol) and radiofrequency procedure cause injury to the SPG (7–9) and, more recently, electrical stimulation of the SPG (4–6) may completely relieve the pain in a proportion of CH patients. However, those destructive therapies lead to side effects since the nerve tissue has been permanently resected. Although electric stimulation therapy does not resect the nerve itself, the stimulator implantation procedure often leads to surgery-related complications. Moreover, the permanent neurolysis and long-term implantation of electrical stimulators are not appropriate for ECH patients who show lengthy remission periods.
Recent studies have suggested that the central nervous system, particularly the hypothalamus, plays an important role in the pathogenesis of CHs (18,19). Thus, electrical stimulation of deep brain structures may activate the hypothalamus and significantly relieve CH symptoms (10). The current study focused only on the PRFT of the peripheral SPG and the majority of the patients showed significant pain relief. Previous authors have speculated that a central activation may be triggered by the peripheral SPG reflex arc (17), so we hypothesized that the PRFT of the SPG may affect the related parts of the central nervous system. Further investigations are required to study the exact mechanisms of this action.
Hence, future random and blind research should be conducted to compare the efficacy of SPG blockades and SPG PRFT to further evaluate if SPG PRFT can replace SPG blockades as the preferred therapeutic intervention technique. The current study reported only the effect of a single PRFT to CH patients. Further studies assessing multiple PRFTs and alterations in treatment parameters that improve PRFT efficacy will be necessary. Moreover, the immediate effect of PRFT on pain attacks should be investigated in future studies. Large sample sizes and long-term follow-up research will be useful to evaluate the efficacy of PRFT in CCH patients.
Conclusion
SPG PRFT is an effective and safe strategy for ECH patients who show negative outcomes following conservative treatments. The early use of SPG PRFT prior to highly invasive surgical therapies may provide another treatment choice for patients suffering from refractory ECHs.
Clinical implications
As CT scanning images are more clear and providing increased accuracy in puncture location details, CT provides a more effective guidance for SPG punctures. CT-guided SPG PRFT is an effective and safe strategy for refractory episodic cluster headache patients prior to more invasive surgical therapies. Further study will be useful to evaluate the efficacy of PRFT in chronic cluster headache patients.
Footnotes
Funding
This work received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.
Acknowledgements
This study was supported by Beijing Municipal Science & Technology Commission (No.Z131107002213061) and High-level Technical Personnel Training Program of the Beijing Municipal Health System (2011-3-034). Both grants equally contributed to the clinical study, data analysis, manuscript writing, etc.