
Abstract
Background
The management of short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT) and with short-lasting unilateral neuralgiform headache attacks with autonomic symptoms (SUNA) remains challenging in view of the limited understanding of their pathophysiological mechanisms.
Methods
An initial observation that patients with both chronic migraine (CM) or cluster headache (CH) and SUNCT/SUNA receiving intravenous dihydroergotamine (IV DHE) had complained of dramatic worsening of the latter led to review of the case notes of patients with CM or CH and co-existent SUNCT/SUNA seen between 2008 and 2013 and who had a trial of IV DHE.
Results
Twenty-four patients were identified. IV DHE was ineffective for SUNCT/SUNA in 16 patients, while one patient reported a marginal improvement. Five patients reported dramatic worsening of the SUNCT/SUNA. Moreover, two patients developed new-onset SUNA during their first IV DHE infusion. Out of these seven patients, those requiring repeated courses of IV DHE consistently experienced exacerbations of SUNCT/SUNA which were suppressed with IV lidocaine.
Conclusions
DHE is an ineffective treatment option for SUNCT and SUNA. Physicians who intend to offer IV DHE to CH or CM patients should warn them that IV DHE could exacerbate and possibly even lead to a de novo onset of SUNCT/SUNA. In view of the reported worsening or new onset of SUNCT/SUNA in patients using dopamine agonists for the treatment of pituitary prolactinomas, we speculate that DHE might worsen or induce SUNCT and SUNA, at least in a sub-group of patients, through a perturbation in the dopaminergic system.
Introduction
Short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT) was first reported in 1978 (1) and more fully described in 1989 (2). After the description in the literature of approximately 50 cases, SUNCT syndrome was encompassed within the trigeminal autonomic cephalalgias (TACs) grouping in the International Classification of Headache Disorders, 2nd edition (ICHD-II) (3). The diagnostic criteria for SUNCT included attacks of unilateral stabbing or pulsating pain centred on the orbital, supraorbital or temporal regions, lasting 5–240 seconds, accompanied by ipsilateral conjunctival injection and tearing, and the frequency of the attacks ranging between three and 200 per day. In recognition of the fact that otherwise similar headache conditions may not have both conjunctival injection and lacrimation, the International Headache Society (IHS) Classification Committee proposed that SUNCT may be a subset of a broader condition called SUNA (short-lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms). In SUNA, there may be cranial autonomic symptoms other than conjunctival injection and lacrimation, or, only one of those symptoms may be present (3). To date only a few case reports and a small series of SUNA patients have been published (4–6), hence the phenotype of SUNA phenotype still needs to be refined. For this reason, the recent ICHD-III beta version diagnostic criteria still keep SUNCT and SUNA as separate entities under the umbrella term ‘short-lasting neuralgiform headache attacks’ (7). It is as yet uncertain whether SUNCT and SUNA are discrete disorders or variants of the same underlying disorder.
Despite being classified within the TACs group, SUNCT and SUNA display demographic characteristics and clinical features overlapping with trigeminal neuralgia (TN). Indeed, it is arguable that SUNCT and SUNA may be better placed amongst the cranial neuralgias rather than the TACs. Moreover, preliminary findings from small series of SUNCT and SUNA patients studied with structural magnetic resonance imaging (MRI) scanning of the trigeminal nerves suggested a high occurrence of neurovascular conflict with the trigeminal nerve ipsilateral to the pain (5,8), with similar percentages to the ones reported in numerous TN series (9,10). These similarities between SUNCT, SUNA and TN have led to open-label trials of preventive treatments used in the latter such as carbamazepine, oxcarbazepine, lamotrigine and intravenous (IV) lidocaine, with meaningful effects in the prevention of SUNCT and SUNA (11,12). Conversely, the medical treatments known to be effective in the other TACs have generally failed to demonstrate convincing responses in SUNCT and SUNA (13).
Dihydroergotamine (DHE) is an effective medical treatment for migraine (14,15). Additionally, there is open-label evidence that supports its use as a transitional treatment in cluster headache (CH) (16,17). To date, there is only one case reported of a SUNCT patient treated with IV DHE in the literature (18). We present the outcome of IV DHE used to treat chronic migraine (CM) and chronic cluster headache (CCH) in a series of patients with co-existent chronic SUNCT or SUNA.
Methods
Intravenous dihydroergotamine (DHE) regimen for chronic migraine and cluster headache.

The study was approved by Northwick Park Hospital Research Ethics Committee, Hampstead London, UK.
Results
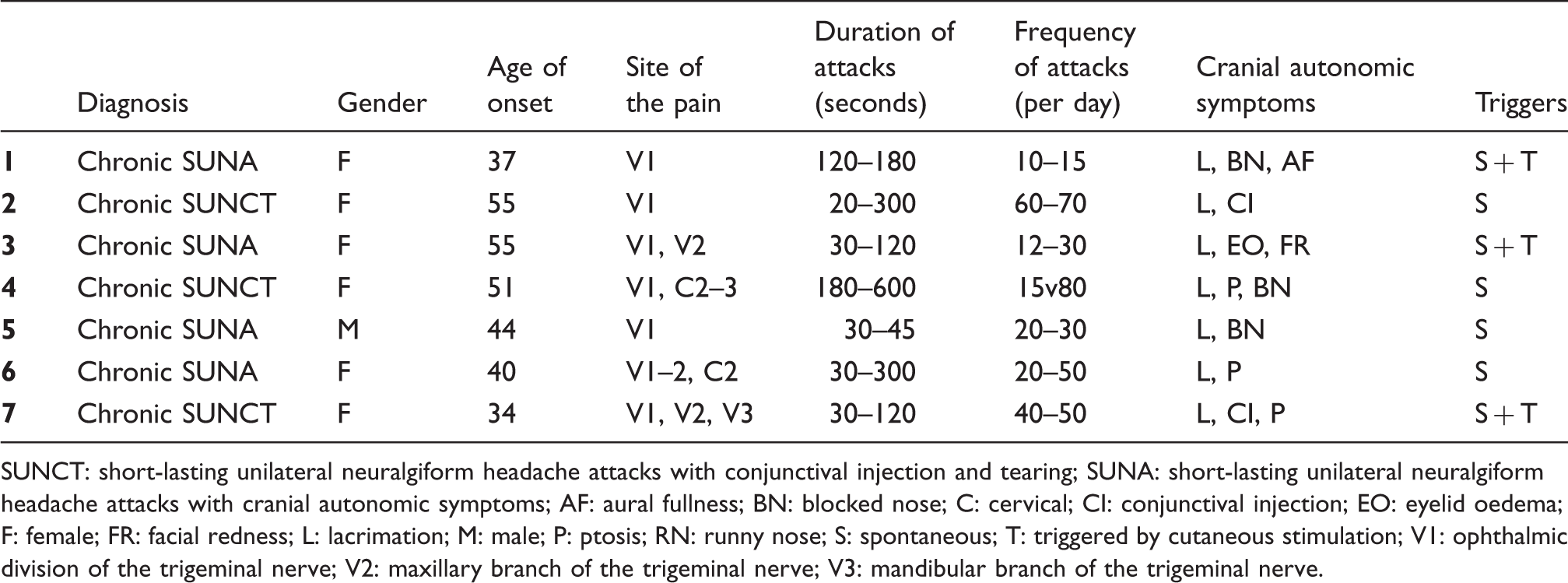
The study group consisted of 24 patients with a diagnosis of chronic SUNCT (n = 8) or SUNA (n = 16) co-existent with CM (n = 19) or CCH (n = 5), who had been treated with IV DHE. All the patients were offered the treatment with the aim of improving their refractory CM or CCH. In 16 out of 24 patients (Table 2), IV DHE had no effect (66.7%); in one patient with CM and SUNCT, IV DHE was significantly effective for the former, but only marginally beneficial for the latter. IV DHE led to a dramatic worsening of the SUNCT/SUNA in five patients, and it triggered a de novo onset SUNA in two patients (n = 7, 29.2%). The main clinical features of the different headaches, investigations, treatments and outcome of IV DHE are summarised in Tables 3 and in Figure 1.
Timing of exacerbation of SUNCT/SUNA during intravenous dihydroergotamine infusion in patients who reported a worsening/new onset of the condition. Principal diagnosis, headache comorbidities and treatment outcome in those whose SUNCT/SUNA did not worsen with intravenous dihydroergotamine. DHE: dihydroergotamine; IV: intravenous; SUNCT: short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing; SUNA: short-lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms; CM: chronic migraine; CCH: chronic cluster headache; SHM: sporadic hemiplegic migraine. Clinical characteristics of SUNCT/SUNA whose headache worsened during intravenous dihydroergotamine. SUNCT: short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing; SUNA: short-lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms; AF: aural fullness; BN: blocked nose; C: cervical; CI: conjunctival injection; EO: eyelid oedema; F: female; FR: facial redness; L: lacrimation; M: male; P: ptosis; RN: runny nose; S: spontaneous; T: triggered by cutaneous stimulation; V1: ophthalmic division of the trigeminal nerve; V2: maxillary branch of the trigeminal nerve; V3: mandibular branch of the trigeminal nerve.

Patient 1
A 41-year-old woman was referred to our headache service in 2008 for a headache disorder that fulfils the criteria for CM. Unfortunately she failed trials of propranolol, amitriptyline, dosulepin, topiramate, sodium valproate, gabapentin, pregabalin, flunarizine and methysergide. Bilateral greater occipital nerve blocks were moderately effective for three to four weeks. She was offered the first IV DHE treatment in 2009. This led to a complete suppression of the migraine for six weeks. Given the limited management options, the treatment had been repeated every three to four months since.
In 2010, with no precipitant triggers, a new headache began. It was characterised by strictly unilateral very severe, stabbing and sharp headache attacks in the ophthalmic division of the trigeminal nerve. The attacks were lasting two to three minutes and they were occurring 10–15 times/day. The attacks were associated with ipsilateral lacrimation, blocked nose and aural fullness. They followed a serrated pattern and they could occur spontaneously as well as triggered by eating, talking and cold wind blowing on her face. There was no refractory period after the triggered attacks. An MRI scan of the head with pituitary and trigeminal views was normal. The headache phenotype fulfilled the ICHD-II criteria for chronic SUNA, in view of the lack of any significant remission periods since (3). The patient developed a cutaneous rash on lamotrigine and had to discontinue it. Topiramate and gabapentin were tried again to no avail. Oxcarbazepine was marginally effective, but she became sleepy and nauseated while on it. Duloxetine was ineffective.
In December 2010 she had a further course of IV DHE for her CM. While the CM improved similarly to the previous times, she experienced a dramatic worsening of the SUNA attacks from day 4 (cumulative DHE dose: 9.25 mg), with three to four attacks/hour lasting two to three minutes each, both spontaneous and triggered by cutaneous stimulation, which disrupted her regular eating and intake of fluids. This exacerbation of SUNCT lasted for two weeks, before the headache gradually subsided. Subsequently, she had three more courses of IV DHE, as it was the only effective treatment for the migraine, followed by seven days of IV lidocaine (1.5–3.5 mg/kg/h) due to the consistent worsening of the SUNA. An occipital nerve stimulator (ONS) was implanted in 2012 with dramatic improvement of the SUNA and 50% reduction in migraine days.
Patient 2
A 58-year-old woman presented to our headache service in 2010 with a nine-year history of a chronic daily headache fulfilling the ICHD-II criteria for CM (3). She had trials of propranolol, atenolol, amitriptyline, gabapentin, pregabalin, topiramate, methysergide and onabotulinum toxin type A, with no appreciable improvement. She was therefore admitted for a course of IV DHE in May 2011. She derived a 50% reduction in migraine days from the infusion for a period of six weeks. The treatment was repeated four months later with expected initial improvement in the migraine. However, a new headache started from day three (cumulative DHE dose: 6.25 mg). The headache was strictly unilateral, centred over the right retro-orbital region, with 60–70 attacks/day, lasting between 20 and 300 seconds and associated with marked ipsilateral lacrimation and conjunctival injection. The attacks were all occurring spontaneously, following a single-stab or a repetitive-stabs pattern. The new headache phenotype fulfilled the ICHD-II criteria for SUNCT. The DHE infusion was discontinued and the patient was started on IV lidocaine for seven days, with suppression of the attacks during the infusion and for the following two weeks. Subsequently the headache relapsed, leaving the patient with daily SUNCT attacks since then. A 50% reduction in attack frequency was achieved on lamotrigine 500 mg/day. Disappointingly, trials of topiramate, oxcarbazepine, gabapentin, greater occipital nerve block, lacosamide and zonisamide did not produce any further benefit.
In view of the fact that DHE was the only treatment providing transient but significant improvement of her CM, she had four further IV DHE treatments four months apart, which consistently led to a dramatic worsening of the SUNCT attacks from days 3–4 of the infusion that were treated with a seven-day course of IV lidocaine.
Patient 3
A 60-year-old woman was referred to our headache service for the management of a headache disorder which started at the age of 33 with the features of chronic cluster headache (CCH). For 17 years the condition followed an episodic pattern, with two bouts per annum of daily attacks lasting six to eight weeks. From 2004 onwards the patient began experiencing daily or nearly daily attacks with no significant remission periods. The headaches were strictly unilateral on the right, centred over the ophthalmic and mandibular trigeminal territories. The attacks were very severe and occurred three to four times daily, usually at 3:45 a.m., 8 a.m. and 10 a.m., lasting two to three hours (if not treated). The pain was accompanied by ipsilateral lacrimation, conjunctival injection, eyelid oedema, rhinorrhoea and facial sweating. Triggers included alcohol, warm environment and the smell of volatile substances. The CH was managed with a combination of verapamil, topiramate and three monthly greater occipital nerve blocks. However, in 2009, with no precipitating triggers, a new headache began. It was characterised by 12 to 30 severe attacks/day of a right side (rarely left side) stabbing pain centred over the periorbital and temporal areas. The attacks lasted between 30 and 120 seconds and were accompanied by ipsilateral lacrimation, eyelid oedema, facial redness and facial sweating. The attacks could occur spontaneously or could be triggered by cutaneous/intraoral stimulation. There was no refractory period following triggered attacks. The headache displayed a chronic pattern from onset. Paroxysmal hemicrania was ruled out with an indometacin test and a diagnosis of chronic SUNA was made. Lamotrigine at high dose as well as carbamazepine and oxcarbazepine did not produce any meaningful benefit. Duloxetine 120 mg/day led to a 50% reduction in the SUNA attack frequency. An MRI scan of the head with pituitary and trigeminal sequences was normal.
In July 2010 she was admitted for an IV DHE treatment for her CCH. Although the CH attacks subsided for eight weeks after discharge, the SUNA attacks worsened dramatically from day 4 of infusion. The attack frequency increased to 60/day on day 4 and for the following two weeks, before they settled. Three months later she had the second IV DHE treatment, which similarly to the first, led to a worsening of the SUNA attacks from day 4. The patient was commenced on IV lidocaine for seven days with complete suppression of the SUNA attacks. Since then, she had further five IV DHE treatments, three months apart, followed by IV lidocaine for seven days, as soon as the SUNA worsened. Since 2012, her SUNA and CCH have been successfully managed with an ONS.
Patient 4
A 55-year-old woman was referred to our headache service for the management of a headache disorder that started at the age of 40 and became progressively more frequent, until it was occurring on a daily basis. At that time she used to take codeine and paracetamol on a daily basis. The headache had the features of CM and medication-overuse headache (MOH). The withdrawal of pain killers led to an improvement of the background headache, though she was still left with more than 15 headache days/month. Pizotifen, propranolol, amitriptyline, gabapentin, topiramate, flunarizine and greater occipital nerve blocks helped only marginally. The CM was managed with a combination of sodium valproate (2 gm daily) and pregabalin (600 mg daily) with partial benefit.
In 2010 a new headache disorder, fulfilling the IHS diagnostic criteria for SUNCT, began. The headaches were strictly unilateral on the left side, centred over the retro-orbital region and radiating to the occiput. She described 15–80 stabbing and shooting, very severe attacks/day, lasting between three to 10 minutes, mainly following a serrated pattern. The attacks were associated with ipsilateral lacrimation, conjunctival injection, blocked nose, aural fullness, facial sweating and ipsilateral photophobia. There were no clear triggers. The SUNCT attacks have been occurring on nearly daily basis with no significant remissions since the onset, suggesting a chronic form. She experienced a skin rash on low dose of lamotrigine. Oxcarbazepine and topiramate did not produce any benefit. Duloxetine 90 mg provided a meaningful reduction in her SUNCT attacks down to three to five episodes/day. An MRI scan of the head with pituitary and trigeminal sequences was unremarkable.
In 2011 she had her first IV DHE treatment for CM management. The headache improved during the infusion and she obtained a 70% reduction in headache days, according to her headache chart, for further six weeks after discharge. The SUNCT attacks remained unchanged. In 2012 she repeated the DHE infusion treatment. From day 3 (DHE cumulative dose: 6.25 mg) she went into a ‘SUNCT status’, with multiple attacks per hour occurring relentlessly throughout the day for 10 days, before they subsided. She had IV DHE treatments two more times since, followed by IV lidocaine for seven days to control the SUNCT worsening.
Patient 5
A 46-year-old man was assessed in our headache clinic for the management of CCH, which began at the age of 43 with no precipitants. The CH attacks were purely occurring on the right side centred over the peri-orbital and retro-orbital regions. He has been experiencing five to six attacks/day (mainly at 2 a.m., 8 a.m., 3 p.m. and 10 p.m.), lasting 60–90 minutes if not treated and associated with ipsilateral lacrimation, conjunctival injection, ptosis, rhinorrhoea, blocked nose, restlessness, nausea, photophobia and phonophobia. His CH management included high-dose and flow oxygen for the acute attacks (he could not tolerate sumatriptan 6 mg injections) and verapamil 960 mg, which was moderately effective for CH prevention. The negative indometacin trial ruled out indomethacin-responsive headaches. An MRI scan of the head showed an arterial (superior cerebellar artery) loop pressing on the trigeminal nerve ipsilaterally to the side of the pain.
In view of the disappointing response to lithium, topiramate, methysergide, sodium valproate, melatonin, baclofen, greater occipital nerve blocks, which were beneficial for a week only, he was offered an admission for IV DHE. During the infusion period he did not experience any CH attacks, but remarkably, at day 5, after the last DHE dose (cumulative dose: 10.25 mg), he started complaining of a new-onset headache with the features of SUNA. The pain was located at the same distribution of the CH attacks, but described as a stabbing, electric-shock type pain, occurring in very short-lived severe attacks, lasting 30–45 seconds (attacks were timed on the ward), occurring every two to three minutes, accompanied by ipsilateral lacrimation and blocked nose. A few hours later the patient was commenced on IV lidocaine, with complete resolution of the SUNA attacks by day 7 and no further attacks for the following 10 days. Subsequently the SUNA attacks relapsed and have been occurring regularly since. The patient is currently managing the SUNA and the CH attacks with oral preventive treatments and ONS.
Patient 6
A 44-year-old woman has been under our care for two types of chronic daily headaches possibly secondary to a craniopharyngioma operated at the age of 7. The first headache condition has the features of CM complicated by medication overuse. The second headache type fulfilled the ICHD-II criteria for chronic SUNA. The latter was characterised by unilateral but sided-alternating severe stabbing headache attacks, centred over the forehead and radiating to the occiput, lasting 30 seconds to five minutes and occurring between 20 and 50 times/day. There were no clear-cut triggers for the attacks. The attacks were accompanied by ipsilateral lacrimation and ptosis. She failed to respond or tolerate trials of amitriptyline, propranolol, topiramate, lamotrigine, oxcarbazepine, carbamazepine, duloxetine, pregabalin, gabapentin, mexiletine and lacosamide, while greater occipital nerve blocks produced only a transient beneficial response. Over time she had a few MRI scans which showed stable post-operative changes. Her pituitary function tests showed slightly reduced thyroid-stimulating hormone (TSH) levels.
In 2010 she underwent her first IV DHE treatment, which was highly beneficial for the CM, with 60% reduction in headache days for three weeks. However, from day 3 of DHE infusion, her SUNA attacks worsened dramatically, from a baseline of 20/day (last two weeks prior to IV DHE), to approximately 80–100 on day 3. For this reason she was started on IV lidocaine for eight days, which led to an 80% reduction in the SUNA attacks frequency. She had further five IV DHE treatments every four months, followed by seven days of IV lidocaine to suppress the consistent worsening of the SUNA attacks.
Patient 7
A 39-year-old woman was referred to our service for the management of a chronic headache disorder which fulfilled the ICHD-II criteria for CM (3). In 2009, with no precipitants, a new headache developed. The headache was strictly unilateral on the right side, with severe stabbing attacks centred along the jaw and radiating to the eye and temple. Initially the attack frequency was low, though over time it worsened, with 40–50 attacks occurring most days. The attack duration ranged between 30 and 120 seconds. Cranial autonomic features associated with the attacks included ipsilateral lacrimation, conjunctival injection and ptosis. The attacks could occur spontaneously, but could also be triggered by chewing, talking, brushing teeth and wind blowing on her face. There were no remission periods. An MRI scan of the head with pituitary and trigeminal sequences showed an arterial loop distorting the trigeminal nerve ipsilaterally to the side of the pain. A diagnosis of chronic SUNCT was made. The combination of lamotrigine and topiramate led to a significant improvement for the SUNCT, though it only marginally helped the CM. However, other preventive treatments including amitriptyline, gabapentin, pregabalin, sodium valproate and greater occipital nerve blocks proved to be ineffective or not tolerated. For this reason, a trial with IV DHE was offered. During the infusion period and for the subsequent eight weeks after discharge, the migraine improved significantly. From day 4 (cumulative DHE dose: 9.25 mg), the SUNCT attacks frequency worsened dramatically to approximately 120 attacks on day 4 and ranging between 100 and 150 during the subsequent two weeks, before they subsided. The patient had five further IV DHE treatments, three months apart, with similar outcome and therefore the DHE treatment was always followed by seven days of IV lidocaine, which promptly suppressed the SUNCT exacerbation.
Discussion
We describe the outcome of IV DHE in a series of 24 CM or CCH patients with coexistent SUNCT or SUNA syndromes, detailing the clinical scenarios of seven patients in whom IV DHE consistently led to a dramatic exacerbation of the latter.
SUNCT and SUNA syndromes have frequently been reported in comorbidity with migraine. In a prospective series by Cohen et al., 35% of SUNCT and 67% of SUNA patients had a personal history of migraine (4). The coexistence of SUNCT, SUNA and hemiplegic migraine has been described in another case series. Four of these patients also had chronic migraine (6). It has been suggested that the coexistence of SUNCT, SUNA and a personal or family history of migraine (migraine biology) may account for some clinical features such as the development of a background continuous pain in some SUNCT and SUNA patients (4). Conversely, the coexistence of SUNCT and CH in the same patient has rarely been described. To our knowledge two patients with concomitant SUNCT and CH have been reported (19,20). In both cases the SUNCT syndrome followed the onset of CH. Similarly, amongst our four patients with coexistent CCH and SUNCT or SUNA, the latter followed the onset of the former disorder and then the two conditions coexisted with attacks of SUNCT/SUNA and CH occurring on the same side of head. It has been postulated that a dysfunction in the posterior hypothalamus gives rise to a central permissive state playing an important role in terminating the attacks in the TACs rather than triggering them (21). It is therefore possible that, especially in the chronic forms of TACs, such as CCH, the persistent derangement of the hypothalamic function may facilitate the occurrence of different disorders within the TACs spectrum, thus explaining the coexistence of CCH and SUNCT/SUNA.
IV DHE has a long history of efficacy in CM, including the medically intractable forms as showed in several open-label and retrospective trials (14,15). IV DHE has also been reported to be effective in CH. Open-label studies in episodic and chronic CH suggested a rapid and sustainable efficacy in the vast majority of patients (16,17). However, little is known with regard to the efficacy of DHE in the other TACs (22). To the best of our knowledge, only one case of a SUNCT patient who failed to respond to IV DHE (3 mg) has been reported (18). In view of the lack of any published data supporting the efficacy of DHE in SUNCT and SUNA, it is not routine practice to treat these patients with IV DHE. We therefore studied a group of patients who tried IV DHE for the management of their refractory CM or CCH who also suffered with SUNCT or SUNA.
While IV DHE led to a remarkable improvement of the baseline primary headache (CM or CCH) in a significant proportion of our refractory patients, it was essentially ineffective in SUNCT and SUNA. Furthermore, in almost a third of our patients IV DHE improved the baseline headache disorder but led to consistent exacerbations of the SUNCT/SUNA condition. These findings suggest that DHE may not represent an effective treatment option for SUNCT and SUNA syndromes; therefore, it should not be considered amongst the armamentarium of transitional treatments for these conditions. Physicians should be careful about administering IV DHE in patients with SUNCT and SUNA as it can worsen these syndromes; additionally, all patients receiving this treatment should be cautioned that IV DHE can lead to de novo onset of SUNCT/SUNA.
Interestingly, none of the patients who did not benefit from DHE reported a worsening of the SUNCT/SUNA. This may be purely coincidental. It would be rather unlikely that the improvement of the baseline CM or CCH has simply unmasked the coexistent SUNCT/SUNA syndromes, leading to a consequent amplification of the latter. The concomitant coexistence of more than one primary headache disorder in the same individual is usually characterised by a specific response to diagnosis-specific treatments, allowing clear differentiation between headache disorders (20).
Conversely, it may be possible that certain DHE neurochemical effects are responsible for the exacerbations of SUNCT and SUNA during infusion. DHE has a complex pharmacology. It interacts with multiple receptors, including serotonin, dopamine and α-adrenoceptors, with different degrees of affinity (23). Preclinical studies have demonstrated the ability of DHE to prevent the development of neurogenic inflammation in the dura by blocking the peripheral C or A-delta fibres (24). This effect, similar to the mode of action of triptans (25), is thought to be facilitated by the high affinity of DHE for 5-HT1B and 5-HT1D receptors located on the dural sensory fibres (26). DHE has been shown to be able to bind to central nervous system structures, including the brainstem, dorsal horn of the cervical spinal cord and the cerebral cortex (27), as well as possibly acting within the trigeminal nucleus caudalis to inhibit trigeminal neuron activity (28). The inhibition of peripheral and possibly central sensitisation via modulation of serotoninergic circuits may explain DHE efficacy in migraine and partly also in CH.
SUNCT and perhaps SUNA pathophysiology is thought to be similar to CH and the other TACs, involving a derangement in the hypothalamic-trigeminal circuits, perhaps leading to an abnormally activated trigemino-autonomic reflex (18). Nonetheless, neither IV DHE, nor subcutaneous sumatriptan 6 mg, which are highly effective in CH (17,25), seem to display any effect in SUNCT/SUNA syndromes (12). It could be argued that the enhanced neuronal serotoninergic tone produced by DHE might be of only marginal importance in SUNCT/SUNA pathophysiology, thus explaining why DHE is ineffective. However, other mechanisms might help explain the opposite therapeutic response of DHE in CH compared to SUNCT/SUNA.
Ergot alkaloids are potent dopamine receptors agonists, with full intrinsic activity at D2 and D3 receptors whereas they are fairly weak antagonists or partial agonists at D1 receptors (23). Dopaminergic pathways are thought to play an important role in the pathophysiology of primary headaches (29) including CH, where a downregulation of hypothalamic dopaminergic neurons has been demonstrated in endrocrinological studies (30). Hence one possible hypothesis is that dopamine agonists, such as DHE, might help restore the decreased sensitivity of dopaminergic neurons in the hypothalamus in CH patients.
The role of the central dopaminergic system in SUNCT and SUNA is unknown. Dopamine agonists including bromocriptine (31–33), lisuride (32), quinagolide (33,34) and cabergoline (32,34,35) have been reported to induce SUNCT attacks in patients with pituitary prolactinoma. The worsening effect of DHE in some of our patients could support the importance of neuroendocrine mechanisms involving the dopamine-prolactin axis in modulating SUNCT and SUNA. However, none of our patients had neuroradiological or laboratory evidence of prolactinoma or hyperprolactinemia. Nonetheless our findings raise the possibility that perturbations in the dopamine-prolactin axis may be important even in primary SUNCT/SUNA syndrome. It is conceivable that specific neuroendocrine pathways involving the hypothalamic dopaminergic neurons may be capable of activating SUNCT pathophysiology at least in a subgroup of patients. According to this hypothesis, antidopaminergic drugs may then be useful in at least a sub-group of SUNCT and SUNA patients, by restoring the balance in the dopamine neurons. However, there are no data in the literature on this subject. In this study, domperidone was used in variable daily doses for the management of nausea, not only by all the patients who worsened with IV DHE, but also by the remaining patients included in this study. Moreover, domperidone only minimally penetrates the blood-brain barrier, so it would be difficult to postulate any involvement of this drug in the worsening of the SUNCT/SUNA attacks in our patients. Metoclopramide was rarely needed by most of our patients.
One of the caveats of this study includes its retrospective design. However, patients who required courses of IV DHE and reported exacerbations of SUNCT/SUNA whilst on treatment were assessed with daily clinical observations during admissions. Additionally, their headaches pattern was monitored with prospectively filled headache diaries. A second caveat concerns the study group. The coexistence of SUNCT/SUNA with the chronic forms of migraine and CH in the same patient is rare. Findings on the management strategies of these rare and complex cases may be of interest mainly for physicians working in tertiary headache centres.
Conclusion
We describe a case series of patients with CM or CCH and SUNCT/SUNA treated with IV DHE. This study highlights a few novel clinical findings with potentially meaningful pathophysiological implications. DHE does not seem to be an effective treatment option for SUNCT and SUNA syndromes. Physicians who consider IV DHE as a treatment approach in cases of refractory CM or CCH co-existent with SUNCT/SUNA should be aware of the possibility that the treatment could lead to an exacerbation of the latter. These clinical phenomena may be due to an increased dopaminergic tone secondary to high doses of IV DHE that possibly perturbs neuroendocrine mechanisms, namely the dopamine-prolactin axis, which may represent an important pathway in SUNCT and SUNA neurobiology.
The different outcome of DHE in CH and SUNCT/SUNA might strengthen the hypothesis, based on epidemiological, clinical, radiological and therapeutic aspects (36), that SUNCT/SUNA and CH may have differing underlying neurobiological substrates. One of the key differences between the two disorders may indeed involve the cerebral dopamine system. Whereas in CH, enhancing the dopamine tone may help restore the balance of downregulated hypothalamic dopaminergic neurons, in SUNCT/SUNA it may wind up certain neuroendocrine pathways, leading to headache exacerbations.
Clinical implications
Intravenous dihydroergotamine does not seem to be an effective treatment option for short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT) and short-lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms (SUNA) syndromes. Physicians who consider intravenous dihydroergotamine as a treatment approach in cases of refractory chronic migraine (CM) or chronic cluster headache (CCH) co-existent with SUNCT/SUNA should be aware of the possibility that the treatment could lead to an exacerbation of the latter. An increased dopaminergic tone secondary to high doses of intravenous dihydroergotamine may perturb neuroendocrine circuits, namely the dopamine-prolactin axis, which may represent an important pathway in SUNCT and SUNA neurobiology.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest
GL has received payment for the development of educational presentations from Allergan and ElectroCore. PS has nothing to declare. MSM serves on the advisory board for Allergan and St Jude Medical, and has received payment for the development of educational presentations from Allergan, Merck Sharpe and Dohme Ltd and Medtronic.