
Abstract
Background
Headache is a common condition, and a common complaint leading patients to emergency departments (ED). There have been a number of studies of the effect of environmental factors on headache, such as weather and air pollutants.
Methods
This retrospective cohort study included data on daily ED visits with a chief complaint of headache in Soroka University Medical Center (SUMC) during 2002–2012. Data on weather and air pollutants were obtained from monitor station in Be'er-Sheva. To estimate the short-term effects of air pollution and temperature on number of daily headache ED visits, we applied generalized linear mixed models (GLMM).
Results
A total of 22,021 ED visits were included in the analysis. An increase in 5℃ in temperature was associated with an increase in ED visits, relative risk (RR) = 1.042, (95% CI 1.009; 1.076). RR for headache was associated with an increase in 10 units of nitrogen dioxide (NO2), RR = 1.110 (95% CI 1.057; 1.167), with a higher effect for older patients.
Discussion
The current findings give evidence of an association between air pollution, weather and ED visits for headache, especially for NO2. Short-term increases in air pollution exposure may trigger headache by increasing pulmonary and systemic inflammation, increasing blood coagulability or altering endothelial function.
Introduction
Acute headache is a common condition, and a common presenting complaint in patients at emergency departments (ED). It is estimated that 1%–3% of all ED visits are due to non-traumatic headache (1). Intracranial pathology is found in only a small minority of these patients (3.5%–10.1%) (2) and most of them suffer from primary headache disorders.
Research directed at identifying precipitating factors for headache episodes in both disorders (commonly referred to as “triggers”) identified several potential factors such as: menstrual changes, afferent stimulation, physical activity, psychological factors, sleep disorders, dietary factors and multiple environmental factors, such as weather, noise, electromagnetic fields, environmental lighting, visual stimuli, odors, cigarette smoke and air pollutants (3–8).
There have been a number of studies examining the effect air pollution on headache (9,10). Szyszkowicz (11) examined 8012 ED visits for headache recorded in Ottawa. This analysis revealed that ED visits for headache are associated with an increased concentration of anthropogenic air pollutants (sulfur dioxide (SO2), nitrogen dioxide (NO2) and carbon monoxide (CO)).
In this study, we investigated the role of meteorological parameters and air pollutants as headache triggers in the hot and arid geographic region of southern Israel.
Materials and methods
Study population
We obtained data on daily ED visits to Soroka University Medical Center (SUMC) with a primary complaint of headache in patients 18 years or older during the 10-year period (between December 1, 2002 and December 31, 2011). SUMC is a tertiary 1000-bed hospital and the only medical center area serving a population of 700,000 of Southern Negev. The annual adult ED visits volume is ∼100,000. We excluded from the analysis all cases that were hospitalized following the ED visit. The analyses for air pollution were restricted only to the residents of Be’er-Sheva (main city in the region, population 215,000), where data from monitor stations were available. The analyses for meteorological factors were analyzed for residents of all of the southern Negev.
Environmental data
Data on meteorological parameters (temperature and relative humidity) and air pollutants were obtained from the monitoring station in Be’er-Sheva operated by the Ministry of Environmental Protection. This is the only monitoring station in the area, which measures all pollutants simultaneously in 20-minute intervals. Historical data for the entire study period include particles with median aerodynamic diameter of 10 µm or less (PM10) concentrations (µg/m3) over time along with NO2 (parts per billion (ppb)) and SO2 (ppb) and average, minimum and maximum temperature (℃). Seasons were defined according to the Alpert et al. synoptic definition (12), where winter and the summer each last approximately four months (three months and 23 days), and the autumn and spring each last nearly a half of this period, 75 days and 61 days, respectively.
Desertification and global warming trends pose significant global ecological and environmental problems (13); e.g. land degradation processes resulting in increasing exposure of population to dust sources in arid and semiarid soils and possible dust storms (14). The Negev region is located between the Saharan and the Arabian deserts (the world’s largest dust belt) and every year is exposed to several intensive dust storms (15,16). A dust-storm (DS) day was defined as a day with an averaged PM10 concentration that was two standard deviations (SD) above the background value and was equal to 71 µg/m3 (16).
Statistical analysis
Data were summarized using frequency tables for categorical variables and summary statistics (mean with SD) for continuous variables. To estimate the short-term effects of air pollution and temperature on number of daily headache ED visits, we applied a generalized linear mixed models (GLMM) methodology described by Szyszkowicz (17). This technique is based on Poisson regression applied to clustered counts. Poisson random-effects models were applied to analyze the cluster counts where the groups of days, determined by the triplet (day of the week, month, year), form the clusters. The hierarchical construction of the clusters allows the model to incorporate level-specific random effects. The behavior of an individual is associated with this hierarchical structure and by consequence many health outcomes are cluster dependent. We used the glmmPQL function from the R statistical package to perform the analysis (17). Relative risk (RR) with 95% confidence intervals (CIs) represent the risk of ED visits for headache associated with an increase in average of pollutant concentration. Each pollutant (PM10, NO2 and SO2) was examined in a separate model, adjusted for temperature and relative humidity. The dust-storm variable was treated as a dichotomous yes/no variable based on occurrence on a given day. For testing possible nonlinear association with temperature variable, we used penalized splines with five degrees of freedom. Additionally, we stratified our analysis by gender and by season (summer, fall, winter and spring). P values less than 0.05 were considered statistically significant.
Results
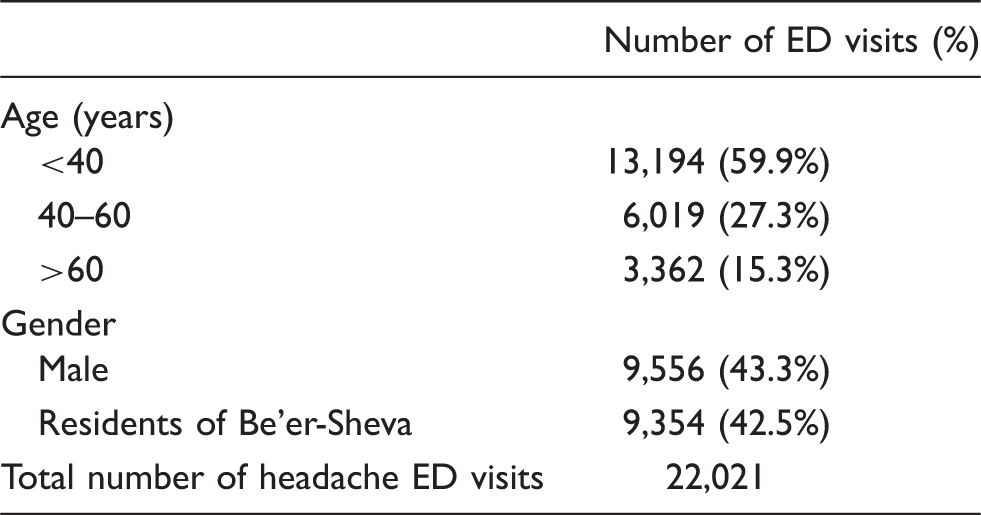
Frequency of emergency department (ED) visits for headache.
Mean, SD of daily levels of air pollutants, meteorological factors and daily numbers of ED visits for headache.

Study period: January 1, 2002–December 31, 2011. CO: carbon monoxide; ED: emergency department; IQR: interquartile range; NO2 = nitrogen dioxide; SO2 = sulfur dioxide; PM10 = particles with median aerodynamic diameter of 10 µm or less; ppb: parts per billion.
Effect of temperature on the incidence of headache ED visits
A positive association was found between an increase in five units of temperature in ℃ and incidence of ED visits for headache (Figure 1): For all cases, RR (1.042, 95% CI 1.009; 1.076, p = 0.005), for the fall seasons, RR (1.052, 95% CI 1.004; 1.102, p = 0.034) and winter season, RR (1.063, 95% CI 1.034; 1.125, p = 0.038) (Figure 2). Higher associations were observed one day after the exposure during the fall and winter seasons only, RR (1.063, 95%CI 1.015; 1.114, p = 0.010) and RR (1.084, 95% CI 1.023; 1.148, p = 0.006).
Change in number of daily emergency department (ED) visits for headache associated with daily average temperature (℃). The effect of short-term increase in temperature on emergency department (ED) visits for headache, by season.

Effect of anthropogenic air pollution on the incidence of headache ED visits
The association between air pollution and incidence of headache in the city of Be’er-Sheva by pollutant and season is presented in Figure 3. The strongest effect was observed between an increase in NO2 (10 units) and headache visits incidence. For all cases the RR for headache visit on the same day was 1.11 (95% CI 1.057; 1.167, p < 0.001). Analysis stratified by season revealed that ED visits for headache were significantly associated with increase in 10 units of NO2 in the winter and spring seasons (RR = 1.18, 95% CI 1.45; 1.19, p = 0.001 and RR = 1.32 (95% CI 1.12; 1.56, p = 0.001 respectively), but not during the summer and fall, respectively.
The effect of short-term increase in pollutant concentrations on emergency department (ED) visits for headache, by season.
Effect of particulate matter air pollution on the incidence of headache ED visits
An association between PM10 and ED visits on the same day was found during the fall season, RR for increase in 10 units of PM10 = 1.01(95% CI 1.00; 1.02, p = 0.006). This association was immediate and did not remain the day after the exposure. No significant association between dust-storm days and ED visits was found, but a positive association was shown during the winter and fall season.
Associations for ED visits for age and gender groups
Relative risk of headache emergency department (ED) visits associated with increase in pollutant concentrations by age, gender.
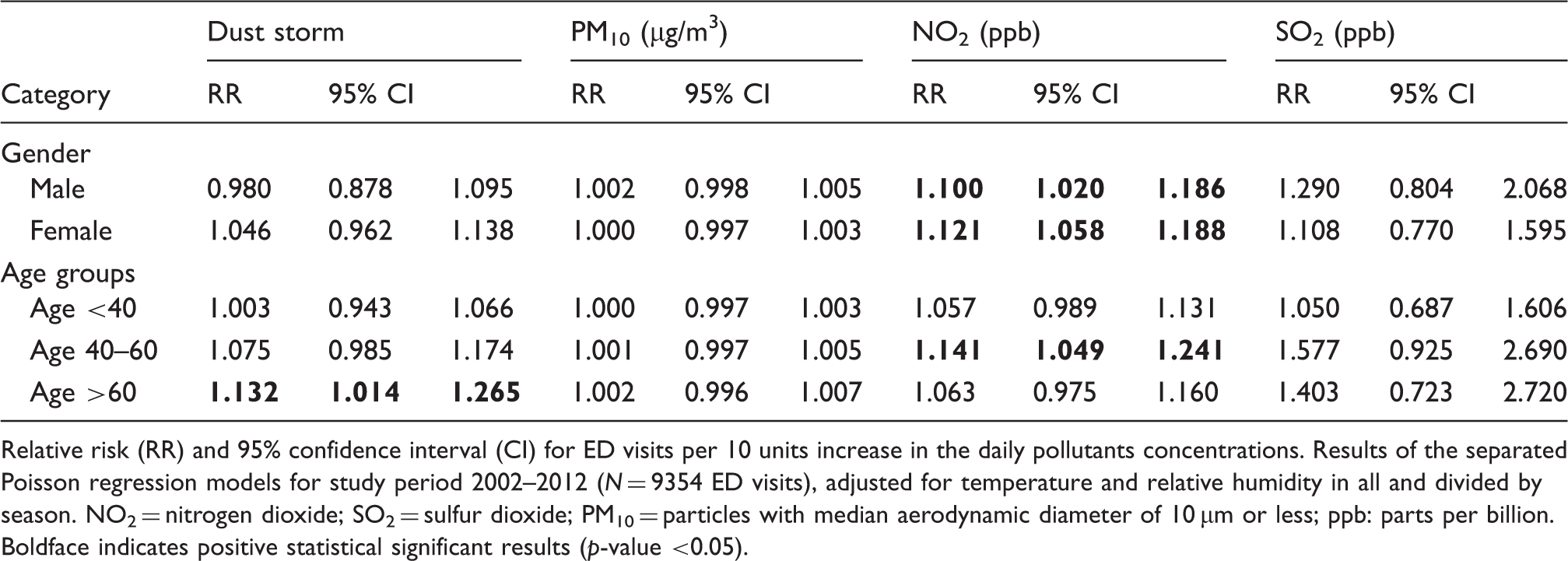
Relative risk (RR) and 95% confidence interval (CI) for ED visits per 10 units increase in the daily pollutants concentrations. Results of the separated Poisson regression models for study period 2002–2012 (N = 9354 ED visits), adjusted for temperature and relative humidity in all and divided by season. NO2 = nitrogen dioxide; SO2 = sulfur dioxide; PM10 = particles with median aerodynamic diameter of 10 µm or less; ppb: parts per billion. Boldface indicates positive statistical significant results (p-value <0.05).
Discussion
In this analysis of more than 22,000 visits with headache to the ED, we have assessed the short-term effects of meteorological and air pollution factors. We have found that an increase in temperature and NO2 was associated with increased risk of headache ED visits. This effect of the ambient temperature was particularly evident during colder seasons (winter and fall). The effect of NO2 and dust storm increased with age.
Headache is a common cause for ED consultations, the majority of which ((∼60%) are diagnosed as primary headaches, especially tension type and migraine (19–21). Similar to our cohort, the ED-consulting headache patients are relatively young (<40 years) and predominantly women (>60%).
Primary headache disorders are believed to be influenced by weather factors (22,23), and higher rates of migraine attacks were found during warmer seasons (24). Nevertheless, larger time series studies of ED headache visits demonstrated conflicting results. Two studies performed in Canadian EDs did not reveal any association (25) while a 7.5% higher risk for headache ED visits with each 5℃ increment in temperature was found in an ED in Boston, Massachusetts, United States (US). Another study conducted in Boston (23) showed in a case-crossover study of 7054 patients that a higher mean ambient temperature in the 24 hours preceding hospital presentation positively and linearly increased the acute risk of headache, and that higher risk was observed for cases between October and March or between April and September. Our findings are in accordance with the studies performed in Boston.
The differential effect of temperature changes between seasons is not clear. Possibly, physiological acclimatization to very high temperatures during the hot seasons somewhat attenuates the effect of temperature changes on headaches incidence during the hot seasons. Another possible explanation can be the wide use of air-conditioning devices during the hot seasons, diminishing the influence of outdoor temperature changes.
SO2 and NO2 are air pollutants commonly released by various industrial processes, especially fossil fuel combustion at power plants and emissions from motor vehicles. Gaseous pollutants can react with other compounds in the atmosphere to form small particles. Short-term exposure both to gases and nano-particles is linked with various effects on the cardiac and respiratory systems (26). Furthermore, during the last decade it has been demonstrated that air pollutants could affect cerebral vasculature and increase the risk of stroke (27). Our analysis of the short-term effect of air pollutants on ED headache visits demonstrated that the air concentration of pollutants, especially NO2, significantly increased the daily number of ED patients with a primary complaint of headache. This effect was found among women and among patients older than 40 years. The effect of air pollutants on ED headache visits was previously shown in several studies from the US, Canada and Chile (10,22,25). In these studies the concentration of several pollutants—NO2, SO2, ozone (O3) and CO—was positively associated with ED headache visits.
Although the pathophysiology of the effect of air pollutants on headache is not clear, several mechanisms were proposed to explain the influence of air pollution on cerebral vasculature, with an increase in systemic inflammation response being the most common together with an endothelial dysfunction and pro-coagulant effect of the pollutants (28). Inflammatory reaction is induced either by cytokines secreted from the lung tissue or by nano-particles penetrating the circulation and may affect the cerebrovascular endothelium or alter the properties of the blood-brain barrier (BBB) (29). All those mechanisms are known to be associated with the pathophysiology of migraine. Interestingly, the effect of air pollutants seems to be increased with older age. This effect was not previously reported, and its association with increased cerebrovascular risk is yet to be studied.
Our study has several limitations. We used outdoor air pollution concentrations measured at fixed point monitors, whereas people spend most of the time indoors. The obtained assessments, based on the fixed monitor stations might have resulted in a non-differential bias in exposure, which might have reduced the magnitude of the association at study toward the null hypothesis and produced wider CIs due to a mixture of classical and Berkson error (30). Secondly, the inclusion criterion was primary complaint rather than diagnosis, and patients were not categorized as primary (migraine or tension-type) or secondary headache. Finally, the data on headache onset time were not available and one can assume a certain unknown-to-us lag between the ED visit and headache onset.
Headache disorders are a common and major health problem significantly impairing patients’ quality of life. The impact of air pollution on headache may suggest a potentially modifiable headache trigger. It is possible that reducing exposure to air pollutants, on the personal or environmental level, may serve as a therapeutic modality for patients severely affected by primary headache disorders. Further study should be directed at exploring such interventional modalities.
Footnotes
Clinical implications
The impact of air pollution and weather on headache may suggest a potentially modifiable headache trigger.
In a large population-based study, we have found that increase in temperature and nitrogen dioxide was associated with increased risk of headache emergency department visits.
Reducing exposure to air pollutants may serve as a therapeutic modality for patients severely affected by primary headache disorders.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.