
Abstract
Background
Previous studies demonstrated that a severe neurovascular contact (NVC) causing displacement or atrophy of the trigeminal nerve is highly associated with classical trigeminal neuralgia (TN). There are no studies describing the association between the clinical characteristics of TN and severe NVC.
Methods
Clinical characteristics were prospectively collected from consecutive TN patients using semi-structured interviews in a cross-sectional study design. We evaluated 3.0 Tesla MRI blinded to the symptomatic side.
Results
We included 135 TN patients. Severe NVC was more prevalent in men (75%) compared to women (38%) (p < 0.001), and the odds in favor of severe NVC on the symptomatic side were 5.1 times higher in men compared to women (95% CI 2.3–10.9, p < 0.001). There was no difference between patients with and without severe NVC in age (≥60 years vs. <60) (OR 1.6 95% CI (0.8–3.4), p = 0.199) or duration of disease (p = 0.101).
Conclusions
Severe NVC was much more prevalent in men than in women, who may more often have other disease etiologies causing or contributing to TN. Severe NVC was not associated with age or with duration of disease.
Introduction
It has so far been widely accepted that neurovascular contact (NVC) plays a major role in the etiology of classical trigeminal neuralgia (TN) (1). Meanwhile, emerging evidence has indicated that it is specifically a “severe” neurovascular contact (NVC), i.e. displacement or atrophy of the trigeminal nerve, that is associated with TN (2–5). This is of major importance to TN etiology and pathophysiology, and possibly also for selection of patients for microvascular decompression (MVD). However, approximately half of TN patients do not have a severe NVC on the symptomatic side (2–6). Furthermore, a simple NVC, i.e. no displacement or atrophy of the trigeminal nerve, was a common finding on the asymptomatic side in TN (2,4,5). A NVC is also common in healthy individuals (7–88%) (4,7–10) and in cadavers (14–52%) (11–15), indicating that a simple NVC on the symptomatic side in TN could be a normal anatomical variant. Thus, in the group of patients without a severe NVC on the symptomatic side there are probably other etiological factors contributing to or solely responsible for TN.
Despite the debate over the importance of a severe NVC in TN there are, to the best of our knowledge, no previous prospective systematic studies describing the association between the clinical characteristics and neuroanatomical abnormalities at 3.0 Tesla magnetic resonance imaging (MRI) in a large cohort of consecutive well-characterized TN patients in a neurological setting (16). Most prior studies reporting the association between NVC and TN were based in neurosurgical settings and, as only a minority of TN patients are referred to surgery (17,18), neurosurgical TN populations are highly selected and not representative of the full spectrum of the disease.
In this prospective clinical study of consecutive TN patients, we aimed to investigate the possible differences in the clinical characteristics between patients with and without a severe NVC on the painful side. In a previous study we found that the female sex is associated with early onset of disease, concomitant persistent pain and sensory abnormalities at bedside examination (19). Another prior study linked concomitant persistent pain in TN to central sensitization (20), indicating that central changes are responsible for the concomitant persistent pain. Based on these findings we hypothesized that severe NVC was not as important in women as in men and was not associated with persistent concomitant pain or sensory abnormalities. Furthermore, based on prior assumptions (21,22), we hypothesized that severe NVC on the symptomatic side was associated with age and duration of disease.
Methods
We included consecutive patients seen at the Danish Headache Center (DHC) with unilateral TN from April 2012 to November 2013. As the study was explorative, we did not perform sample size calculations, and the number of patients was determined by the number of patients in the inclusion period. Exclusion criteria were bilateral TN, communication barriers, prior MVD or rhizotomia, symptomatic trigeminal neuralgia and contraindications to MRI. The method of the data collection, the MRI protocol and evaluation were previously reported in detail (5,19,23,24). It was determined by the Danish National Committee on Health Research Ethics (ID number H-1-2012-093) that the project did not need ethics approval or patients’ informed consent, as it is observational and based on routine clinical and laboratory workup.
Diagnosis was based on the diagnostic criteria of the second edition of the International Classification of Headache Disorders (ICHD-2) (25), and diagnosis was made by neurologists specializing in headache and facial pain. The diagnostic criteria exclude sensory abnormalities at bedside examination in TN. Meanwhile, psychophysical studies (26,27) and clinical experience (19,28) demonstrated that some TN patients have detectable sensory abnormalities. In case of sensory abnormalities at clinical routine neurological examination, we diagnosed TN if the other diagnostic criteria were fulfilled and a complete clinical history, neurological examination and a 3.0 Tesla MRI did not raise suspicion of other disease. We previously demonstrated that TN patients with sensory abnormalities at bedside examination have a higher prevalence of concomitant persistent pain (19) but are otherwise not different from TN patients without sensory abnormalities (23). On the basis of this evidence we recently suggested changes in the diagnostic criteria for TN in the final version of the third edition of ICHD allowing sensory abnormalities if secondary causes of TN have been ruled out by MRI, other appropriate investigations and patient history (24).
Clinical data were obtained by experienced neurologists and recorded on semi-structured interview forms. Several qualitative and quantitative variables were systematically collected using a semi-structured clinical interview (Supplementary material).
MRI protocol and definitions
All patients underwent an MRI scan within two months after the semi-structured interview was obtained. Imager was a 3.0 Tesla Phillips Achieva imager (Phillips Medical Systems, Best, Netherlands) equipped with a 32-channel head coil with multi-transmit parallel radiofrequency (RF) transmission. MRI protocol included sagittal T2-weighted turbo spin echo sequence covering the whole brain, axial thin section T2-weighted gradient and spin echo (GRASE) sequence encompassing the brainstem and the proximal and posterior fossa, three-dimensional (3D) time of flight MR angiography (s3DI MC HR) and 3D high spatial resolution heavily T2-weighted sequence (3D balanced fast field echo, BFFE). Multiplanar reconstructions were performed of the cisternal part of the NVC strongly parallel to the trigeminal nerve in the axial and sagittal plane and perpendicular to the NVC in the coronal plane.
MRI scans were evaluated by an experienced neuroradiologist (FW), who was blinded to symptom side. NVC was defined as contact between a blood vessel and the trigeminal nerve without visible cerebrospinal fluid between the two structures. If the evaluation was uncertain it was considered “no NVC.” Degree of contact was graded on a three-point scale as simple contact (Figure 1), displacement or atrophy (Figure 2). Displacement was defined as displacement or distortion of the trigeminal nerve at the site of an NVC. Atrophy was defined as reduced volume of the trigeminal nerve at the site of an NVC. “Severe NVC” was defined as NVC with displacement and/or atrophy. If the NVC was caused by one or more arteries or by one or more arteries and one or more veins, the NVC was defined as “NVC involving an artery.”
Flowchart of included patients. Axial (a), coronal (b) and sagittal (c) views of 3.0 Tesla magnetic resonance imaging of a simple neurovascular contact between the left trigeminal nerve (arrows) and the superior cerebellar artery (arrowheads). Patient suffers from left-sided classical trigeminal neuralgia.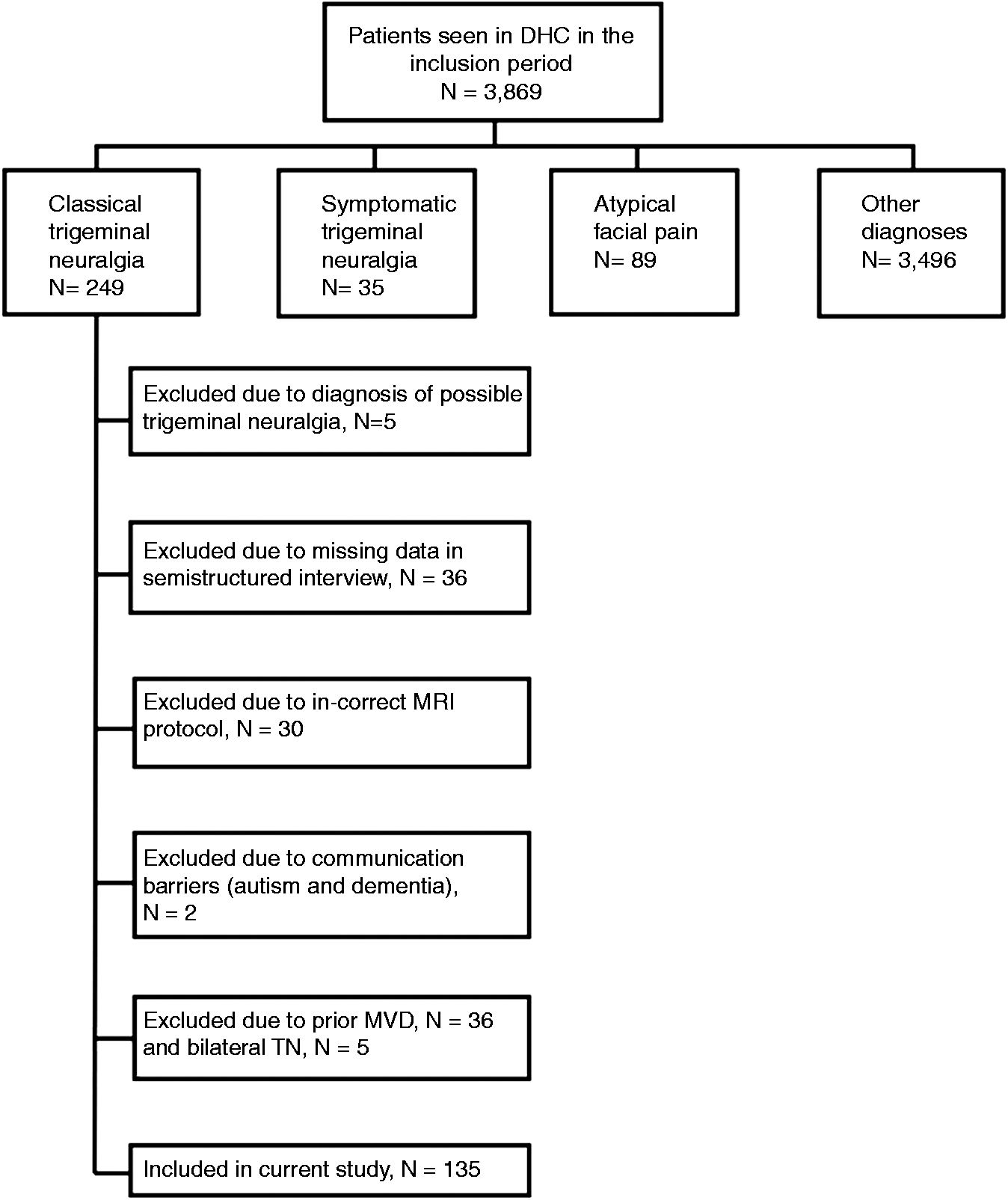

Statistical analyses
Continuous data are summarized by descriptive statistics, and the unpaired two-sample t-test was used for comparing independent groups. Categorical variables are presented with frequency distributions (N, %) and exact confidence limits. McNemar’s, Chi square and Fisher’s test were used as appropriate to assess associations of categorical variables. We defined a short duration of disease as ≤2 years and a long duration of disease as ≥10 years. Sensitivity was calculated as the true-positive (NVCs on the symptomatic side) rate divided by the true positive rate plus the false-negative (NVCs on the asymptomatic side) rate. Specificity was calculated as the true-negative rate divided by the true-negative rate plus the false-positive rate. P values for a significant difference between sensitivities and specificities of unpaired groups were analyzed by Chi square test and p values for significant difference between odds ratios (ORs) of paired data were evaluated by differences in the maximum likelihood estimates in conditional logistic regression.
We used multivariate logistic regression models with backward stepwise regression to test for an association between a subset of predefined variables and presence of severe NVC on the symptomatic side (vs. no severe NVC on the symptomatic side). Variables with significant association (p ≤ 0.05) were retained in the model and variables with no significant association were excluded sequentially. The independent variables were sex, age at interview (<60 vs. ≥60 years), concomitant persistent pain and sensory abnormalities at bedside examination.
If more than 5% of the data from the semi-structured interview form were missing, the patient was excluded from the analyses. P values are reported as two tailed with a level of significance of 5%. Analyses were carried out using SAS 9.3 (SAS Institute Inc, Cary, NC, USA).
Results
During the inclusion period, 249 patients diagnosed with TN had outpatient visits at DHC. Thirty-six patients were excluded for missing data and two patients were excluded because of communication problems. Five patients were excluded because of a diagnosis of “possible TN,” which could not be clarified at the end of the inclusion period. Thirty-six patients were excluded owing to prior MVD and five patients because of bilateral TN. The remaining 135 patients constitute the study population (Figure 3). The clinical characteristics of the total patient population were described in previous papers (19,23), and the prevalence of NVC and its associated characteristics on the symptomatic and asymptomatic side was reported in a recently published paper (5).
Axial (a), coronal (b) and sagittal (c) views of 3.0 Tesla magnetic resonance imaging of a displaced and atrophic left-sided trigeminal nerve (arrows) at the site of a loop from the superior cerebellar artery (arrowheads). Patient suffers from left-sided classical trigeminal neuralgia.
The evaluation of the NVC was uncertain on the symptomatic side in three cases and in five cases on the asymptomatic side. These cases were considered no NVC. As was reported in a prior paper (5) severe NVC on the symptomatic side was present in 71 (53%) of patients while 64 (47%) did not have severe NVC on the symptomatic side. Out of the 64 patients without a severe NVC on the symptomatic side, 49 (77%) had a simple NVC and 15 (23%) had no NVC.
Sex differences
Severe NVC on the symptomatic side was present in 40 (75%) of all men (N = 53) and in 31 (38%) of all women (N = 82), p < 0.001. Of the 15 patients without any NVC on the symptomatic side, 13 (87%) were women. The odds in favor of severe NVC on the symptomatic side vs. no severe NVC on the symptomatic side were 5.1 times higher in men compared to women (95% confidence interval (CI) 2.3–10.9, p < 0.001), and sex was the only characteristic associated with severe NVC in the multivariate logistic regression models. Stratified OR for the association between symptomatic side (vs. asymptomatic side) and severe NVC was 15.5 (3.7–64.8), p < 0.001 in men and OR 9.0 (2.7–29.7), p < 0.001 in women. The difference between the two ORs was not significant (p = 0.568). The sensitivity of a severe NVC on the symptomatic side was higher in men (75%) compared to women (38%) (p < 0.001), while the specificity of a severe NVC was higher in women (91%) compared to men (79%) (p = 0.041). In men, 47 (89%) had an NVC involving an artery on the symptomatic side as opposed to women, of whom 53 (65%) had an NVC involving an artery on the symptomatic side (p = 0.002).
Age and duration of disease
Patients with severe NVC were 5.2 years older (0.044) at time of interview and MRI, but the difference in age was not significant when controlled for sex in multivariate logistic regression (<60 vs. ≥60 years, OR = 1.7 (0.8–3.5), p = 0.199). Comparing patients with a short duration of disease (≤2 years) (n = 44, median duration =1 year, range (0–2)) to patients with a long duration of disease (≥10 years) (n = 35, median 14 years, range (10–66), there was trend toward a higher prevalence of severe NVC in patients with a short duration of disease (61%) vs. patients with a long duration of disease (43%), p = 0.101.
Other clinical characteristics
Demographics, periodicity and pain characteristics in classical trigeminal neuralgia patients with and without a severe neurovascular contact (NVC) on the symptomatic side.

VNRS: verbal numeric rating scale; CI: confidence interval. Values represent numbers of patients (%) unless otherwise indicated. N = 135. Test for significant difference: aChi-square, bunpaired t-test, cWilcoxon signed rank test. dSevere contact is defined as a neurovascular contact (NVC) causing either displacement or atrophy of the nerve. eNo severe contact is defined as either a simple NVC or no NVC. fBilateral cases were excluded from the study. gCurrent age is age at semi-structured interview. Magnetic resonance imaging (MRI) scans were performed within two months of the semi-structured interview in all patients. hRemission periods were defined as pain free periods lasting at least a month without medication or with very low dosage of medication defined as maximally carbamazepine 100 mg daily or oxcarbazepine 150 mg daily or corresponding doses of other drugs. iWe distinguished between two types of pain: paroxysmal pain lasting from a split second to two minutes and described by patients as superficial, intense, lancinating, stabbing, ice pick-like or electrical lightning. The other category of pain ranged from two minutes up to being constantly present and was described by patients as deep, toothache-like, aching, nagging, boring or dull. This type of pain was termed “concomitant persistent pain.”
Trigger factors, associated autonomic symptoms, sensory abnormalities, response to medication, comorbidities and family history.

CI: confidence interval. Values represent numbers of patients (%) unless otherwise indicated. N = 135. Test for significant difference: aChi-square, bunpaired t-test, cFisher’s exact test. dSevere contact is defined as a neurovascular contact causing either displacement or atrophy. eNo severe contact is defined as either a simple contact or no contact at all. fThe majority (88%) of patients who had ipsilateral autonomic symptoms associated with pain. Attacks had sporadic autonomic symptoms, i.e. autonomic symptoms were not pronounced at each attack. gThe clinical examination consisted of routine neurological examination for touch with cotton swab and pinprick with a pin in the three trigeminal branches. Sensory abnormalities in patients who had undergone prior surgical peripheral treatments for trigeminal neuralgia (TN) were not considered in the statistical analyses because surgical intervention could both cause complications of sensory disturbances and could possibly normalize sensory function. N = 125. hIt was regarded as a response if a patient had experienced pain relief after taking the drugs. If patients stopped using the drugs because of side effects or allergic reactions before therapeutic dosages and possible pain relief were reached, it was recorded as inconclusive due to intolerable side effects and counted as “no response” (one in each group). Patients who had not tried sodium channel blockers were excluded from the analysis. N = 113. Our data do not allow us to differentiate as to whether the response to sodium channel blockers was primarily related to a decrease in the short-lasting paroxysmal pain or also to a decrease in the concomitant persistent pain. iHypertension was defined as taking antihypertensive drugs specifically for hypertension. jFirst-degree relative with classical TN or facial pain.
Discussion
This is the first systematic study of the association between the clinical characteristics and neuroanatomical abnormalities in TN. The most important finding was that severe NVC is much more common in men than in women, indicating that women more often have other etiological factors contributing to TN. Secondly, we find that severe NVC is not associated with age, duration of disease, concomitant persistent pain or sensory abnormalities at bedside examination.
Differences between men and women in degree of NVC
We demonstrate that severe NVC is considerably more prevalent in men compared to women; thus the odds of severe NVC on the symptomatic side were five times higher in men compared to women. This major difference could not be explained by age differences. Findings indicate that in women there are probably more frequently other disease etiologies contributing to or solely responsible for TN. This is in line with the findings of Barker et al. (28), who documented that the female sex was a predictor of recurrence of pain after MVD. It is well established that differences between the sexes, when it comes both to clinical and experimental pain, are frequent (29). We recently reported that in almost all (98%) of severe NVCs there is an artery involved (5). Thus, an artery is generally the anatomical prerequisite for displacement or atrophy of the trigeminal nerve in TN patients. In accordance with these findings, we here demonstrate that men more frequently have an NVC involving an artery compared to women. Our findings may therefore also reflect a difference in the neuroanatomy in men and women.
Anatomical studies documented damage of the myelin at the site of an NVC in TN (30), and this is thought to be the anatomical correlate for the hyperexcitability, ectopic impulses and ephaptic transmission supposedly causing TN pain (1). Considering the average age at onset of 49.6 years in the group of patients without a severe NVC on the symptomatic side, consisting predominantly of women, one could speculate that hormonal fluctuations and changes related to perimenopause in some individuals may damage the ultrastructure of the myelin membrane in a similar way as the damage induced by a severe NVC. Indeed, animal studies linked estrogen receptor ligands and progesterone to neuroprotection, stimulation of endogenous myelination and myelin repair (31,32). As noted by Devor et al., it is also a possibility that the primary disorder is in or near the trigeminal ganglion in patients who do not have an NCV (1).
NVC is not a progressive phenomenon
Our findings indicate that severe NVC is not associated with age, nor with duration of disease—surprisingly there was a tendency to the opposite with respect to duration of disease. Neither was it associated with concomitant persistent pain nor with sensory abnormalities, which we in a prior study reported to be both prevalent and related (19). Our findings are in contradiction to the theory on the natural history of TN developed by Burchiel and Slavin, who stated that the trigeminal nerve gradually becomes transformed because of increasing mechanical compression leading to changes in the character of pain towards more and more persistent neuropathic pain, sensory impairment and poorer response to medication (21). On the contrary, our findings indicate that compression of the trigeminal nerve by a blood vessel is not generally a predominantly progressive phenomenon.
Moreover, our findings demonstrate that the primary etiology and pathophysiological mechanisms of concomitant persistent pain should be sought elsewhere than at the level of an NVC, which is in accordance with a recent study that reported facilitation of central nociceptive processing in TN patients with concomitant persistent pain indicative of central sensitization (20).
A recent retrospective study on the natural history of TN reported that pain did not become worse over time and only a few patients gradually developed resistance to medication (18). Adding to this picture, we found that the response to sodium channel blockers was high regardless of degree of NVC, which suggests a common pathophysiological pathway in TN across different disease etiologies.
Strengths and limitations
We prospectively collected detailed semi-structured interviews from a large cohort of TN patients in a neurological setting and systematically performed 3.0 Tesla MRI according to a protocol designed for the trigeminal nerve, and evaluation was performed blinded to symptomatic side. We used one only evaluator and did not include healthy controls. Thus, we cannot provide measures of interobserver agreement, nor can we correlate the findings to a healthy Danish population. The study population is from a single tertiary treatment center. Although we receive TN patients from the full spectrum of the disease, our results may not be representative for less-affected TN patients who can be treated in the primary or secondary sectors.
Conclusions
Severe NVC was common in men but not in women, indicating that factors other than NVC may be responsible for TN in a large proportion of women. Contrary to our primary hypothesis, age and duration of disease were not associated with severe NVC.
Clinical implications
Severe neurovascular contact with displacement or atrophy of the trigeminal nerve was more prevalent in men compared to women. Women may therefore more often have other etiological factors contributing to, or solely responsible for, classical trigeminal neuralgia. Severe neurovascular contact was not associated with duration of disease or with current age.
Footnotes
Funding
Part of the prize “Global Excellence in Health” awarded to DHC financed this study. This work was supported by the Lundbeck Foundation (grant number R118-A11531) and Trigeminus Foreningen. The funding sources had no role in the study.
Conflicts of interest
Lars Bendtsen was the principal investigator for Convergence Pharmaceuticals study 1014802/202 and has received research grants from Convergence Pharmaceuticals.