
Abstract
Background: Hemiplegic migraine (HM) is a rare variety of migraine with aura, characterized by motor deficits during the aura, often beginning in childhood. The hemiplegic attacks can be severe and prolonged but the prognosis is usually good. Data on neuroimaging, including diffusion-weighted imaging (DWI) and spectroscopy, during prolonged attacks of HM are quite limited, particularly in children.
Case: An eight-year-old female had a prolonged attack of sporadic HM characterized by right-sided hemiplegia, global aphasia, fever and impairment of consciousness. MRI nine hours after hemiplegia onset was negative, while the following MRI scans (days 4 and 11) documented a progressive increase in cortical swelling in the left hemisphere with mild hyperintensity on DWI and mild reduction of apparent diffusion coefficient values. Proton MRI spectroscopy (MRS) (day 15) showed a decrease in the N-acetylaspartate/creatine ratio in the left hemisphere. 99mTc-ECD single-photon emission tomography (SPET) (day 27) showed marked left hemispheric hypoperfusion. The patient recovered completely after 40 days and neuroimaging follow-up (MRI and SPET) after six months was normal. The patient carried a missense mutation of the ATP1A2 gene.
Conclusion: Multimodal neuroimaging (MRI, DWI, MRS, SPET) in a prolonged HM attack supports evidence for a primary neuronal dysfunction.
Introduction
Hemiplegic migraine (HM) is a rare variety of migraine with aura, but unlike the latter it is characterized by motor deficits during the aura, which can last up to 24 hours and are completely reversible (1). HM episodes can be very severe, with confusion, coma, fever, seizures and prolonged hemiplegic attacks lasting up to several weeks having been reported (1). Data on neuroimaging during prolonged attacks of HM are quite limited, particularly in children (2–5). Brain MRI in the acute phase may show signal hyperintensity in T2-dependent sequences (2,3,6–11) and on diffusion-weighted imaging (DWI) with normal or reduced apparent diffusion coefficient (ADC) values (2,3,6,8–12). Data on MRI spectroscopy (MRS) (9) and cerebral single-photon emission tomography (SPET) (2,4,6,7,11) during prolonged HM attacks are quite scarce.
Case report
An eight-year-old female was referred to the hospital with acute developing right-sided hemiplegia, global aphasia, deterioration of vigilance, headache and fever. The weakness and neurological deficits developed gradually over 30 minutes. A few hours before, the child had complained of moderate headache responsive to paracetamol.
Since the child was two years of age, five attacks of transient hemiplegia (lasting less than 20 minutes), mainly on the right side, had occurred about once a year, sometimes associated with aphasia and right-central facial nerve palsy, followed by headache for a few hours. The last attack had occurred at the age of six years and six months.
Brain CT scans and MRI at the age of three years and six months, and electroencephalographam (EEG) at the age of four years were normal. At the age of 11 months, the child had two episodes of febrile convulsions. In the paternal line, a second cousin and a great-uncle had both suffered from migraine without aura and a second cousin had suffered from migraine with visual aura; the other family members had no other relevant history.
On admission the patient was lethargic (Glasgow Coma Scale: E2V2M5), febrile (38.9°C), and aphasic, with right-sided hemiplegia.
Brain CT scan (one hour after hemiplegia onset) and MRI including DWI (nine hours after hemiplegia onset) were normal. Cerebrospinal fluid (CSF) examination (physical and chemical examination, microscopy, culture, viral polymerase chain reaction assay), indices of inflammation, plasma cultures and serology, performed few hours after the onset, were unremarkable. Immunological investigations (antinuclear, anti-extractable nuclear antigen, anti-neutrophil cytoplasmic, lupus anticoagulant, anticardiolipin and anti-native DNA antibodies, rheumatoid factor, C3, C4) and coagulation tests (prothrombin time, partial thromboplastin time, international normalized ratio, protein C, protein S, plasminogen activator, beta2-glicoprotein I antibodies, factor V Leiden) were negative. A heterozygote MTHFR C677T mutation was detected. Intravenous dexamethasone was administered, with mild benefit.
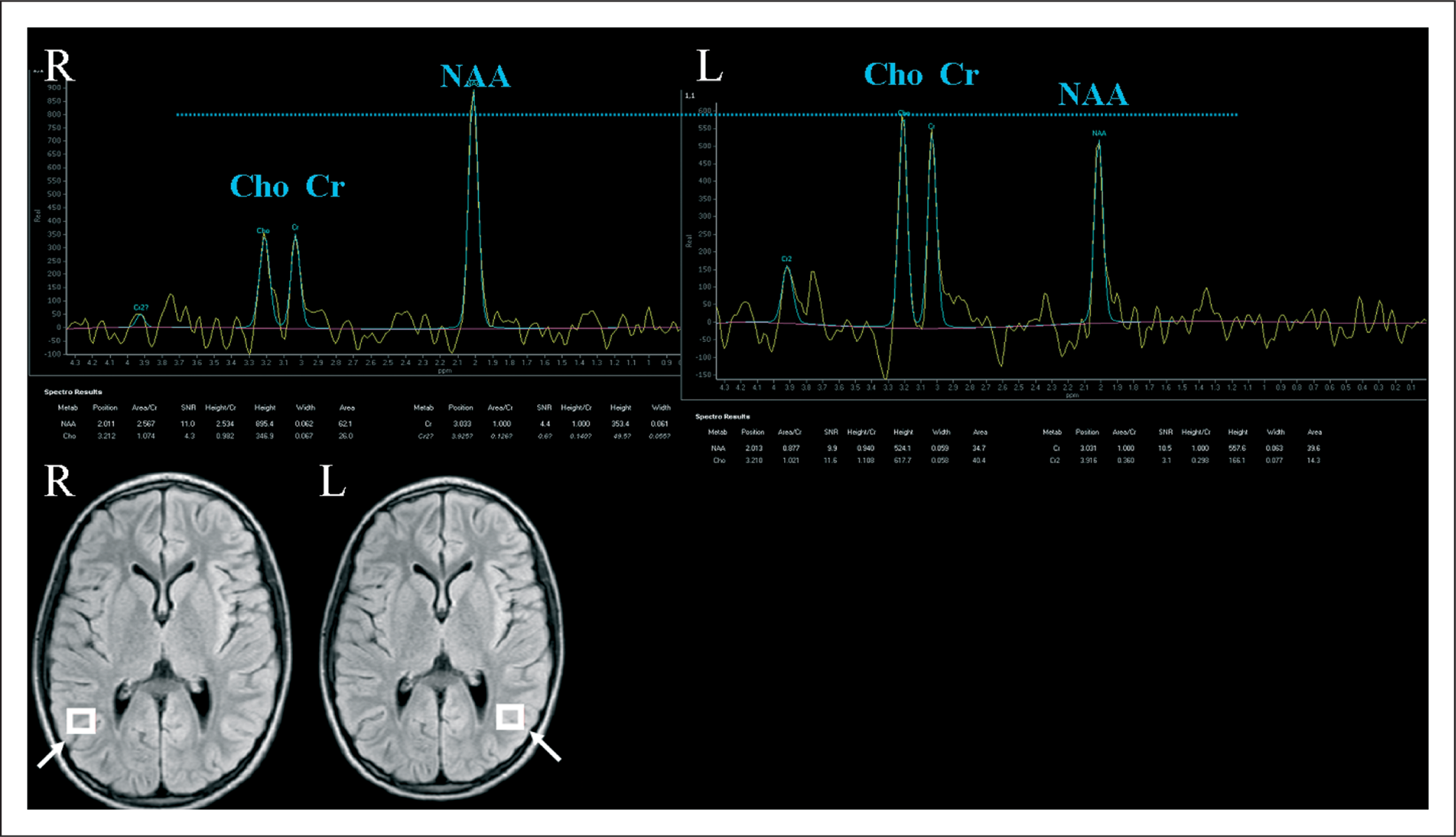
An EEG (day 4) documented a marked hemispheric asymmetry with high-amplitude delta waves in the left hemisphere, not modified by an intravenous diazepam bolus. A second MRI (day 4), showed on fluid attenuation inversion recovery (FLAIR) images a mild swelling of cortical sulci in the left occipital regions with slight hyperintensity in the DWI (Figure 1A,B) with normal ADC values, and no enhancement on postcontrast T1-weighted images. MR angiography (MRA) showed a mild arterial dilation of left intracranial vessels. Transcranial doppler and echocardiogram were normal. During the first three days, the patient presented with drowsiness, severe throbbing headache with nausea, phonophobia, photophobia, complete right hemiplegia with right-central facial nerve palsy, global aphasia, sphincter incontinence and high fever unresponsive to antipyretics; then the clinical picture gradually improved. Fever stopped after one week from the onset. A third brain MRI (day 11) showed on FLAIR images an extensive swelling of the left cortical hemisphere, with slight hyperintensity in the DWI sequences (Figure 1C,D) and mild reduction of ADC values (881 s/mm2; controlateral side 960 s/mm2). A fourth MRI (day 15) disclosed a significant reduction of the left cortical hemisphere swelling (Figure 1E,F). On proton MRS (TE 299 ms) performed 15 days after the onset of hemiplegia, there was a mild decrease of the N-acetylaspartate/creatine (NAA/Cr) ratio on the left occipital cortex compared to the controlateral one (respectively 0.90 and 2.53) (Figure 2). MRI were done using a 1.5-T magnet (Philips Achieva 1.5 Tesla) without sedation.
MRI. (A) Axial FLAIR and (B) DWI (day 4) showing mild cortical swelling of the left occipital region; after one week (day 11) the same sequences (C, D) documented an extensive cortical swelling in the left hemisphere, which significantly reduced on day 15 (E, F). FLAIR = fluid attenuation inversion recovery; DWI = diffusion-weighted imaging. Proton MRS. Proton MRS (PRESS sequence TR 200 TE 299) (day 15) in the region of interest on the left side shows reduced N-acetylaspartate/creatine ratio (NAA/Cr) compared to the right side (left: 0.90; right: 2.53). The findings are consistent with reduced neuronal acitivity. NAA= N-acetylaspartate. Cho = choline. Cr = creatine. MRS = MRI spectroscopy.
99mTc-ethylcysteinate dimmer (99mTc-ECD) brain perfusion SPET (day 27) showed a marked left hemispheric hypoperfusion and a slight hypoperfusion of the right cerebellar cortex (Figure 3A,B). Semiquantitative evaluation of the uptake of the radiopharmaceutical at the left hemisphere was 45.15%, while on the right side was 54.85%. 99mTc-ECD (Neurolite) was chosen because of the higher contrast (gray-to-white matter ratio) as compared to 99mTc–D, L-hexamethylpropylene amine oxime (99mTc-HMPAO) and because it clears faster from the body, resulting in less exposure of the child.
99mTc-ECD SPET. (A) 99mTc-ECD brain perfusion SPET (day 27) showing a marked left hemispheric hypoperfusion (especially at the parietal cortex and temporal lobe) and (B) a slight hypoperfusion of the right cerebellar cortex. (C) 99mTc-ECD SPET after six months showing normal cerebral and (D) cerebellar perfusion. SPET = single-photon emission tomography.
The hemiplegia significantly improved after two weeks and completely resolved after one month, while the global aphasia resolved more gradually, after 40 days from onset. Follow-up MRI (not shown) and 99mTc-ECD SPET (Figure 3C,D) after six months were normal; the semiquantitative uptake was almost completely normal (left hemisphere: 49.84%; right hemisphere: 50.16%).
The neuroimaging study protocol was approved by our Institutional Review Board. The molecular analysis of the alpha-2 isoform of sodium-potassium-ATPase (ATP1A2) gene disclosed a missense mutation c.1091C>T (p.Thr364Met) in heterozigosis on exon 9, not found neither in both parents or in 100 Caucasian controls; this mutation has not been previously reported.
Discussion
All clinical, radiological and genetic findings in our case were fully consistent with the diagnosis of sporadic hemiplegic migraine (SHM), notably the very early onset of HM attacks, the recurrence of typical HM attacks with motor aura lasting less than 24 hours, the association with benign febrile convulsions that preceded the first HM attack as well as the severe and prolonged hemiplegia with impairment of consciousness.
Multimodal investigations were performed in order to rule out other causes for the very severe attack that mimics potential life-threatening conditions such as meningo-encephalitis, stroke, seizures with prolonged Todd's palsy, migrainous infarction, MELAS syndrome and transient headache with neurological deficits and CSF lymphocytosis.
In the current International Headache Society criteria for HM (13), the duration of each aura symptom is limited to 24 hours. Considering this criterion, our case should be considered as atypical because hemiplegia was rather prolonged; however, hemiplegic attacks lasting for several weeks have been reported in other HM cases (6,7,9), even in children (2,5). Rarely, residual permanent neurological deficits, such as aphasia and ideomotor apraxia, may persist (7). In our case the focal neurological deficits lasted about six weeks and were completely reversible, confirming that long duration of aura symptoms is not associated with permanent focal neurological deficits.
The features of headache in our patient met the criteria for migraine without aura, and there was not prior history of migraine, but headache was always associated with recurrent hemiplegia attacks.
It has been recently shown that de novo mutations in the two main familial hemiplegic migraine (FHM) genes, ATP1A2 and CACNA1A, were frequent (76%) in early-onset SHM (before 16 years), in particular when SHM was associated with additional neurological features such as ataxia (for CACNA1A mutations), epilepsy or intellectual deficit (14).
A de novo mutation in ATP1A2 gene was found in our patient.
The neuroradiological findings previously reported in prolonged attacks of HM include:
diffuse cortical swelling and edema contralateral to hemiparesis on T2-weighted and FLAIR images (2,5,7–9,12); DWI sequences may show hyperintensity with normal (3,6) or reduced (4) ADC values, or may be normal (2,6,10–12); mild enhancement of the controlateral cortex and/or of the meninges and pial vessels (4,9,10,12) or no enhancement (3,6) on T1-weighted images after gadolinium.
The affected regions do not correspond to a single vascular territory, there is no cerebral ischemia, and the MRI abnormalities are usually resolved after 4–12 weeks (2,3,6–11).
In our case, the first MRI was negative while the neuroradiological follow-up documented a progressive increase of the cortical swelling with mild hyperintensity on DWI and mild reduction of ADC values in the subacute phase (day 11), suggesting intracellular edema. The delayed DWI signal abnormalities suggest that the cortical edema is not of ischemic origin and is probably caused by a prolonged neuronal depolarization. The mild dilation of intracranial vessels contralateral to hemiparesis, observed on MRA, could be a compensatory phenomenon, as reported in other cases (2,3,10,11).
In Figure 4 the clinical course and neuroradiological findings have been compared, showing a clear temporal dissociation.
Clinical course and neuroradiological findings. Comparison between the clinical course and neuroradiological findings in our case, showing a clear temporal dissociation. MRI was normal at the onset and then progressively worsened (day 11). 99mTc-ECD SPET (day 27), performed when the hemiplegia was almost completely resolved, showed a marked cerebral hypoperfusion of the left hemipshere. SPET = single-photon emission tomography.
Proton MRS (day 15), similarly to another adult case (9), showed a reduction of NAA, consistent with reduced neuronal metabolic activity and neuronal loss; it has been hypothesized that, in these cases, cell death could be due to a mechanism of apoptosis (9) or excitotoxicity (7).
99mTc-ECD brain perfusion SPET (day 27), performed when the hemiplegia was almost completely resolved but aphasia persisted, showed a marked unilateral cerebral hypoperfusion. This finding, associated with a normal cerebral blood flow, as documented by transcranial doppler and MRA, might also suggest a primary neuronal dysfunction with a reduced uptake of the radiopharmaceutical by “stunned neuronal cells”. SPET was performed with 99mTc-ECD, which estimates the regional cerebral blood flow (rCBF) and seems less affected by “luxury perfusion phenomena” as compared to 99mTc-HMPAO, showing metabolically active cerebral tissue rather then only perfusion. In the other cases reported in the literature, using 99mTc-HMPAO, the SPET showed increased tracer uptake on day 2 (6,11), which persisted on days 4 and 23 (11), or diffused hypoperfusion of the affected hemisphere on hospital day 2 (4). The only other case, to our knowledge, using 99mTc-ECD revealed hypoperfusion three months after (7) and two years after the onset of symptoms suggesting possible irreversible damage of cerebral tissue. In our patient SPET was normal after six months. Therefore, prolonged HM attacks could lead to reversible or irreversible abnormalities that can be visualized using 99mTC-ECD. In our case SPET also documented a slight crossed cerebellar diaschisis, as previously reported in two cases with HM (4,11). Crossed cerebellar diaschisis is a phenomenon attributable to a functional deafferentation of normal input to a region not directly involved by the pathology.
In Figure 5 the neuroimaging findings have been related to the possible underlying pathogenic mechanisms.
Pathogenesis. The neuroimaging findings in our case have been related to the possible underlying pathogenic mechanisms. *Atrophy has been reported in other cases (5) but not documented by MRI at six months from the onset in our case.
Our case contributes to the relevant literature with multimodal neuroimaging documentation and a longitudinal neuroradiological follow-up of a prolonged HM attack in a child. Cerebral MRI showed, in the acute and subacute phases, progressive changes of signal alterations in the hemisphere affected, temporally uncorrelated to the clinical course. MRS findings argue for a neuronal loss (decreased NAA) without cerebral ischemia. 99mTc-ECD SPET documents a reversible impairment of the neuronal function, which lasted longer than the clinical symptoms and MRI abnormalities.
A limitation of our study is that MRS and SPET were not done early in the course of illness. Multimodal neuroimaging is experimental and expensive, and therefore cannot be justified in routine practice and should be done in conjunction with an approved Institutional Review Board. Brain MRI (including DWI) and MRA have an essential role in the differential diagnosis of acute hemiplegia; however, neuroimaging data in this case did not obviate the need for extensive testing of potential serious causes other than HM.
Multimodal neuroimaging (MRI, DWI, MRS and SPET) provides a significant contribution to understanding the pathogenesis of prolonged HM attacks, supporting evidence for a primary neuronal dysfunction.
Footnotes
Acknowledgements
Thanks are expressed to Dr. Maria Teresa Bassi for performing the molecular analysis of ATP1A2 gene.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest statement
The authors declare that there are no conflicts of interest.