
Abstract
Objective
Whether migraine is associated with urinary calculi is an unresolved issue, although topiramate, a migraine-preventive agent, is known to contribute to this complication. This study investigates the association between migraine and the risk of urinary calculi.
Methods
We identified a total of 147,399 patients aged ≥18 years with migraine diagnoses recorded in the Taiwan National Health Insurance Research Database between 2005 and 2009. Each patient was randomly matched with one individual without headache using propensity scores. All participants were followed from the date of enrollment until urinary calculi development, death, or the end of 2010.
Results
The risk of urinary calculi was greater in the migraine than the control cohort (adjusted hazard ratio (aHR), 1.58; 95% confidence interval (CI), 1.52–1.63; p < 0.001, irrespective of the influence of topiramate. The risk was higher in younger and female patients. The magnitude of the risk was proportional to the annual frequency of clinic visits for headache (≥6 vs. <3, aHR = 1.11; 95% CI, 1.04–1.17; p = 0.002), but did not differ between migraine patients with and without aura.
Conclusions
Our study showed migraine was associated with an increased risk of urinary calculi, independent of topiramate use. A higher frequency of clinic visits was associated with a greater risk.
Keywords
Introduction
Migraine is a common and disabling neurovascular disease with female predominance and a peak prevalence at 25–55 years of age. The overall one-year prevalence is about 8%–15% in Western countries (1–4) and 9.7% in Taiwan (5). Population-based studies have verified the associations of several conditions, such as stroke (6), depression (7), anxiety disorders (8), epilepsy (9) and sensorineural hearing loss (10), with migraine. Intriguingly, in a cross-sectional population-based twin study, Bernecker et al. (11) found that migraine was comorbid with urinary calculi. Clinically, concern about the association between migraine and urinary calculi has increased, as the latter have been reported as a complication of topiramate, a frequently prescribed anti-epileptic and migraine-preventive agent (12). One United States study estimates that about 3%–13% of American migraine sufferers are on preventive therapy, while an estimated 38% actually need a preventive agent (13).
No large-scale longitudinal study to date has investigated the association between topiramate use and urinary calculi, and whether this complication is a result of migraine per se or the use of this medication remains to be elucidated. To address this issue, we conducted a nationwide, large-scale, population-based study using the Taiwan National Health Insurance Research Database (NHIRD) to determine whether migraine or concurrent medication use is associated with the formation of urinary calculi.
Methods
Data source
Taiwan’s National Health Insurance (NHI) program, launched in 1995, covers more than 99% of the population, which is currently 23 million. This mandatory universal program offers comprehensive medical coverage, including outpatient, inpatient, emergency, dental, and traditional Chinese medicine services and prescription drugs, to all Taiwanese residents. NHI databases managed and publicly released by the National Health Research Institute of Taiwan were used in this study. The multiple NHI databases (enrollment files, claims data, and drug prescription registry) provide comprehensive utilization and enrollment information for all covered patients. Diseases are coded according to the 2001 International Classification of Diseases, ninth revision, Clinical Modification (ICD-9-CM). The accuracy of diagnoses in the NHIRD has been validated for several diseases (14–16), and this database has been the primary source for several published studies (17,18). All information that would potentially expose the identities of individual patients has been encrypted. The confidentiality of the data abides by the regulations of the Bureau of National Health Insurance and the National Health Research Institute. This study was approved by the institutional review board of Taipei Veterans General Hospital.
Study design
This nationwide population-based, observational, retrospective cohort study was performed in Taiwan to determine the association between urinary calculi and migraine. Two cohorts—a migraine cohort and a matched control cohort—were enrolled in the study (online Supplementary Figure S1). The migraine cohort comprised all patients who visited a neurologist with the diagnosis of migraine (ICD-9-CM code 346.x) between January 2005 and December 2009, from a population of approximately 23 million. According to the ICD-9-CM, three subgroups of migraine were identified: migraine with aura (MA; codes 346.00–346.01), migraine without aura (MO; codes 346.10–346.11), and migraine unspecified (codes 346.90–346.91). Each patient with migraine entered the cohort on the day of the first clinical visit with the diagnosis codes of migraine. Those aged <18 years, with antecedent urinary calculi or followed up for ≤30 days after migraine diagnosis were excluded. On the other hand, matched control individuals were extracted from a dataset of 1 million beneficiaries randomly sampled from the original NHIRD. We randomly assigned an index date of the control participant corresponding to the diagnosis date of the migraine patient initially. Those with diagnoses of migraine (ICD-9-CM code 346.x), tension-type headache (code 307.81), or headache (code 784.0) prior to the index date, those aged <18 years, with antecedent urinary calculi, and those followed up for ≤30 days after the index date were excluded as the control group. For each cohort, the remaining participants began their follow-up on day 31, which was defined as the index date in this study, after exclusion of those who were followed up for ≤30 days.
Propensity score matching
To reduce selection bias, we performed 1:1 case-control propensity score matching. For each patient in the migraine cohort, we identified one control patient with a matched propensity score for the likelihood of migraine diagnosis, calculated from baseline covariates using multivariate logistic regression. Individuals in the migraine cohort who could not be matched were excluded from the study.
Outcomes
The primary outcome was the development of urinary calculi during the follow-up period. Urinary calculi occurrence was defined by the first hospitalization or ambulatory visit with a primary diagnosis (ICD-9-CM code 592.x or 594.x), surgery for urinary calculi, or extracorporeal shock wave lithotripsy (ESWL). Both cohorts were followed from January 1, 2005 until December 31, 2010, death, or the occurrence of the primary outcome. The follow-up of the control cohort was also terminated if migraine (ICD-9-CM code 346.x) developed.
Baseline characteristics
Baseline demographic characteristics, including age, sex, medical care utilization (number of ambulatory visits in the past year), income, and urbanization, were extracted and recorded. Charlson Comorbidity Index (CCI) scores were used to determine overall systemic health (19). Each increase in the CCI score is associated with a stepwise increase in cumulative mortality, such that a score of 0 indicates a 10-year survival rate of 99% and a score of 5 denotes a 10-year survival rate of 34% (19). Data on systemic diseases not included in the CCI, including atrial fibrillation, valvular heart disease, hypertension, asthma, dyslipidemia and drug abuse, were also collected. The look-back period for all baseline covariates and history of urinary calculi was at least one year before index date.
Data on concurrent medications potentially associated with physical conditions or calcium metabolism were extracted and classified using the World Health Organization Anatomical Therapeutic Chemical system. Medications were categorized as antiplatelet agents, warfarin, angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, beta blockers, calcium-channel blockers, diuretics, nitrate, statin, dipyridamole, steroids, estrogen, progesterone, nonsteroidal anti-inflammatory drugs, proton-pump inhibitors and antihyperglycemic drugs.
Statistical analysis
The cohorts’ baseline characteristics were analyzed using descriptive statistics and compared using Pearson χ2 tests for categorical variables and independent t-tests for parametric continuous variables. Propensity scores for the likelihood of migraine diagnosis were calculated using multivariate logistic regression analyses, conditional on baseline covariates. The incidence rates of urinary calculi in the two groups were calculated by Poisson distribution, and the relative risks of this complication were compared using hazard ratios (HRs) in Cox regression models. Cox regression models were also used to examine the influences of age, sex, CCI score, and migraine subtype on the incidence of urinary calculi after the diagnosis of migraine. Interactions were examined for these subgroups using the likelihood ratio test.
The Microsoft SQL Server 2008 R2 (Microsoft Corporation, Redmond, WA, USA) was used for data linkage, processing, and sampling. Propensity scores were calculated using SAS software (version 9.2; SAS Institute Inc, Cary, NC, USA). All other statistical analyses were conducted using STATA statistical software (version 12.0; StataCorp, TX, USA).
Results
Characteristics of the study population
Demographic and clinical characteristics of patients.

Including aspirin, clopidogrel, ticlopidine, and cilostazol.
SD: standard deviation; ACE: angiotensin-converting-enzyme; ARB: angiotensin II receptor blocker.
Incidence rates and risks of urinary calculi
Incidence and risk of urinary calculi in patients with migraine and matched participants.
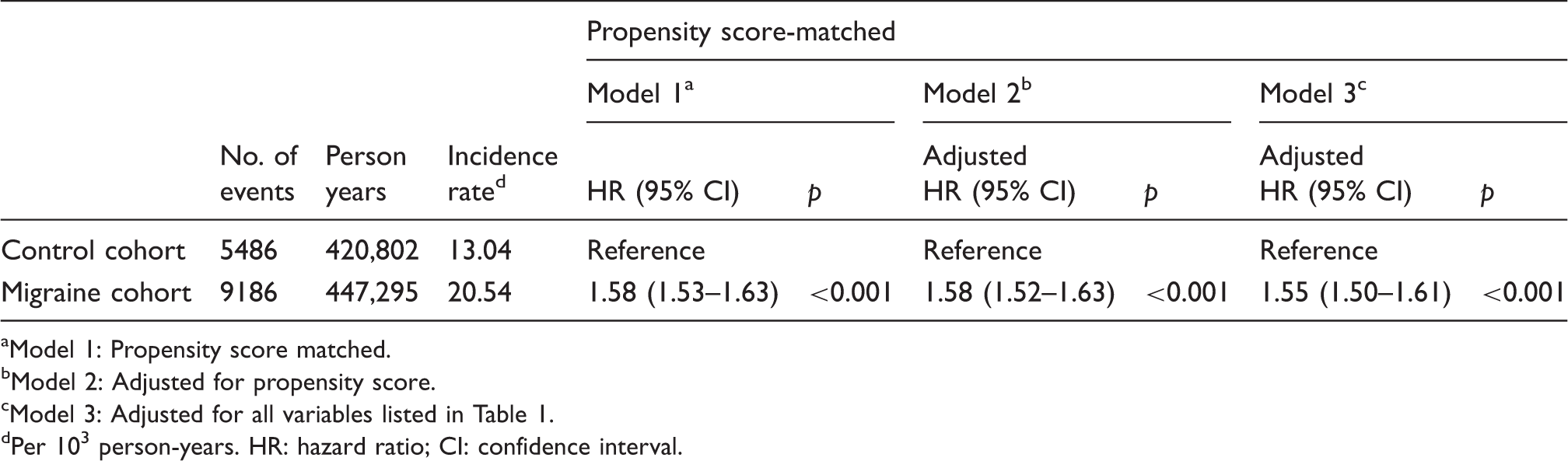
Model 1: Propensity score matched.
bModel 2: Adjusted for propensity score.
cModel 3: Adjusted for all variables listed in Table 1.
dPer 103 person-years. HR: hazard ratio; CI: confidence interval.
Subgroup analyses of urinary calculi risk by age, sex, CCI score, and topiramate use
Subgroup analyses of the risk of urinary calculi in patients with migraine and matched subjects.

Adjusted for propensity score.
pinteraction <0.001;
pinteraction = 0.001;
pinteraction = 0.565;
pinteraction = 0.007.
In subgroup analyses of topiramate initiator, patients with migraine were compared with matched controls.
Defined as using topiramate within 30 days after enrollment and without using topiramate within one year before enrollment. CI, confidence interval.
On the other hand, we defined topiramate initiator as those who used topiramate within 30 days after enrollment but did not receive any topiramate within one year before enrollment. A significant interaction between topiramate initiator and migraine was observed (pinteraction = 0.007), and migraine was associated with an increased risk of a urinary calculi event in both topiramate initiator and non-initiator groups, with an aHR of 1.96 (95% CI, 1.66–2.31; p < 0.001) and 1.56 (95% CI, 1.51–1.61; p < 0.001), respectively (Table 3).
Risk factors for urinary calculi among patients with migraine
The risks of urinary calculi were similar in patients with MO and MA (aHR 0.99; 95% CI, 0.92–1.06; p = 0.695). When we divided patients with migraine into two groups according to topiramate initiator or not, the risk of urinary calculi was significantly greater in topiramate initiators than non-initiators, with an aHR of 1.12 (95% CI 1.01–1.23, p < 0.026).
After excluding those with topiramate use within one year before enrollment, migraine patients were stratified into three subgroups according to the total days of using topiramate within the first year after migraine diagnoses. The risk of urinary calculi was significantly greater in patients receiving ≥30 days topiramate treatment within the first year (aHR 2.19, 95% CI 1.21–3.96, p = 0.006) but not in those receiving topiramate for one to 29 days (aHR 1.09, 95% CI 0.98–1.20, p = 0.112) when compared to the nonusers.
Risk of urinary calculi in patients with migraine.

HR: hazard ratio; CI: confidence interval.
Adjusted for all confounders in Table 1.
Defined as using topiramate within 30 days after enrollment and without using topiramate within one year before enrollment.
Adjusted for all confounders in Table 1 plus subtype of migraine, i.e. migraine with or without aura.
The initiating topiramate use was calculated as the number of days of topiramate used within the first year after enrollment in subjects without using topiramate within one year before enrollment. Patients with a follow-up period less than 1 year were excluded. The index date was redefined as 366 days after diagnosis of migraine to avoid immortal time bias.
Adjusted for all confounders in Table 1 plus topiramate use and annual frequency of ambulatory visits for headache within first year after diagnosis of migraine.
fDefined as the frequency of ambulatory visits within the first year after enrollment in subjects without using topiramate within one year before enrollment. Patients with a follow-up period less than 1 year were excluded. The index date was redefined as 366 days after diagnosis of migraine to avoid immortal time bias.
Sensitivity analyses
Sensitivity analysis for the risk of urinary calculi in the migraine and control cohorts.

Per 103 person years.
Adjusted for propensity score. CI: confidence interval; ESWL: extracorporeal shock wave lithotripsy.
Discussion
Our study demonstrated an association between migraine per se and urinary calculi, independent of topiramate usage. Patients with migraine were at increased risk of developing urinary calculi (aHR 1.55) compared with matched controls during the six-year study period. In subgroup analyses, this risk was greater in women and younger patients, in patients receiving topiramate ≥30 days within the first year after diagnosis of migraine, and those making more ambulatory visits for headache, especially those making ≥6 visits within the first year (aHR 1.11 vs. <3 visits).
Few published studies have examined the association between migraine and urinary calculi. Bernecker et al. (11) first reported that urinary calculi were more common in patients with migraine in a cross-sectional study, but they did not explore the effects of medications, especially topiramate. Our longitudinal research was the first to establish the increased risk of urinary calculi development in patients with migraine. Most previous studies have attributed urinary calculi formation in patients with migraine to the effects of topiramate treatment. In a case series of seven patients with migraine, topiramate treatment was associated with an increased lithogenic risk in a dose-dependent manner (20). The lithogenic effects of topiramate on hypocitraturia may persist for long periods of time after treatment and predispose patients to urinary calculi formation. This dose-dependent lithogenic effect was demonstrated in the present study in an analysis of the migraine cohort stratified by accumulated days of topiramate treatment; the risk of urinary calculi development was significantly greater in patients receiving topiramate treatment ≥30 days within the first year after migraine diagnosis than in those receiving <30 days. However, the risk of urinary calculi was also significantly higher in patients who did not receive topiramate treatment initially, indicating that the association of migraine with lithogenic risk was independent of topiramate usage.
In the general population, men are much more likely than women to develop urinary calculi (21). However, urinary calculi were more prevalent in women with migraine in the current study, similar to the findings of Bernecker et al. (11). Moreover, the risk did not differ between MA and MO. The mechanisms underlying the link between migraine and urinary calculi are largely unknown. We propose two possible explanations. The first potential candidate is calcitonin gene-related peptide (CGRP), one of the most abundant neuropeptides in the nervous tissue, which plays a crucial role in migraine generation via the cephalic vasodilation effect and pain transmission (22). CGRP also has a potent inhibitory effect on the motility of the human ureter in vitro, which may promote ureteral obstruction due to urine stasis and urinary calculi (23). The concentration-dependent inhibitory effects of CGRP on the ureteral smooth muscle were confirmed in guinea-pig models (24,25). Elevated plasma CGRP levels in cranial (26) and systematic circulation were found in patients with migraine, regardless of the presence or aura and outside of attacks (26,27). Of note, CGRP levels were also higher in female than in male patients with migraine (28,29). Moreover, Cernuda-Morollón et al. (30) reported higher CGRP levels in patients with chronic migraine (≥15 headache days per month) than in those with episodic migraine (<15 headache days per month), which might explain our finding that a higher frequency of ambulatory visits for headache within the first year, especially ≥6 visits, was associated with a greater risk of developing urinary calculi. The second possible explanation for lithogenic risk involves increased oxidative stress and decreased antioxidant capacity. Bernecker et al. (11,31) assessed biomarkers such as nitrite and found increased oxidative stress in subjects with migraine. On the other hand, results of a recent study of 17,695 participants in the National Health and Nutrition Examination Survey of the United States showed significantly lower serum antioxidant levels in patients with histories of urinary calculi (32). Decreased antioxidant capacity and increased oxidative stress were found to promote urine crystallization and subsequent development of urinary calculi in animal (33,34) and in vivo studies (35).
The major strengths of our study are the large sample size and nationwide population-based design, which relies on a comprehensive medical utilization claim database including all patients diagnosed with migraine during 2005–2009. To accurately interpret the influence of migraine on the incidence of urinary calculi, we used a propensity score-matched case-control method to minimize possible confounding factors and provide convincing power for appropriate statistical analyses. Neurologists made all diagnoses of migraine included in the current study using ICD-9 codes. Moreover, we validated urinary calculi diagnoses using interventions, which showed consistent results (8).
Several limitations of this study should be addressed. First, diagnoses of migraine in our study were derived from administrative claims data and may not be as accurate as those made using a standardized protocol. However, to validate the administrative claims identification of diagnoses, we included only those made by neurologists. The accuracy of migraine diagnoses made by neurologists in Taiwan using the International Classification of Headache Disorders, second edition criteria, exceeded 90% (36). Second, patients with migraine who did not seek medical assistance or sought alternative treatment may have been misclassified into the matched control cohort. Thus, the risk of developing urinary calculi in patients with migraine was likely underestimated in our study. Third, deviations in urinary calculi coding in the NHI claims data are also inevitable. However, our study provided consistent evidence of the increased risk of urinary calculi in patients with migraine after validation of the former diagnosis using intervention procedures. Fourth, information on several potential confounders of urinary calculi development, such as obesity, excessive oxalate intake, inadequate water intake, and calcium supplementation, was not available in our database. Fifth, previous studies have found that the incidence and prevalence of urinary calculi are higher in Taiwan than in Western countries (37–40); thus, our results should be interpreted cautiously and with recognition of ethnic differences and the influence of different clinical settings. Sixth, the current study identified only an association between migraine and urinary calculi; the causal relationship between these disorders warrants further investigations. Finally, the migraine cohort included only individuals with active migraine who sought medical attention.
Migraine and urinary calculi are common disorders that cause functional disability and loss of work time. In the current study, migraine was viewed as a previously unidentified risk factor for urinary calculi. Clinicians should pay more attention to urinary tract symptoms in patients with frequent migraine attacks, such as those with chronic migraine, to aid the early detection of potential urinary calculi. Patients with migraine, especially those with frequent headache and those using topiramate, should be educated in the prevention of urinary calculi development, including adequate water intake, low oxalate ingestion, and avoidance of exposure to lithogenic agents.
In conclusion, this large-scale, case-control, population-based longitudinal study revealed an association between migraine and the risk of developing urinary calculi, independent of topiramate usage. Our study has important clinical implications, but further research is needed to delineate the mechanisms underlying urinary calculi development in patients with migraine.
Clinical implications
Our study showed migraine was associated with an increased risk of urinary calculi, independent of topiramate use. A higher frequency of clinic visits was associated with a greater risk.
Footnotes
Author contributions
Min-Juei Tsai, Yung-Tai Chen and Shuu-Jiun Wang conceived and designed the study. Min-Juei Tsai and Yung-Tai Chen researched the data for the article and provided the first draft equally. Shuo-Ming Ou, Chia-Jen Shih and Kuan-Po Peng researched the data for the article. Chao-Hsiun Tang was responsible for the acquisition of the database. All authors interpreted the data, revised the manuscript for intellectual content, and gave the final approval of the final version of the draft. Shuu-Jiun Wang is the guarantor.
Ethics approval
This study was approved by the institutional review board of Taipei Veterans General Hospital, Taipei, Taiwan. This study is exempt from written informed consent because all information that would potentially expose a specific individual patient to identification has been encrypted. The confidentiality of the data abides by the data regulations of the Bureau of National Health Insurance and the National Health Research Institute.
Funding
This study was supported in part by grants from the Taiwan National Science Council (100-2314-B-010-019-MY2, 100-2314-B-010-018-MY3), Taipei Veterans General Hospital (VGHUST101-G7-1-1, V101C-106, V101E7-003), NSC support for the Center for Dynamical Biomarkers and Translational Medicine, National Central University, Taiwan (NSC 100-2911-I-008-001), Brain Research Center, National Yang-Ming University and a grant from Ministry of Education, Aim for the Top University Plan.
Conflicts of interest
Shuu-Jiun Wang has served on the advisory boards of Allergan and Eli Lilly Taiwan. He has received speaking honoraria from local companies (Taiwan branches) of Pfizer, Elli Lilly and GSK. He has received research grants from the Taiwan National Science Council, Taipei Veterans General Hospital and Taiwan Headache Society. The other authors have nothing to declare.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.