
Abstract
Aims
The aims of this article are to characterize the headache in idiopathic intracranial hypertension (IIH) and to field-test the ICHD diagnostic criteria for headache attributed to IIH.
Materials and methods
We included 44 patients with new-onset IIH. Thirty-four patients with suspected but unconfirmed IIH served as controls. Headache and other IIH-related symptoms were assessed by a detailed standardized interview. In participants referred before diagnostic lumbar puncture (n = 67), we recorded headache intensity before and after cerebrospinal fluid (CSF) withdrawal.
Results
Headache in patients with IIH was daily occurring in 86%, focal in 84% and pulsating in 52%. Aggravation of headache by coughing or straining and relief after CSF withdrawal were significantly more frequent in patients than in controls (p ≤ 0.002). From the ICHD-2 to the ICHD-3 beta classification the sensitivity increased from 60% to 86% whereas the specificity decreased from 86% to 53%. Based on our data the headache criteria can be revised to increase sensitivity to 95% and specificity to 65%.
Conclusion
Aggravation of headache by coughing or straining, relief after CSF withdrawal, retrobulbar pain and pulsatile tinnitus may suggest intracranial hypertension. Based on data from a well-defined IIH cohort, we propose a revision of the ICDH-3 beta diagnostic criteria with improved clinical applicability and increased sensitivity and specificity.
Keywords
Introduction
Headache, in addition to visual loss, is the major complication of idiopathic intracranial hypertension (IIH). Headache is present in more than 90% of patients at time of diagnosis, and in more than two-thirds headache persists as a chronic and disabling symptom even after other symptoms and signs of active disease have resolved (1,2). The clinical hallmarks of IIH are elevated intracranial pressure (ICP) and bilateral papilledema. However, manometric ICP recordings may erroneously be elevated if patients are incorrectly positioned or anxious (3), or they may falsely show normal pressure in patients with intracranial hypertension due to marked spontaneous fluctuations in ICP (4). Likewise detection of subtle papilledema and the differentiation of true papilledema from various causes of pseudopapilledema may be difficult (5). Clinically relevant and valid classification criteria of IIH-related headache are thus essential to support the correct identification of patients with IIH.
The aim of this case-control study was to characterize the headache in patients with IIH at time of diagnosis and to field test the International Classification of Headache Disorders, second edition (ICHD-2) (6) and the International Classification of Headache Disorders, third edition beta (ICHD-3 beta) (7) criteria of headache attributed by IIH.
Methods and materials
Participants
This case-control study was conducted from 2011 to 2013. We recruited patients referred to the Danish Headache Centre (DHC), the Department of Neurology or the Department of Neuro-Ophthalmology, Glostrup Hospital under suspicion of having IIH. Individuals without headache were excluded. Final sample size was determined by the number of eligible subjects referred in the inclusion period. Patients with IIH according to the Friedman and Jacobson Criteria (8) were included as cases. Only patients who could be evaluated by the investigators before or within seven days of diagnostic ICP measurement were included. Subjects with normal ICP and no neuro-ophthalmological signs of IIH were included to constitute the control group (detailed description is presented in Figure 1).
Overview of participants included in the study.
Standard protocol approvals, registration and patient consents
Individuals gave written, informed consent to participate in the study. The study was conducted in accordance with the Declaration of Helsinki and approved by the Regional Ethics Committee (protocol H-3-2011-016).
Interview
We assessed a detailed patient history in all participants by a comprehensive, standardized and structured interview including demographics, prior medical history and exposures, detailed information of current and prior headaches, and visual disturbances and other symptoms. Interviews were performed face to face and prior to diagnostic lumbar puncture (unless this was already performed prior to referral (Figure 1)).
General examination
Patients and controls underwent a complete somatic and neurological examination including weight and height recordings and direct ophthalmoscopy performed by an experienced physician (HY). Computed tomography (CT) or magnetic resonance (MR) imaging was performed all subjects. In all patients with elevated ICP, venous sequences were performed. A thorough standardized neuro-ophthalmological examination, including visual acuity (Snellen), color-vision (Ishihara), automated visual field examination (Humphrey 30-2), slit lamp examination, examination of motility and pupils, indirect ophthalmoscopy, fundus photo and optical coherence tomography, was performed in all patients. Controls, in which initial direct ophthalmoscopy could not undoubtedly rule out papilledema (due to congential crowded optic disc or otherwise abnormally appearing disc) underwent the same neuro-ophthalmological examination programme to confirm abscense of papilledema.
Lumbar puncture and ICP measurement
We measured ICP by standardized lumbar puncture manometry performed in the lateral decubitus position. Patients had their legs straightened and were given a minimum of 10 minutes and instructed to relax before a stabilized opening pressure was recorded. After opening pressure was recorded we collected cerebrospinal fluid (CSF). In patients with opening pressure >250 mm H20, CSF was withdrawn until a final ICP of 120–170 mm H20 could be recorded. In controls 5–10 ml (depending on opening pressure) of CSF was withdrawn. CSF from all participants was sent for standard cytological and biochemical analysis.
Effect of CSF withdrawal
Patients were asked to report headache intensity on a visual analog scale (VAS) ranging from 0 (no pain) to 10 points (extreme pain) before and after lumbar puncture. The initial headache rating was performed before any steps of the procedure were initiated and the final assessment was performed 10–15 minutes after the procedure had been completed. We did not inform patients of any possible effect of CSF withdrawal on headache, and patients were blinded to the outcome of ICP measurement at time of final headache rating.
Testing the ICHD criteria
International Classification of Headache Disorders, second edition (ICHD-2) criteria for headache attributed to IIH (6).

IIH: idiopathic intracranial hypertension; CSF: cerebrospinal fluid.
International Classification of Headache Disorders, third edition beta (ICHD-3-beta) criteria for headache attributed to IIH (7).
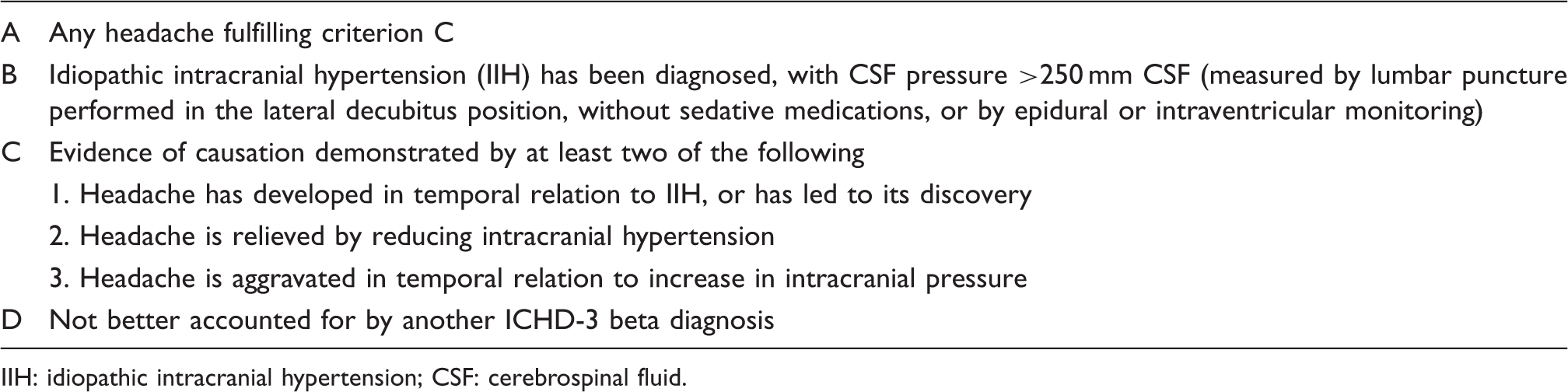
IIH: idiopathic intracranial hypertension; CSF: cerebrospinal fluid.
Based on the collected material we tested four different sets of criteria for IIH headache and evaluated them in respect to sensitivity and specificity.
In patients with no headache at time of lumbar puncture (n = 4, Figure 1) criterion ICHD-3 beta, C2 and the criterion C2.a of the new diagnostic criteria proposed by the authors were considered unfulfilled.
Statistical analysis
Statistical analyses were conducted using SAS 9.3. Significance levels were set at <0.05. Age and body mass index (BMI) of patients with IIH and controls were compared using two-tailed t-test. Differences in headache relief after CSF withdrawal, characteristics of headache and other symptoms were investigated by the Chi-square test. We calculated sensitivity, specificity according to standard statistical definitions (9).
The relationship between ICP and headache intensity (reported immediately before lumbar puncture) was explored using Spearman rank order correlation.
Results
We included 44 patients with new-onset IIH and 34 controls in whom the diagnosis of intracranial hypertension was disconfirmed (Figure 1). Bilateral papilledema was found in 39 (89%) patients. The remaining five patients had no clinically detectable papilledema.
Demographics and headache characteristics in patients with IIH and in controls.
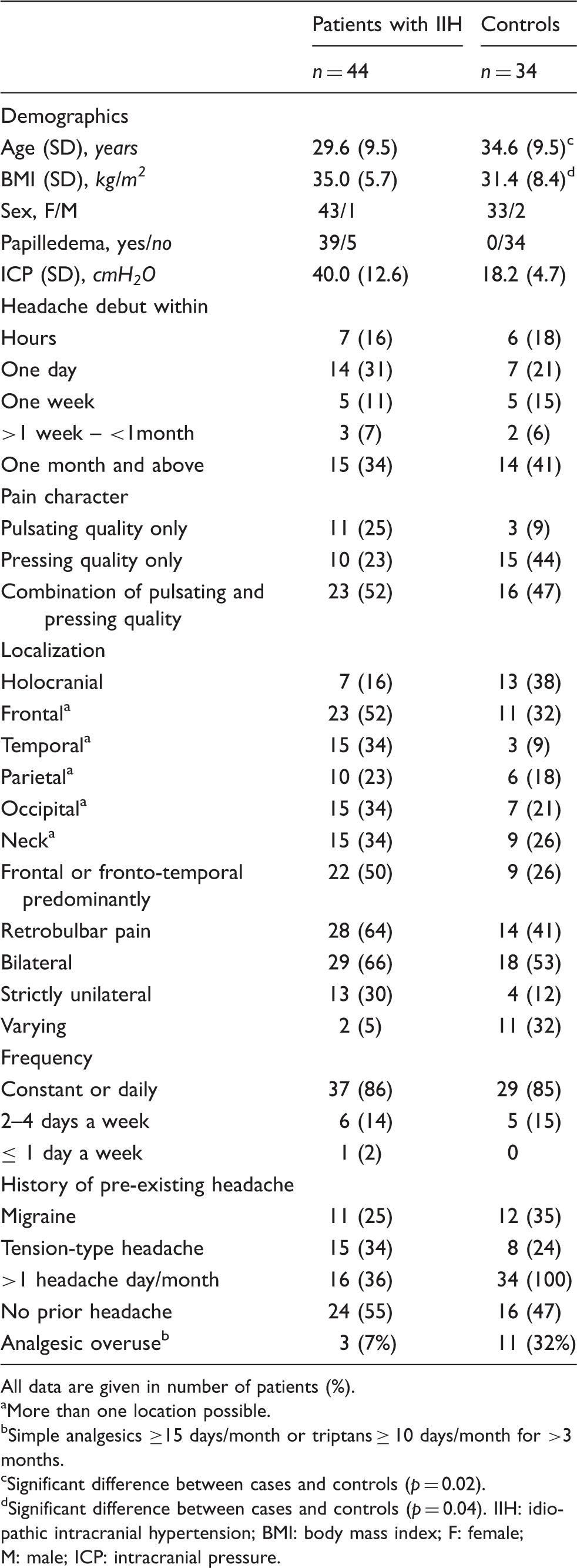
All data are given in number of patients (%).
More than one location possible.
Simple analgesics ≥15 days/month or triptans ≥ 10 days/month for >3 months.
Significant difference between cases and controls (p = 0.02).
Significant difference between cases and controls (p = 0.04). IIH: idiopathic intracranial hypertension; BMI: body mass index; F: female; M: male; ICP: intracranial pressure.
Headache characteristics and other symptoms in patients with IIH and controls
Headache in the majority of patients with IIH was focal (84%) and daily occurring (86%). In 45% of the patients location was purely fronto-temporal and 77% reported that their headache was at least partially of pulsating quality (Table 3). Strictly unilateral location was reported by 13 patients (30%). Only four of them had a history of pre-existent episodic migraine (one to 12 attacks/year) with (n = 2) or without aura (n = 2).
Although 45% of the patients had a history of pre-existent headache, the majority of patients (75%) reported that they were able to distinguish IIH-related headache from prior headaches based on intensity, duration, character and or localization.
Sensitivity and specificity of headache characteristics and other symptoms of patients with idiopathic intracranial hypertension (IIH) (n = 44) compared to controls (n = 34).

Significant p-values are shown in bold.
Visual disturbances were generally a frequent complaint in patients with IIH. However, blurring of vision (not aura) was reported in more than half of controls, quite similar to the frequency in patients with IIH. Transitory visual obscurations (TVOs) were significantly more frequent in patients with IIH (64%), but were also commonly reported by controls (35%). While TVOs were unilateral in 25% of patients, all but one control (92%) reported bilateral symptoms (92%).
Headache relief after CSF removal
Headache relief after lumbar puncture and CSF removal.

CSF: cerebrospinal fluid; BMI: body mass index; F: female; M: male; ICP: intracranial pressure; VAS: visual analog score. Significant p-values are shown in bold.
Withdrawal of CSF was followed by headache relief in most of the patients with IIH (sensitivity 72%). However, it was not exclusively seen in patients, but in fact reported in nearly a quarter of controls (specificity 77%). We found no correlation between headache intensity at time of lumbar puncture (patients with IIH) and ICP (p = 0.84, ρ = 0.03).
Sensitivity and specificity of the ICHD diagnostic criteria
Proportions of individuals satisfying the headache-related criteria of ICHD-2 and ICHD-3 beta are shown in Figure 2. While revision of the ICHD-2 criteria to ICHD-3 beta increased the sensitivity from 60% to 86%, the specificity was reduced from 86% to 53%. Based on data from our study, we could modify the present criteria (Table 6) and increase sensitivity to 95% and the specificity to 65% (Figure 2).
Proportions of patients and controls satisfying ICHD-2, ICHD-3 beta and the new criteria proposed by the authors. Proposed diagnostic criteria for headache attributed to idiopathic intracranial hypertension. CSF: cerebrospinal fluid; ICHD-3-beta: International Classification of Headache Disorders, third edition beta.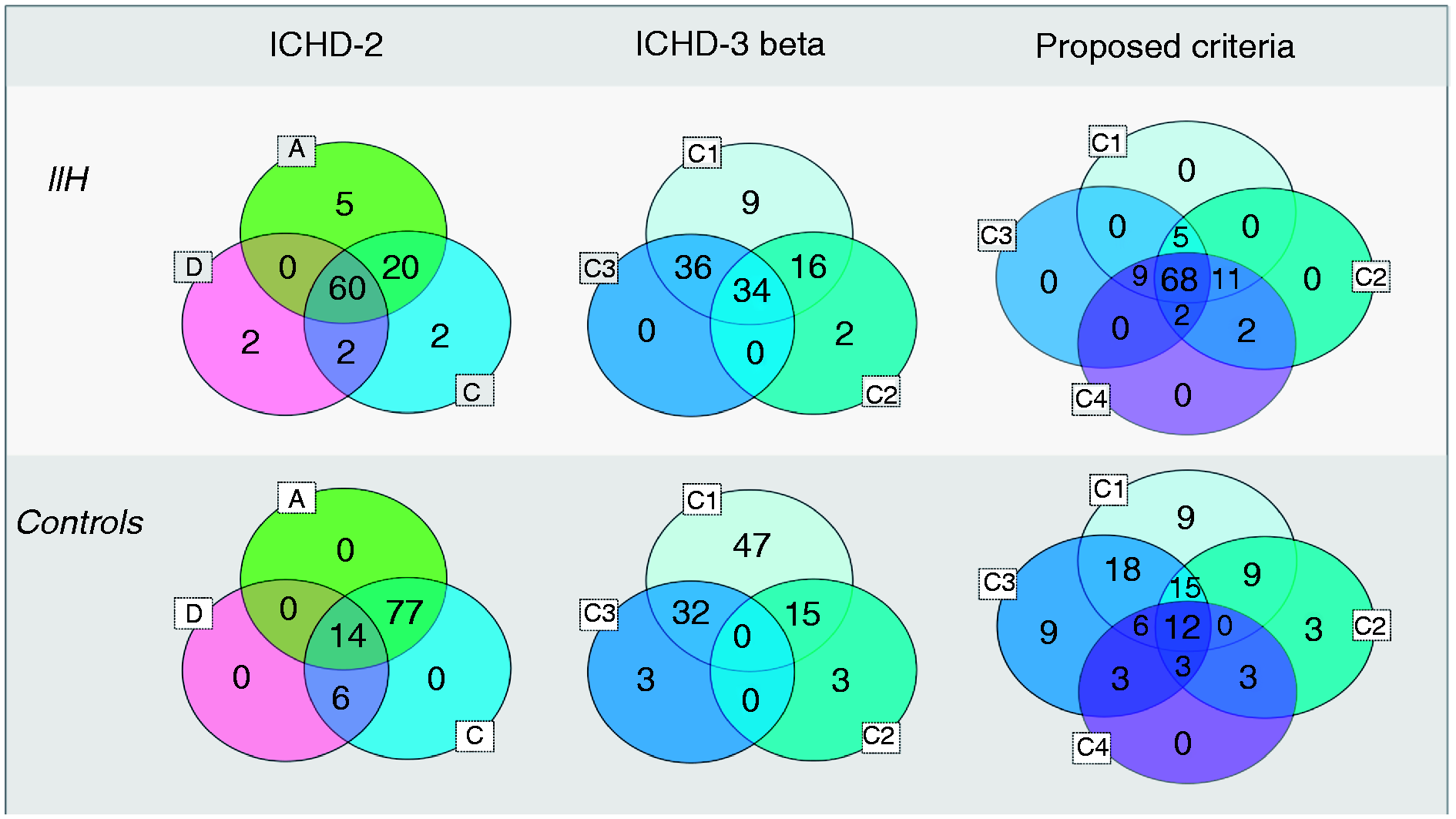

Discussion
Relief of headache after reduction of intracranial hypertension is a main feature of the ICHD-2 diagnostic criteria for “headache attributed to idiopathic intracranial hypertension” (6) and is maintained as a characteristic in the ICHD-3 beta version of the criteria just published (Tables 1 and 2) (7). Although improvement of headache and other symptoms after CSF removal has been reported by several authors (2,10–13) our study, to our knowledge, is the first to ever validate the diagnostic value of this criterion in a controlled design. In addition we for the first time explored the specificity of several other headache characteristics believed to be associated with IIH. Based on these systematically recorded data, we tested the ICHD-2 and ICHD-3 beta and propose a new set of validated diagnostic headache criteria.
We found that CSF withdrawal and normalization of ICP immediately improved the headache in 72%. In comparison headache relief was reported by only 23% of controls with normal opening pressure. Immediate headache relief after CSF removal thus seems to have a fairly good specificity (77%) for separating patients with true IIH from phenotypical similar patients.
Daily occurrence of headache attributed to IIH as described in the ICHD-2 criteria was reported by 82% of our patients. This is consistent with previous studies reporting daily headaches in between 67% and 93% of the patients (10,11,14–16). Likewise aggravation of headache by coughing or straining was both sensitive (70%) and specific (65%) to increased ICP (ICHD, A3). In contrast we could not confirm the characteristics of the diffuse and non-pulsating pain described in ICHD-2. Non-pulsating pain was reported by only 23% of our patients while 25% reported that headache was always pulsating. That IIH-related headache is in fact more likely to be pulsating, or at least have pulsating elements, is supported by other studies reporting this quality in between 70% and 83% of patients (11,14,15).
Diffuse holocranial headache was reported by only 16%. Twelve patients (30%) reported strictly unilateral headache although only four of them had a history of pre-existent migraine. In almost half of our patients headache was strictly fronto-temporal. This is consistent with other studies (10,11,14,15) including the one by Fay et al. (17) in which headaches resulting from experimentally induced intracranial hypertension were always frontally and temporally located.
Headache related to IIH has been described as typically worse in the morning and aggravated by postural changes (14,18). Theoretically this could be expected because of transient increase in ICP caused by supine position and CO2 retention during sleep. We, however, found no evidence for either of these symptoms being associated with intracranial hypertension.
In the newly published ICDH-3 beta version the criteria of headache attributed to IIH have undergone substantial changes. The IIH headache is expected to respond to increased and reduced ICP, but in contrast to the ICHD-2, ICP levels are unspecified and no other pain characteristics are required. Accordingly we found that sensitivity increased from an unacceptably low sensitivity of ICDH-2 (60%) to 86% (Figure 2). However, this came at a cost of substantially reduced specificity (from 86% to 53%).
To test the ICHD criteria in our material, we had to make some assumptions and modifications (described in the methods). Disappearance of headache within 72 hours of normalization of ICP (ICHD-2, D Table 1) would require continuous ICP measures and tightly controlled ICP. Because of invasiveness and ethical concerns, cost and logistics, this was not possible in our study. Most important, it would very rarely be applicable in the clinical settings. Likewise the criterion “temporal relation of headache development and increase in ICP” (ICHD-2, C) is difficult to achieve retrospectively and thus nearly always remains speculative. To minimize the impact of individual interpretation, we suggest that criteria be kept as tangible and clinically applicable as possible. The ICHD-3 beta already revised the criteria of causation by adding “headache leading to its (IIH) discovery” (ICHD-3 beta, C1). However, based on our material we found that IIH is often discovered only after visual symptoms lead to ophthalmological examination. We therefore suggest that the assumption that headache is related to ICP elevation instead be based on development of a new kind of headache or a clear exacerbation of pre-existing headache (13,19) (Table 6). For the criteria of headache response to ICP levels (ICHD-3 beta, C2 and C3) we suggest that indices of ICP alterations remain clearly specified and testable (Table 6).
Optimal balance between clinically relevant sensitivity and specificity is the foundation of diagnostic criteria. And although sensitivity is pivotal in IIH we find that the reduction of specificity to 53% by ICHD-3 beta is unfortunate. It may increase the potential false-positive diagnosis (especially prone in patients without papilledema) that may cause considerable problems. In our proposed modification of the criteria we were able to improve specificity to 65%. Although an even higher specificity would have been preferred it should be kept in mind that the C-criterion tested in this study is only a supplement to the main criteria of IIH (8,20). The purpose of the criteria is primarily to support the clinical suspicion of IIH and raise alertness to the differential diagnosis and the need for additional investigations, rather than to establish the diagnosis. Based on this we suggest that a more detailed description of the IIH-related headache be included in the new diagnostic criteria. In addition to headache characteristics we included papilledema and/or pulsatile tinnitus as a sub-criterion urging that absence of both makes the headache less likely to be attributed to IIH. Pulsatile tinnitus is reported more frequently in IIH with papilledema compared to IIH without papilledema probably reflecting the higher ICP found in IIH with papilledema (21).
The validity of the set of characteristics proposed in this study is supported by the large proportion of patients (at least 68%) fulfilling all four of the sub-criteria.
The ICHD-3 beta has added criteria D, “not better accounted for by other ICDH-3 criteria.” This is an important supplement to the diagnostic criteria as IIH may mimic the primary headaches, especially chronic migraine or chronic tension-type headache (2), which on the other hand commonly coexist in patients with IIH.
In addition to headache we explored the diagnostic value of other IIH-related symptoms. Interestingly, blurring of vision (other than aura) was reported by 58% of the controls even though all but three (with unilateral optic disc edema caused by AION or prior optic neuritis) patients had normal-appearing fundi and no history of ocular disease. This stresses the very unspecific and subjective nature of visual blurring in patients with headache. Transitory visual obscurations, although more specific than visual blurring, were not uncommon in controls.
The strength of this study is the prospective and case-controlled design, a well-defined study population including only newly diagnosed patients with treatment-naive IIH. Controls were sex matched and of similar age with only slightly lower BMI, thus representing a relevant population that clinically may be difficult to distinguish from patients with IIH. Assessment of headache and other symptoms was standardized and primarily performed prior to lumbar puncture and neurological examination, thus blinded to ICP status. Complete blinding, however, was not always possible because of information of suspected papilledema from referring units in many of the patients with IIH.
The study was limited by the relatively short monitoring of headache relief after CSF withdrawal and by the history of pre-existing primary headaches in almost half of the patients. Even though the majority of patients with pre-existing headache reported changes in headache character in relation to diagnosis, we cannot completely rule out the influence of non-IIH headache as features may overlap. In addition the selection of controls from patients initially suspected of having IIH biased the specificity calculations. Inclusion of a control group of patients with pure primary headaches would address this. However, phenotypically they may not have been as good a match and performing lumbar puncture for ICP measurement in these patients without clinical indication would cause ethical concerns.
In conclusion, we suggest modifications of the current criteria for IIH-related headache and demonstrate an excellent sensitivity, and an improved specificity and applicability compared to the ICHD-3 beta criteria. Diagnostic criteria that can raise specificity further are desirable. However, as headache attributed to IIH mimics the primary headaches, this may be difficult to obtain. The diagnosis of headache attributed to IIH thus remains a challenge and should be subject to high levels of clinical awareness.
Clinical implications
Headache attributed to idiopathic intracranial hypertension (IIH) is mostly daily occurring, and often focal and/or pulsating, thus resembling chronic migraine. Headache relief after cerebrospinal fluid (CSF) withdrawal indicates that headache may be attributed to IIH. Blurring of vision is unspecific and not a valid symptom of IIH in patients without papilledema. The diagnostic criteria of headache attributed by IIH as suggested by the authors may help support the clinical suspicion of IIH and raise alertness to the differential diagnosis and the need for additional investigation. It is important to note that the headache criteria described in the International Classification of Headache Disorders (ICHD) describe headache attributed to IIH and are only supplementary to the main criteria of IIH. The diagnosis of IIH itself should always be based on the main criteria of the disease (8,20).
Footnotes
Funding
This work was supported by grants from Region Hovedstadens Forskningsfond. The funding sources had no role in the study design; in the collection, analysis and interpretation data; in the writing of the report; or in the decision to submit the paper for publication.
Conflict of interest
H. Yri has received honoraria for consultant work from NeuroCore and a travel grant from Berlin-Chemie Menarini. R. Jensen has received honoraria for lectures and patient leaflets from MSD, Berlin-Chemie Menarini, ATI and Pfizer and serves on medical advisory boards for LindeGas, ATI and Neurocore.
Acknowledgments
We thank Winnie G. Nielsen, BA, Lene Elkjær, BA, and especially Hanne Andresen, BA, for their tireless efforts and technical assistance during data collection (ICP measurements). We thank neuro-ophthalmologists Marianne Wegener, MD, and Steffen Hamann, MD, PhD, for their thorough ophthalmological examination and evaluation supporting the diagnosis in our patients and controls.