
Abstract
Objectives
The objective of this article is to compare the diagnosis of menstrual migraine without aura (MM) from a clinical interview with prospective headache diaries in a population-based study.
Material and methods
A total of 237 women with self-reported migraine in at least half of menstruations were interviewed by a neurologist about headache and diagnosed according to the International Classification of Headache Disorders II (ICHD II). Additionally, the MM criteria were expanded to include other types of migraine related to menstruation. Subsequently, all women were asked to complete three month prospective headache diaries.
Results
A total of 123 (52%) women completed both clinical interview and diaries. Thirty-eight women were excluded from the analyses: Two had incomplete diaries and 36 women recorded ≤1 menstruation, leaving 85 diaries eligible for analysis. Sensitivity, specificity, positive and negative predictive value and Kappa for the diagnosis of MM in clinical interview vs. headache diary were 82%, 83%, 90%, 71% and 0.62 (95% CI 0.45–0.79). Using a broader definition of MM, Kappa was 0.64 (95% CI 0.47–0.83).
Conclusion
A thorough clinical interview is valid for the diagnosis of MM. When this is undertaken, prospective headache diaries should not be mandatory to diagnose MM but may be necessary to exclude a chance association.
Keywords
Introduction
Menstrual migraine without aura (MM) is, according to the International Classification of Headache Disorders (ICHD) II and III beta version, defined as attacks of migraine without aura (MO), occurring between days −2 to +3 of the menstrual cycle in at least two out of three menstruations (1,2). It is subdivided into two types; pure menstrual migraine, characterized by MO attacks occurring exclusively in the defined perimenstrual period, and menstrually-related migraine in which non-menstrual migraine attacks also occur.
MM differs from most of the other conditions in the ICHD by virtue of the temporal relationship with a specific event, i.e. menstruation. Accordingly, the establishment of the diagnosis needs both a precise headache diagnosis and the correct timing and frequency of attacks associated with menstruation. Three previous studies have demonstrated this challenge, as MM was over-reported by 83%, 62% and 19% of women by self-assessment (3–5). Another concern is that the diagnostic criteria for MM are interpreted differently among researchers. There are an increasing number of studies that pool data and analyze the attacks that occur between days −2 to +3 without evidence that these women have MM. In order to avoid both an overestimation of MM and to confirm that the women have migraine attacks associated with menstruation that are more than a chance occurrence, the recommendation of prospective headache diaries was changed to a requirement in the current beta version of the ICHD III (1). Thus, MM is the only diagnosis throughout the classification in which a prospective headache diary is required. However, the validity of a MM diagnosis from a physician’s interview based on the ICHD criteria, rather than by self-assessment, has never been evaluated.
The aim of this study was to compare the diagnoses of MM from a clinical interview with a three-month prospective headache diary. Additionally, we expanded the MM criteria in order to explore other types of migraine related to menstruation.
Material and methods
Questionnaire, interview and diary
The study was divided into three steps; (1) a mailed screening questionnaire in 2005, (2) a clinical interview and a physical/neurological examination by a physician during 2011–2012, and (3) prospective headache diaries for three months directly following the interview.
A screening questionnaire about headache, migraine and its relation to menstruation was mailed to 5000 women aged 30–34 years from the general population. The screening questionnaire had two separate purposes: One was to study chronic headache and the second was to study menstrual migraine. Different populations were studied, since the present study excluded women with chronic headache. The delay between screening and interview was caused by lack of resources. The response rate was 73% and the question: “How often do you experience migraine in relation to menstruation?” was used to identify women with possible menstrual migraine. All women who reported migraine in at least half of their menstruations and <180 headache days/year were invited to a clinical interview and examination six years later. Of 360 women meeting the inclusion criteria, four had emigrated, nine had insufficient Norwegian language skills and 39 did not reply to five or more phone calls. Among the 308 eligible women, 237 (77%) participated in the interview. The interview focused on headache, migraine and its relationship to menstruation. Participants unable to meet at the clinic were interviewed by telephone (87/237). The headaches were classified according to the ICHD II, including the appendix criteria for MM. In addition, we expanded the criteria to include migraine with aura (MA) by applying the appendix criteria for MM to a migraine diagnosis of MA. We also included probable menstrual MO and probable menstrual MA, i.e. if the MM criteria were fulfilled except for one criterion (i.e. frequency or timing of attacks), similar to that of probable migraine in the ICHD III beta version, but attacks were at a minimum required in 50% of menstrual cycles. A more exhaustive description of the screening method and interviews are published elsewhere (6).
Subsequently, the women were instructed to complete a prospective paper-pencil headache diary for three months. When a headache occurred, the women filled in: time of onset and end of headache, aura symptoms, pain quality, pain location, severity on numeric rating scale 0–10 (NRS; 0 = no pain, 10 = most severe pain), aggravation by routine physical activity, associated symptoms (nausea, photo- and phonophobia), medical treatment (time taken, type and dose), and sick leave. In addition, they were asked to record each day of uterine bleeding. Women were allowed to take their usual symptomatic attack treatment, continue migraine prophylaxis and hormonal contraception, if used. The diaries were returned by mail in a stamped, self-addressed envelope. If a diary was not returned after three months, one reminder was issued.
Data entry and analysis of diaries
The diaries were reviewed by two investigators (KGV and MBR) and the diary database was constructed by KGV. The diaries did not cover information about name or diagnoses of the participants. In order to merge the data from interviews and diaries, a five-digit identification number was placed on the front of each diary. In cases with missing or imprecise information with respect to the first day of menstruation, the participant was contacted per telephone to elaborate the information. When a migraine attack lasted more than one day, it was considered as a single multiday attack, unless an interval of ≥48 hours pain free separated the headaches. This definition was used since most of the attacks were treated with symptomatic drugs and headache occurring within 48 hours is considered as relapse of migraine in randomized controlled drug trials (7). When all but one ICHD criterion for MO were fulfilled, the attack was considered as MO if symptomatic treatment was used. A diagnosis of MM required at least two MO attacks with onset on day 1 ± 2 of the menstrual cycle during three consecutive cycles. In women who recorded only two menstruations, MM was diagnosed if MO occurred in both menstruations. If an attack started outside the defined period (day 1 ± 2), it was considered as a non-menstrual attack. For the analysis of MM, only women fulfilling the current ICHD criteria for menstrual migraine were included. Separate analyses were made for the expanded criteria. Women who experienced ≤1 menstruation were excluded from analyses.
Statistics
The data were analyzed using the Statistical Package of Social Sciences (SPSS) version 20. The sensitivity, specificity and predictive value of the interview-diagnoses were assessed. Kappa-statistics with 95% confidence interval (CI) and McNemar’s test for symmetry were used to compare diagnoses from interviews and diaries. Demographic data and comparisons of women with/without MM were compared with χ2 test for categorical variables and independent t-test for continuous variables. Estimations of significance were two sided and a p level <0.05 was considered significant.
Ethics
The study was approved by the Regional Committee for Medical Research Ethics and the Data Protection Authorities. The participants received written and verbal information about the project and inclusion was based on informed consent. No compensation for compliance/participation was given.
Results
A total of 123 (52%) women returned diaries and among these, two lacked complete information regarding the exact timing of menstruation and were therefore excluded from the analyses. Another 36 women were excluded because ≤1 menstruations were recorded. Reasons for oligo-/amenorrhea were progestogen-only contraception (n = 21), hysterectomy (n = 4), pregnancy/lactation (n = 4), early menopause (n = 1), irregular cycle length (n = 2), pregnancy (n = 1) and unknown cause (n = 3). Thus, 85 diaries were eligible for analysis (Figure 1).
Flowchart.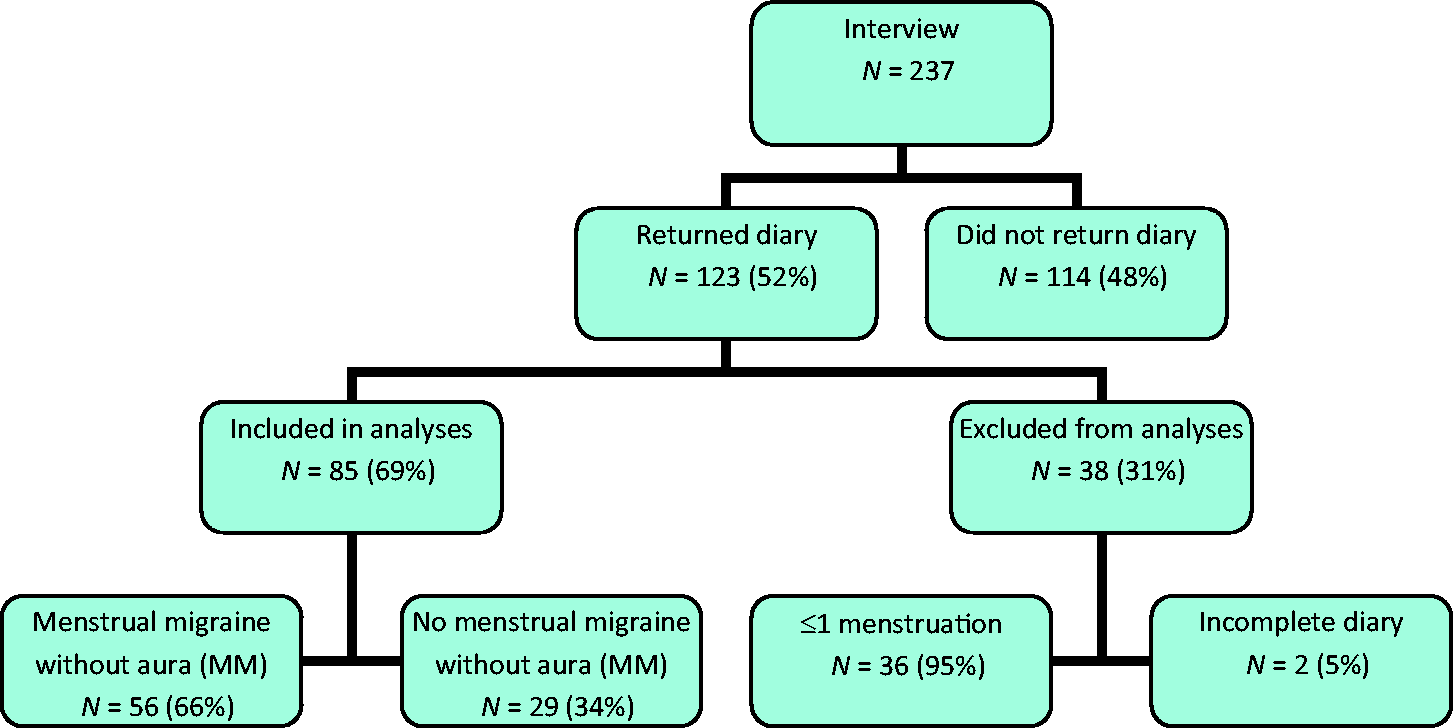
Clinical characteristics of women with and without menstrual migraine without aura (MM).
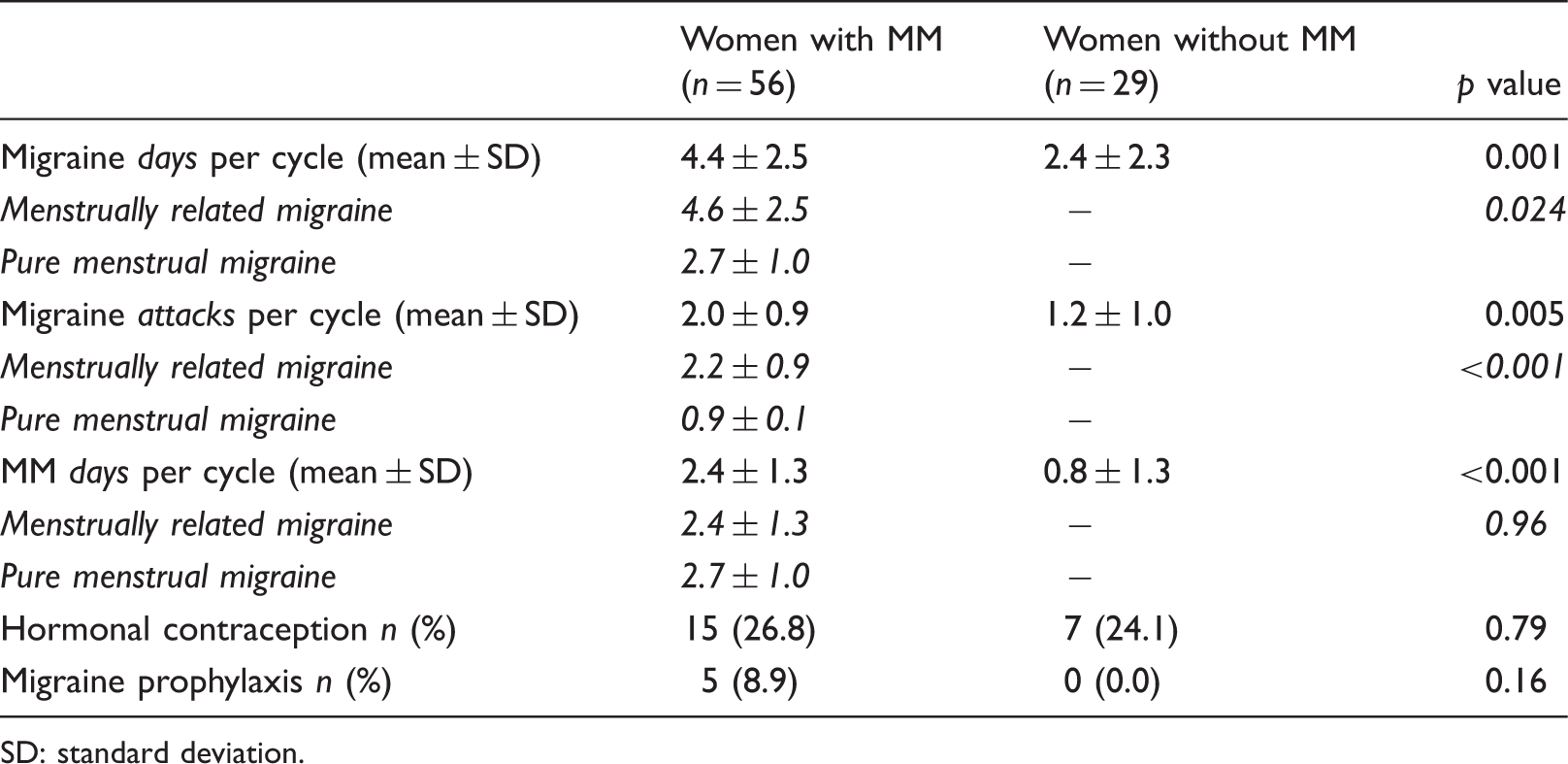
SD: standard deviation.
Responders vs. nonresponders
Comparison of women; diary responders vs. nonresponders.

36 missing values. b41 missing values. NOK: Norwegian kroner (currency).
Interview vs. diary
MM according to the ICHD criteria
Sensitivity, specificity and predictive values of interview diagnosis of menstrual migraine without aura (MM).
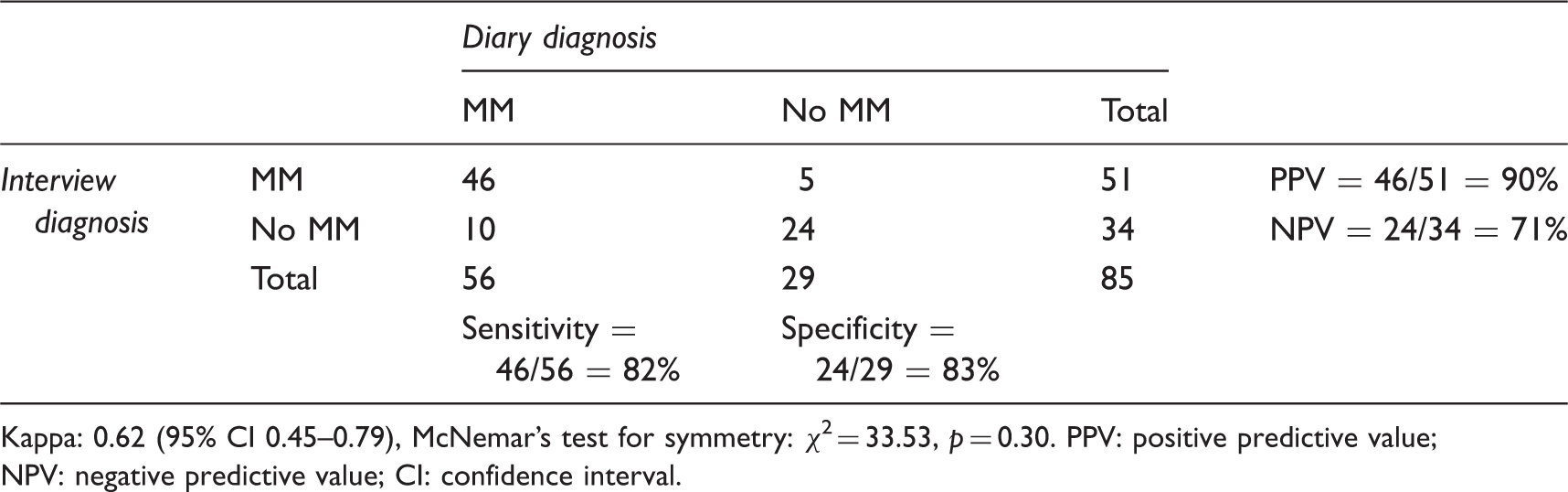
Kappa: 0.62 (95% CI 0.45–0.79), McNemar’s test for symmetry: χ2 = 33.53, p = 0.30. PPV: positive predictive value; NPV: negative predictive value; CI: confidence interval.
A total of 46 women fulfilled MM criteria both in diary and interview (Table 3). Among the 10 women negatively misclassified as no MM in the interview, four reported no menstrual relationship of their migraine. The remaining six reported an association between migraine and menstruation in the interview, but did not fulfil the required frequency (<2/3 of menstruations, n = 4), timing of the attacks (onset of MO on day 4, n = 1) or headache diagnosis (probable MO n = 1). Among the five women positively misclassified by interview, two women regularly had migraine attacks that started earlier (day −4 or −5) than required, but still showed a clear menstrual pattern. The remaining three women had attacks randomly distributed across the menstrual cycle, with no increase perimenstrually.
A total of seven women were identified with pure menstrual migraine in the diaries and eight by interview. In only three cases did it represent the same woman. Among the five women positively misclassified by interview, three had menstrually related migraine and two no MM. Negative misclassification of pure menstrual migraine occurred in four women, of whom three had menstrually related migraine and the remaining no MM.
Expanded criteria of menstrual migraine
The group with expanded criteria for menstrual migraine comprised four women with menstrual MA, two women with probable MO related to menstruation and the 56 women with MM. When we compared the diagnoses from interviews and diaries, the observed agreement rate was 86% and the Kappa value 0.64 (95% CI 0.47–0.83) with equal positive and negative misclassification (six in each group). The corresponding sensitivity, specificity, positive and negative predictive values was 90%, 75%, 90% and 75%.
All four women with menstrual MA by interview recorded aura symptoms (visual, sensory, or both) preceding their menstrual migraine attacks in the diaries. Both women who were diagnosed with probable MO associated with menstruation in the interview fulfilled the MM criteria in the diaries. Among women who stated that their migraine occurred in <2/3 but ≥1/2 of menstruations, three of four had MM in the diaries.
Discussion
This is the first study validating MM diagnoses from a clinical interview based on the ICHD criteria with a prospective headache diary. Our main finding was that the clinical interview is valid for the diagnosis of MM since the chance-corrected agreement rate was (Kappa) 0.62, which is defined as substantial agreement (8). This was also true by expanding the group with menstrual MA and probable menstrual MO.
Discussion of the results
The present study differs from previous studies because our interview diagnoses were strictly based on the ICHD criteria and not by self-assessment. We used the same definitions of MM both in interviews and diaries, while the definitions seem to vary between interview and diaries in two other studies (3,5). Additionally, all participants in our study were asked to complete a diary, including those who were not diagnosed with MM by interview. In this way we actually identified an underreporting of MM: More women had MM in diaries than by interviews. Further, six of 10 of the women who were misclassified as no MM by interview reported a menstrual association of their migraine and fulfilled all but one of the ICHD criteria for MM.
The over-reporting of MM by self-assessment may have contributed to the large prevalence figures of MM with occurrence up to 50%–70% among female migraineurs in previous studies (9–11). Based on interview diagnoses in our study population, only 17.6% of all female migraineurs had MM. In light of our findings using diaries, the prevalence of MM among women with migraine aged 36–40 years is approximately 20%. Additionally we identified women with other types of migraine related to menstruation, suggesting that about 25% of women with migraine have some form of menstrual migraine.
We found a high misclassification of pure menstrual migraine between interviews and diaries, as only three of seven women with this diary diagnosis reported pure menstrual migraine by interview. The four women with negative misclassification of pure menstrual migraine by interview recorded few migraine days in total (2.5 days/cycle) compared to all those with menstrually related migraine (4.4 days/cycle, Table 1). A three-month diary may have been too short to detect nonmenstrual attacks in these women. The women who were positively misclassified by interview also recorded fewer migraine days (2.3 days/cycle) than the average for women with menstrually related migraine (Table 1). This illustrates a difficulty of distinguishing between pure and menstrually-related migraine in menstrual migraineurs with lower attack frequency.
Women with MM had significantly more frequent migraine than women without MM, even though none of the participants had ≥15 headache days/month. This implies that women fulfilling the criteria for menstrually-related migraine are among high-frequency sufferers of migraine. However, the more frequent migraine a woman has, the greater is the chance that at least one of the attacks incidentally occurs within the five-day window. The first proposed diagnostic criteria of MM from 1988 referred to this issue: “It seems reasonable to demand that 90% of attacks should occur between two days before menses and the last day of menses” (12). In the revised versions of ICHD II and III beta, this perspective disappeared. Thus, women with frequent migraine may be diagnosed with MM according to the current criteria merely because they have a high attack frequency and not because of a true association between menstruation and migraine. Although the demand of 90% may seem too conservative, a limitation on the number of nonmenstrual attacks in the diagnostic criteria should be considered (13).
The diagnostic criteria of MM are placed in the appendix of the ICHD III beta version and are primarily considered as research criteria that need validation. We expanded these criteria to encompass all types of migraine related to menstruation, and identified four women with menstrual MA and two with probable menstrual MO. This is in line with the revised ICHD II criteria that included MO only in relation to the diagnosis of chronic migraine (14), while the ICHD III beta now includes all types of migraine in relation to chronic migraine (1). Although women with menstrual MA and probable menstrual MO account for only a small proportion of all women with migraine, it could be worth including them as a subgroup of MM in the revised version of the appendix criteria. Otherwise, potential pathophysiological mechanisms will never be explored.
Methodological considerations
We used a paper-pencil diary, which is low cost and easy to use. However, paper-pencil diaries are associated with drawbacks like low compliance and possibility for backfilling diary entries (15). The compliance in our study was low, as only 52% returned the diary; frequent reminders, or a compensation for filling in a diary, might have increased the return rate. It is, however, well known that compliance using headache diaries is low, even in headache clinics (3,16,17). Electronic diaries have both compliance and technical challenges and are associated with possible selection bias (18). During the past years, an increasing proportion of the population own a smartphone and numerous different headache diary applications (apps) are available for free. This fast-access and portable method may be the future method to use in order to achieve higher compliance rates.
Women who returned diaries did not differ significantly from women who did not return diaries, with respect to headache frequency and the diagnosis of MM in the interview. This indicates that the diaries are representative for all women who were interviewed. The six years’ delay between the screening questionnaire and the clinical interview did not influence our result, since it is the clinical and the diary data that are compared and these data were collected in close temporal relation.
We excluded 36 women with ≤1 menstruation, because it was impossible to judge whether they have MM or not exclusively based on diaries. Among these, 33 had oligo-/amenorrhea at the time of the interview and were diagnosed with MM based on their (previous) history before they became amenorrheic. In another three individuals, the menstrual situation changed during the three months directly following the interview. This shows that diaries are not perfect in detecting all women with menstrual migraine. Ideally, the clinical interview and diary should cover the same time period, which was not the case in our study. Thus, this might explain part of the disagreement, as migraine frequency as well as the menstrual situation may change with time.
Conclusion
Our study indicates that a thorough clinical interview is valid for the diagnosis of MM. When this is undertaken, prospective headache diaries should not be mandatory to diagnose MM, but can identify additional cases not recognized at the interview. Additionally, they can be used diagnostically to exclude a chance association and clinically, to monitor the efficacy of management.
Clinical implications
A clinical interview, based on the International Classification of Headache Disorders (ICHD) criteria, is valid for the diagnosis of menstrual migraine without aura. Prospective headache diaries are recommended to exclude cases with a chance occurrence and to monitor the efficacy of treatment.
Footnotes
Funding
This work was supported by grants from the South-Eastern Norway Regional Health Authority (grant number 2013001), Akershus University Hospital (grant number 2629014) and Institute of Clinical Medicine, University of Oslo.
Conflict of interest
None declared.