
Abstract
Introduction
Cluster headache is an excruciating unilateral headache with autonomic symptoms whose periodic nocturnal activity, which interrupts sleep, has been attributed to a hypothalamic generator.
Case report
We describe a patient with a longstanding episodic cluster headache who experienced, on two occasions, a period of nocturnal awakenings without pain or autonomic symptoms, lasting one week before the onset of a cluster bout. Awakenings occurred twice/night at the same hours of impending cluster attacks and had no apparent trigger, being unusual for this patient who had no previous sleep disturbances. Neurological examination and brain imaging were normal.
Discussion
This case documents two new aspects of cluster headache. It suggests that repeated nocturnal awakenings can be a warning sign of an impending cluster period, a finding that may have therapeutic implications, and also that hypothalamic activation may begin several days before trigemino-autonomic symptoms, thus behaving as a true bout generator.
Introduction
Cluster headache (CH) is one of the most intense types of pain, appearing in bursts of unilateral headache attacks with cranial autonomic symptoms with a typical periodic pattern. While its pathogenesis is unclear, there is increasing evidence about the pivotal role of the hypothalamus in this primary headache. In fact, it has a circadian and circannual rhythmicity, it has been associated with genetic disorders of the orexinergic system, the hypothalamus is activated during attacks, and its stimulation may relieve chronic forms of cluster (1,2). Yet, its cyclic activation occurs without warning. We describe a patient with longstanding episodic CH who experienced transient disruptions of the sleep-awake cycle immediately before two CH bouts. This case illustrates a possible clinical signature of the hypothalamic generator that may be a warning sign of an impending attack.
Case report
A 49-year-old man suffered from CH since the age of 36, with an average of one episode/year. Episodes were more likely to begin in October–November, lasted about two months and consisted of three attacks/24 hours (two nocturnal), lasting 45–60 minutes. During attacks excruciating pain was felt in the left eye and temple, associated with ipsilateral lacrimation, conjunctival injection, ptosis, eyelid edema and marked agitation.
Cluster headache bouts.
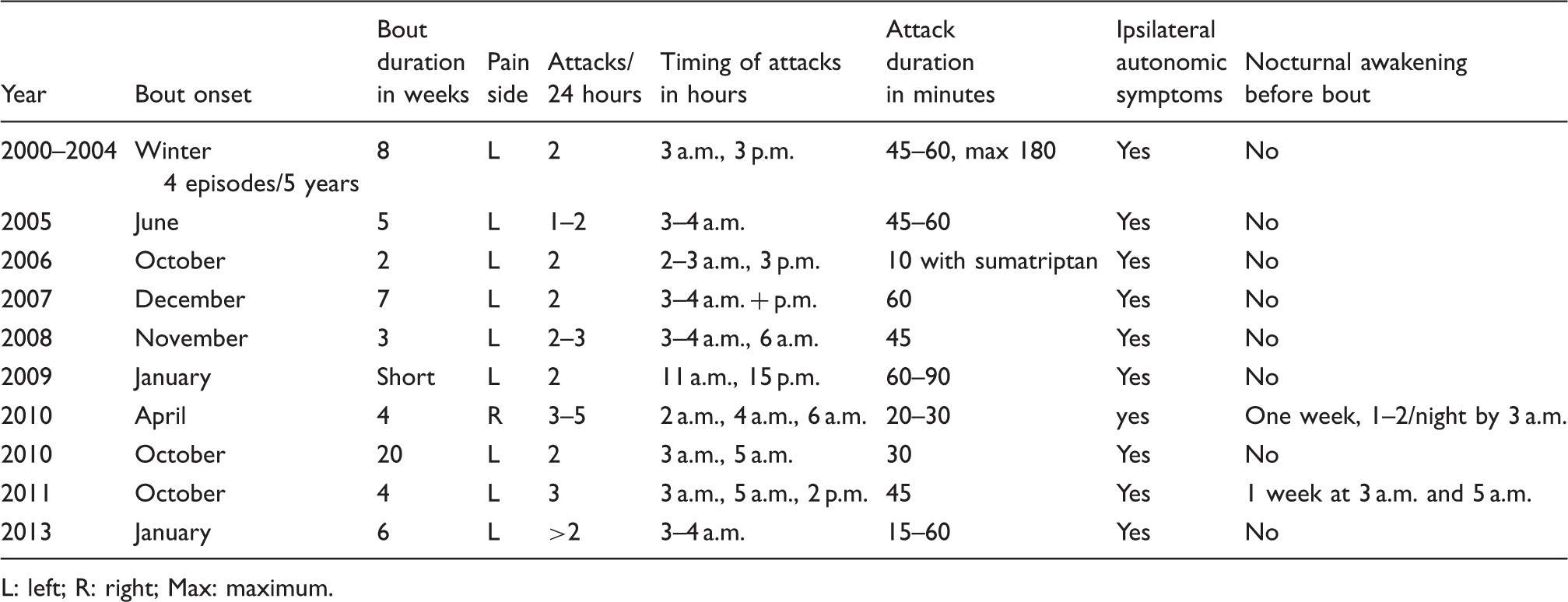
L: left; R: right; Max: maximum.
On two occasions the cluster period was preceded, for one week, by unexplained consecutive nocturnal awakenings, once or twice/night, at 3 a.m. and 5 a.m., without pain or autonomic symptoms. The patient described them as being suddenly fully awake, with no pain or restlessness, no need to get out of bed nor any other symptoms, and falling back asleep after 15–20 minutes. When this phenomenon occurred, for the first time, outside his usual cluster “season,” he did not associate it immediately with CH until the pain appeared seven days later. On the second occasion, nocturnal awakenings (two/night) occurred again during five consecutive nights before the onset of cluster attacks.
The patient is a smoker but is otherwise healthy. He has no depressive symptoms, no previous sleep complaints or any need to take sleeping medication and denies excessive daytime somnolence. Neurological exam, computed tomography (CT) and brain magnetic resonance imaging (MRI) are normal.
Discussion
A patient with episodic CH, fulfilling the ICHD-III beta diagnostic criteria (3), experienced on two occasions a warning sign of an impending cluster episode, characterized by recurrent cyclic nocturnal awakening, without pain or autonomic symptoms, with the same timetable as his imminent cluster attacks. There were no previous sleep complaints outside the cluster periods, nor any apparent trigger.
The repeated occurrence of these phenomena for five or seven consecutive nights, with the typical timetable of cluster attacks and immediately before the onset of a bout, suggests a relation between the two disorders. It is unlikely that it was caused by pain, since pain intensity and associated autonomic symptoms would be easily noticed and remembered.
The relation between CH and sleep is complex (4). Sleep is a trigger of CH attacks and attacks disrupt sleep. Melatonin secretion is changed during CH bouts and both sleep deprivation and compounds that consolidate sleep may prevent attacks of pain (4,5). Yet the typical pattern is nocturnal awakening because of pain, not in its anticipation (4,6). There is a single report of a transient insomnia during a CH bout (but not before the bout) that was attributed to fear of the attacks (7). On the other hand, while dissociations between pain and autonomic symptoms have been reported to occur in 3% of CH patients (8), to our knowledge there are no descriptions of cyclic awakenings without pain.
This unusual presentation is relevant for two reasons. Firstly, because it indicates that the sleep-wake dysfunction can be the first manifestation of a bout, thus providing clinical evidence in support of the hypothesis of the hypothalamic generator of CH bouts (not just the attacks). Secondly, because cyclic nocturnal awakening may be a warning sign of a new cluster bout, signaling the need to introduce prophylactic medication.
While systematic prospective studies are necessary to unveil the frequency of this symptom and its predictive value of cluster episodes, it is worth stressing that it may go unnoticed if not specifically sought. In fact, many patients consult their physician only at the middle of cluster episodes, a time when early, nonpainful manifestations might have been forgotten or ignored. Systematic studies of any prodromal symptoms are worthy of being recorded and better studied.
Clinical implications
Cluster headache is an excruciating headache with a periodic recurrence. Periods of pain usually appear without warning, which does not allow for preemptive intervention. This patient experienced two different recurrent nocturnal awakenings without pain for five to seven consecutive nights before the onset of a cluster period. It suggests the existence of warning signs of an impending cluster activity, such as a disruption of the sleep-wake cycle that may be due to a hypothalamic bout generator.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.