
Abstract
Background
The hallmark of migraine aura (MA) is transient cortical dysfunction but it is not known if MA is associated with structural cortical or subcortical changes. To determine the relation between MA and structural gray matter abnormalities, we studied a unique sample of 20 patients with frequent side-locked MA, i.e. visual aura consistently occurring in the same hemifield.
Methods
We applied a highly sensitive within-patient design to assess anatomical differences with both voxel-based morphometry and surface-based morphometry on a whole-hemisphere level and for specific anatomical regions of interest. Within-subject comparisons were made with regard to aura symptoms (N = 20 vs 20) and with regard to headache (N = 13 vs 13).
Results
We found no differences in gray matter structure with regard to aura symptoms in MA patients. Comparing the typical migraine headache side of the patients to the contralateral side revealed a difference in cortical thickness in the inferior frontal gyrus (mean difference 0.12 mm, p = 0.036).
Conclusion
MA per se is associated with abnormal function but not with lateralized abnormalities of gray matter structure. Alteration of the inferior frontal cortex suggests structural reorganization of pain inhibitory circuits in response to the repeated intense nociceptive input due to the headache attacks.
Introduction
Migraine with aura (MA) is characterized by recurrent attacks of visual, sensory, aphasic, or motor symptoms (1). Most commonly, patients experience homonymous visual disturbances (2). These symptoms clearly reflect a transient cortical dysfunction, most likely due to the well-described electrophysiological phenomenon of cortical spreading depression (CSD) (3) characterized by a slowly spreading wave of cortical depolarization followed by suppression of neuronal activity (4).
MA has traditionally been considered a benign disorder without structural changes in the brain. However, recent magnetic resonance imaging (MRI) data suggest that gray matter abnormalities occur in mixed populations of patients with and without aura (5–11); however, not consistently (12,13). The possible relation between aura and cortical structural changes exclusively in patients suffering from MA has not previously been investigated. CSD is known to cause transient neuronal swelling and dendritic changes (14,15) but animal experiments showed no clear-cut evidence that CSD per se might cause cortical or subcortical tissue damage (15,16).
In the present study, we examined the relation of migraine aura and migraine pain to cortical and subcortical structure by investigating a unique sample of patients with frequent visual aura consistently occurring in the same hemifield. Using functional magnetic resonance imagining (fMRI) we previously observed cortical hyperexcitability of symptomatic hemispheres with regard to aura in these individuals (17), and we therefore hypothesized that gray matter structural abnormalities are present in the symptomatic hemispheres of MA patients. We applied a highly sensitive within-patient design to assess differences between symptomatic and asymptomatic hemispheres by both voxel-based morphometry (VBM) and surface-based morphometry (SBM) on a whole-hemisphere level and for specific anatomical regions of interest (ROIs).
Methods
Clinical characteristics of 20 patients with migraine with aura (MA).
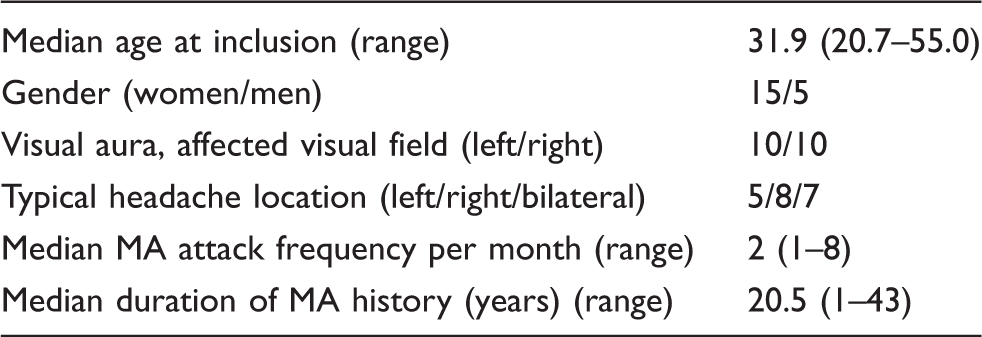
Inclusion criteria were unilateral, homonymous visual aura occurring on the same side (either the left or right hemifield) in 90% of attacks or more with an attack frequency of one attack per month or more. Exclusion criteria were any other type of primary or secondary headache (except for infrequent tension-type headache), serious somatic or psychiatric conditions, or intake of daily medication including prophylactic migraine treatment. A general medical history was taken for all patients and they underwent a complete neurological examination. Before inclusion, patients provided a very detailed description of their aura symptoms.
The median MA attack frequency was two attacks per month (range one to eight attacks/month). All patients experienced visual symptoms. In some patients, visual aura was followed by sensory (N = 11) and aphasic (N = 5) symptoms. Patients reporting more than one aura symptom experienced visual aura in every attack. Some patients (N = 7) reported bilateral headaches. Most, but not all, patients with unilateral headache reported headache contralateral to the side of the aura symptoms (N = 10) as observed in previous studies (19).
The ethics committee of the County of Copenhagen (H-KA-20060083) approved the study, which was undertaken in accordance with the Helsinki Declaration of 1964, as revised in 2008. The study was carried out at Glostrup Hospital, Copenhagen area, Denmark, between April 2011 and February 2012. All subjects gave written informed consent to participate in the study.
MRI procedure
MRI was performed on a 3.0T Philips Intera Achieva scanner (Philips Medical Systems, Best, The Netherlands) using a 32-element phased-array receive head coil. Anatomical images were acquired using a T1-weighted three-dimensional turbo field-echo sequence (170 sagittal slices of 1 mm thickness; in-plane resolution 1 × 1 mm; repetition time 9.9 s; echo time 4.6 ms; and flip angle 81 degrees).
Data analysis
The symptomatic hemispheres (i.e. contralateral to the visual symptoms) of the patients were compared to their contralateral asymptomatic hemispheres. Since right-sided and left-sided symptoms were reported by an equal number of patients, an equal number of right and left symptomatic hemispheres were analyzed.
Thus, any differences between right and left hemispheres (e.g. caused by normal anatomical right/left asymmetry or magnetic field inhomogeneity of the scanner) unrelated to migraine aura would be expected to cancel out in the analysis.
As a secondary endpoint, we compared interhemispheric differences with regard to headache side.
VBM and cortical thickness measurements have been shown to generally provide very consistent results, but cortical thickness estimation may provide a more sensitive measure of cortical changes (20). While cortical thickness is selectively measured using the SBM-based method, VBM provides a mixed measure of gray matter including cortical density, as well as cortical thickness (20). Thus, a combination of these two complementary methods is useful both to detect and specify the underlying gray matter changes.
VBM
Structural data were analyzed with FSL-VBM (http://fsl.fmrib.ox.ac.uk/fsl/fslwiki/FSLVBM) (21), an optimized VBM protocol (22) carried out with FMRIB Software Library (FSL) tools (23). Before the analysis, mirror images of the acquired anatomical data were created for each subject by flipping the images along the x-axis. The brain was extracted using the structural images and gray matter segmentation was performed before the images were registered to the Montreal Neurological Institute (MNI) 152 standard space using non-linear registration. The resulting images, mirrored and original data, were averaged to create a left-right symmetric, study-specific gray matter template. Second, all native gray matter images were non-linearly registered to this study-specific template and “modulated” to correct for local expansion (or contraction) due to the non-linear component of the spatial transformation. The modulated gray matter images were then smoothed with an isotropic Gaussian kernel with a sigma of 3 mm, i.e. approximately full width half maximum (FWHM) of 3 × 2.3 = 6.9 mm. Finally, images in the original orientation were compared to the corresponding mirrored images. This approach of “brain flipping” for hemisphere comparison has been applied in previous studies (22,24). Symptomatic vs asymptomatic hemispheres were compared in a paired fashion by application of voxel-wise general linear model (GLM) using permutation-based non-parametric testing (25), correcting for multiple comparisons across space by threshold-free cluster enhancement (26) (cluster-wise p < 0.05).
SBM
Cortical reconstruction and volumetric segmentation was performed with the FreeSurfer image analysis suite (http://surfer.nmr.mgh.harvard.edu/) (27,28). Using this approach, the gray and white matter surfaces were defined by an automated brain segmentation process. An experienced investigator, who was blinded with respect to the symptomatic hemispheres of the subjects, then manually corrected the automated segmentation. Cortical thickness was estimated at each point across the cortex by calculating the distance between the gray/white matter boundary and the cortical surface. Individual whole brain (right and left hemisphere) surface maps were then registered to a common FreeSurfer template surface pseudo-hemisphere (fsaverage_sym) (29) by the FreeSurfer spherical registration system (30) and smoothed with a 10 mm two-dimensional (2D) Gaussian smoothing kernel (30). Symptomatic and asymptomatic hemispheres were statistically compared in a paired design while applying cluster-wise correction for multiple comparisons using a permutation-based non-parametric analysis (cluster-wise p < 0.05). Additionally, we measured the volume of the thalamus, caudate, putamen, amygdala and hippocampus bilaterally for each subject using FreeSurfer’s automated subcortical segmentation.
ROI analysis
Several ROIs were examined for focal changes of gray matter using both of the methods described above. We investigated the following ROIs parcellated by FreeSurfer: primary visual cortex (V1), secondary visual cortex (V2), visual area V5/MT and somatosensory cortex (SSC, Brodmann areas BA1, BA2, BA3a and BA3b). Furthermore, we examined the following ROIs, which are not available in FreeSurfer, using the FSL version of the Jülich histological atlas (31): visual area V3, visual area V4 and the lateral geniculate nucleus (LGN).
Finally, we specifically checked whether the hyperresponsivity in the symptomatic hemisphere with respect to aura, previously reported for the individuals who also participated in the present study, is directly related to changes of cortical morphology. This was performed for all ROIs for which hyperresponsivity was observed (inferior frontal gyrus, superior parietal lobule and inferior parietal lobule) by correlating the blood-oxygenation level-dependent (BOLD) responses to visual stimulation to the mean cortical density (VBM results) and mean cortical thickness (SBM results) of these areas. Statistical calculations were carried out using R ver. 2.14.1 for Mac OS X. Mean cortical thickness and mean gray matter density for each ROI was compared using paired t tests corrected for multiple comparison using the sequential Bonferroni correction according to Holm (32).
Sensitivity of the analyses
Cortical density and cortical thickness have previously been shown to decrease linearly with age (22,33). In order to assess the sensitivity of the methods used in this study, we investigated the relation of mean whole-brain density and total cortical gray matter volume with subject age. Statistical testing for correlation was applied using Pearson’s product-moment correlation.
Retrospective power analyses were carried out to calculate the minimum difference in cortical thickness that could have been detected at a 5% significance level with 80% power for each of the investigated ROIs.
Results
Results of interhemispheric comparisons of symptomatic versus asymptomatic sides for whole-hemisphere testing and for specific regions of interest (ROIs).

Values are p values corrected for multiple comparisons. SBM: surface-based morphometry; VBM: voxel-based morphometry; V1: primary visual cortex; V2: secondary visual cortex; V3: visual area V3, V4: visual area V4, V5/MT: visual area V5/Middle temporal; LGN: lateral geniculate nucleus; SCC: somatosensory cortex; NA: not applicable.
VBM
Voxel-wise whole-hemispheric comparison of symptomatic versus asymptomatic hemispheres with regard to aura showed no differences. We found no differences of regional gray matter density in any of the examined ROIs. There was no correlation between the functional activation of hyperresponsive ROIs (17) and the mean VBM gray matter density values. Comparing the typical headache side to the non-headache side did not reveal any side-to-side differences for the voxel-wise whole-hemisphere comparison or the ROI based analysis, either.
SBM
We found no differences for the whole-hemisphere or ROI-based comparison of symptomatic and asymptomatic hemispheres with regard to aura. There was no correlation between the functional activation of hyperresponsive ROIs (17) and the cortical thickness of these ROIs.
For the comparison of headache side versus non-headache side (patients with unilateral headache, N = 13), the whole-hemispheric analysis showed a between-hemisphere difference corresponding to an increased cortical thickness in the hemispheres contralateral to the perceived headache side in the pars opercularis of the inferior frontal gyrus (mean between-hemisphere difference 0.12 mm, SD 0.64 mm, cluster-wise p = 0.036, MNI coordinates x, y, z = −46, 17, 21); see Figure 1. No differences were seen for the a priori specified ROIs or for volumes of subcortical structures. A subsidiary analysis comparing left and right hemispheres revealed no differences in frontal cortical thickness. Further, no interhemispheric differences in the volume of thalamus, caudate, putamen, amygdala or hippocampus were found between symptomatic and asymptomatic or between headache and non-headache side.
Results of interhemispheric comparison of headache side (N = 13) versus non-headache side (N = 13). A statistically significant cluster of difference in cortical thickness (non-headache side minus headache side) was found exclusively in the pars opercularis of the inferior frontal gyrus. The non-headache side (contralateral hemisphere to the perceived pain side) was found to be thicker than the headache side (mean between-hemisphere difference 0.12 mm, SD 0.64 mm, cluster-wise P = 0.036, MNI coordinates x, y, z = −46, 17, 21).
An additional, exploratory analysis showed a correlation between the difference in cortical thickness of the pars opercularis ROI between the pain and non-pain sides in patients with unilateral headache and the attack frequency (n = 13, Pearson’s product-moment correlation, p = 0.005). We did not find a correlation between the mean (left and right) cortical thickness of this ROI and the attack frequency (N = 20, Pearson’s product-moment correlation, p = 0.32).
Further, comparing the mean cortical thickness of the ROI between patients with unilateral versus patients with bilateral headaches did not show any difference (N = 13 vs. 7, two-sample t test, p = 0.87). Additional whole-brain comparisons of patients with unilateral versus bilateral headache (VBM and SBM) also did not reveal any structural differences.
Sensitivity of the analyses
The minimum differences in cortical thickness that could have been detected in this study for the specific ROIs were: V1: 0.07 mm, V2: 0.05 mm, V3: 0.10 mm, V4: 0.17 mm, V5/MT: 0.11 mm, SSC: 0.10 mm. Accordingly, we found significant correlations between age and whole-brain gray matter density (VBM, p < 0.01) and between age and whole-brain cortical volume (SBM, p = 0.01).
Discussion
Using a highly sensitive design and validated automatic analysis methods, we found that side-fixed aura is not associated with gray matter abnormalities in MA patients. Comparing the typical migraine headache side of the patients to the contralateral side revealed a difference in cortical thickness in the inferior frontal gyrus but no differences in gray matter density.
Previous studies using only VBM have compared structural MRI data of mixed groups of migraine patients with and without aura to healthy controls (6,8–12). Results are somewhat conflicting, but overall suggest decreases in gray matter density in frontal and cingulate cortex of migraine patients. To our knowledge, there are no reports of VBM abnormalities in MA specifically.
In a previous study increased cortical thickness in the visual areas V3a and MT+ (0.14 mm and 0.24 mm, respectively) was found in MA patients compared to healthy controls, but not compared to patients with migraine without aura (5). A study by the same group reported thickening of the somatosensory cortex in a mixed group of migraine patients (with and without aura) compared to controls (7). Datta et al. found no differences in cortical thickness between groups in a large sample of migraine patients with and without aura and matched controls (13). In the present study we found a difference in cortical thickness of the inferior frontal gyrus related to migraine pain processing (in patients with unilateral headache, N = 13) but no differences related to MA. Whether this difference indicates a thickening of the hemisphere contralateral to the pain or a thinning of ipsilateral hemisphere is unknown. In addition, the magnitude of this interhemispheric difference is positively correlated with the attack frequency. Interestingly, a study of patients with unilateral facial pain specifically reported decreased density of the inferior frontal gyrus ipsilateral to the pain side (34). The inferior frontal gyrus is part of the central pain processing network (35) and probably contributes to pain modulation/inhibition (36). Altogether, the alteration of the inferior frontal cortex observed in the present study could indicate structural reorganization of pain inhibitory circuits in response to the repeated intense nociceptive input due to the headache attacks. It needs to be further elucidated whether such structural neuroplasticity is physiological and favorable in terms of migraine outcomes or whether it is actually perpetuating the clinical signs and symptoms of migraine.
We recently conducted an fMRI study on the same group of MA patients as in the current study with a visual stimulation paradigm and observed a hyper-responsiveness of an advanced visual processing network presenting only in the symptomatic aura hemispheres (17). Another recent study found increased responses in the primary visual cortex and the LGN in interictal MA (37). The results of the present study suggest that, despite increased cortical responsiveness, aura per se is not associated with lateralized structural abnormalities in the cortex.
The main objective of the present study was to investigate whether cerebral cortex that produces migraine aura symptoms is structurally different from non-aura-producing cortex. We addressed this by direct comparison of hemispheres within subjects, thus avoiding variability due to subject-specific parameters such as age and gender. It is well known that the right and left hemispheres are structurally asymmetric (38). To control for this, we included the same number of patients with right-sided and left-sided symptoms. This was also balanced within each gender group (females: eight left, seven right; males: three left, two right). While we found no structural differences directly related to the presence of aura, it is still possible that the condition of MA is associated with structural changes on a whole-brain level. Studies using SBM are conflicting with regard to this matter, and VBM has not been applied to studying MA specifically. Future studies comparing patients with MA to patients without aura and to healthy controls and applying both SBM and VBM techniques are therefore warranted.
In conclusion, while MA is associated with ictal and interictal cortical dysfunction, we found no abnormalities of cortical or subcortical gray matter structure related to aura. In contrast, a difference in cortical thickness related to migraine headache lateralization was found in a frontal brain area potentially contributing to pain inhibition.
Clinical implications
Migraine aura, although associated with cortical dysfunction, does not cause and is not caused by lateralized structural gray matter abnormalities. The repeated intense nociceptive input of migraine headache possibly causes structural reorganization of cortical pain inhibitory circuits.
Conflict of interest
Drs Hougaard, Amin, Hoffmann, Larsson and Magon have nothing to declare.
Dr Sprenger has consulted for ATI, Novartis, Eli Lilly, Allergan, Mitsubishi Pharma, Genzyme and Biogen Idec. He has received reimbursement for travel expenses or lectures from Janssen, Pfizer, Bayer Schering, Eli Lilly and Biogen.
Dr Ashina has received unrestricted grant support from Merck and ATI and he is a consultant and/or scientific adviser for ATI, Allergan, Amgen and Alder.
Footnotes
Funding
The work was supported by the University of Copenhagen, the Lundbeck Foundation Center for Neurovascular Signalling (LUCENS), the Danish Council for Independent Research-Medical Sciences (FSS) (grant 271-08-0446), the Novo Nordisk Foundation (grant R172-A14333) and the Research Foundation of the Capital Region of Denmark.
Acknowledgments
The authors thank all participating patients. We would also like to thank Dr Egill Rostrup for advice regarding data analyses, radiologist Vibeke Andreé Larsen for reviewing MRI images, and radiographers Bente S Møller, Marjut Lindhardt, and Helle J Simonsen for helping with scans.