
Abstract
Aim
The impact of early degenerative changes of the cervical spine on pain in adulthood is unknown. The objective was to determine whether degeneration in adolescence predicts headache or neck pain in young adulthood.
Methods
As part of a follow-up of schoolchildren with and without headache, 17-year-old adolescents with headache at least three times a month (N = 47) and adolescents with no headache (N = 22) participated in a magnetic resonance imaging (MRI) study of the cervical spine. The same adolescents were re-examined by phone interview at the age of 22 years (N = 60/69, 87%).
Results
Mild disc degeneration at the age of 17 years was common, but was not associated with either frequent or intensive headache or neck pain at the age of 22 years.
Conclusion: Mild degenerative changes of the cervical spine in 17-year-old adolescents cannot be regarded as a cause of future headache or neck pain.
Introduction
Degeneration of the cervical spine is common in healthy adults and also in adolescence (1–3). It is not known if early degenerative changes of the cervical spine lead to pain in adult years as has been shown in subjects with early degeneration of the lumbar spine (4). In few follow-up studies of healthy adults, the association between degeneration and pain has not been clear. In a 10-year magnetic resonance imaging (MRI) follow-up study of 223 healthy adults, degeneration of the cervical spine progressed in 85% of participants. In the follow-up phase, the progression of disc space narrowing was associated with the incidence of stiff shoulders, while decrease in the signal intensity of the intervertebral disc was more common in painless participants when compared with those with incident neck pain (1). In another 10-year X-ray follow-up study of healthy adults, only baseline disc degeneration at level C6/7 was shown to predict the incidence of neck pain (5).
In our previous cross-sectional study on the same study population of schoolchildren, headache was associated with muscle pain, but not with dysfunction of the upper neck (6). Mild degenerative changes of the cervical spine were found in 67% of participants at the age of 17 years, with no difference between adolescents with and without headache (2).
The purpose of the present study was to determine whether disc degeneration of the cervical spine in adolescence predicts headache or neck pain 5 years later in young adults. The hypothesis was that early degeneration leads to pain in forthcoming years.
Methods
Sample
The present study is part of a population-based follow-up study of headache in schoolchildren. A flow chart shows the participation rates of all study phases (Figure 1). The original source population covered all 12-year-old schoolchildren in the city of Turku (total population of 170,931, year 1998) in south-western Finland (7). The details of the study design have been published previously (2,6–8).
Flow chart of the study population. HA: headache; NP: neck pain.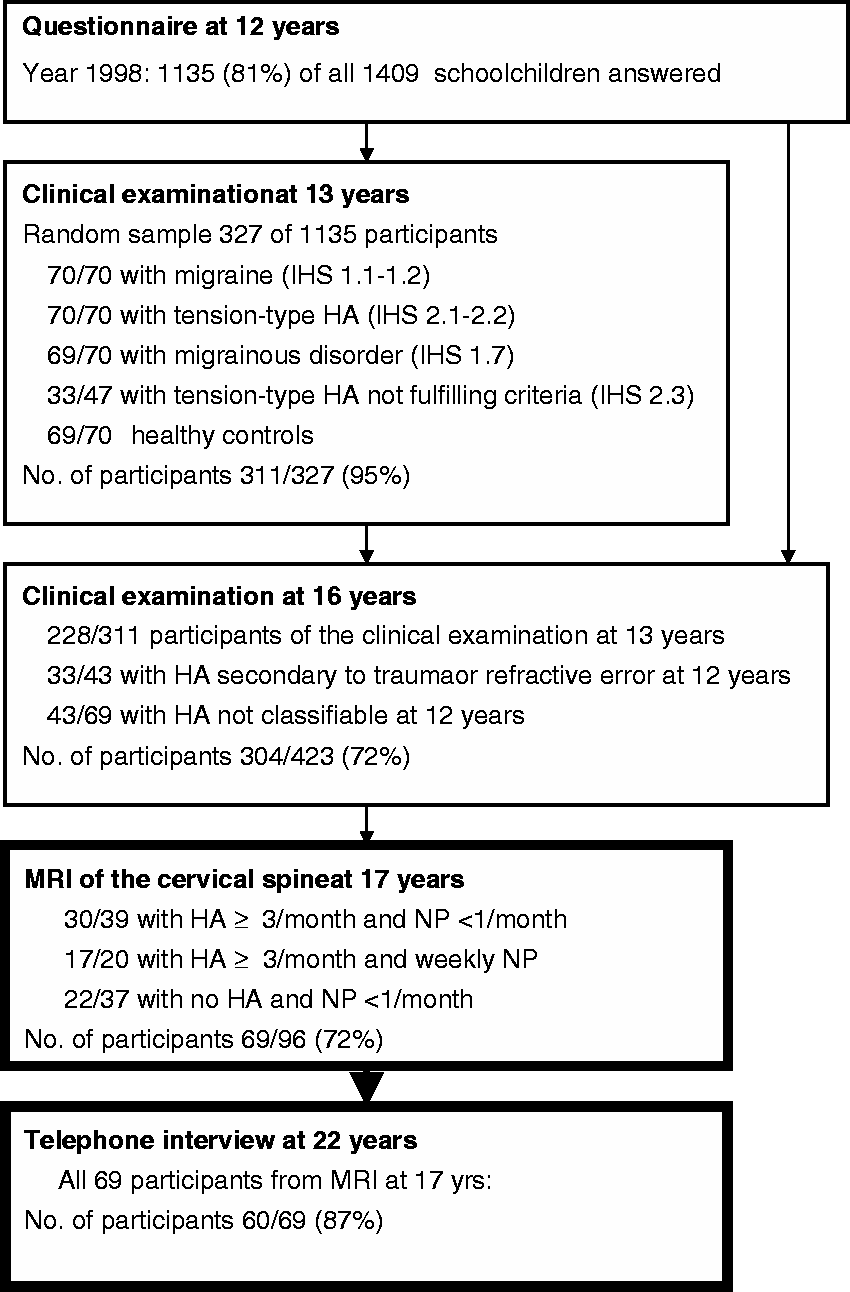
Adolescents with headache at least three times a month (N = 47/59, 80%) and adolescents with no headache (N = 22/37, 59%) attended MRI of the cervical spine at the age of 17 years. Of headache sufferers, those with weekly neck pain (N = 17) or with infrequent (0 or <1/month) neck pain (N = 30) were chosen to attend MRI. Of adolescents with no headache, only those with infrequent neck pain (0 or <1/month, N = 22) were invited to MRI (2).
After 5 years, at the age of 22 years, the same adolescents from MRI study were interviewed by phone using a structured questionnaire (N = 60/69, participation rate 87%). The interviewer was blind to the participants’ pain histories and to the findings of cervical MRI. Even if participation rates were high in all study phases, the final study population from 17 to 22 years of age may be biased if compared with the whole population of 12-year-old schoolchildren.
Outcome variables
In the clinical examination at the age of 16 years and in the telephone interview at the age of 22 years, headache frequency and neck pain frequency were defined as the monthly number of headache or neck pain episodes during the preceding 6 months (response options no, <1/month, monthly: x times/month). The average intensity of headache and the intensity of neck pain in the preceding 6 months were evaluated using the numerical scale (0–10, 0 = no pain, 10 = maximal intensity of pain). The associations of predictive disc degeneration with headache and neck pain frequency and intensity at the age of 22 years in different subgroups and also associations with persistent pain from adolescence to adulthood were analyzed (Figure 2). The small number of participants with changing headache or neck pain frequency did not enable the comparison of initially pain-free participants with those with incident pain, or the comparison of participants with persistent frequent pain with those with improving pain (Table 1).
Analyzed associations of DD-variables at 17 years as predictive factors. MRI: magnetic resonance imaging of the cervical spine; DD: disc degeneration; HA: headache; NP: neck pain; mo: month. Changes in the frequency of headache (HA) and neck pain (NP) from 16 to 22 years of age. Monthly rate of pain episodes. Headache. Neck pain.

Predictive factors in magnetic resonance imaging
The details of the MRI study at the age of 17 years have been published previously (2). In summary, the cervical spine was imaged using 1.5-T imaging system (Symphony; Siemens, Erlangen, Germany). All scans were interpreted independently by three neuroradiologists blinded to the participants’ pain histories. Localization of disc degeneration (DD) was analyzed in three ways: first, the occurrence of DD in the whole imaging area from C2 to Th4; second, the occurrence of DD in the upper neck (levels C2/3 and C3/4); third, the occurrence of DD in the lower neck (from C4/5 to C6/7).
In our cross-sectional study of MRI participants at the age of 17 years (2), 67% had DD (a decrease in disc signal intensity) at least at one level. DD was mainly mild and most commonly at level C5/6 (46% of participants). Annular tears were found in three, mild foraminal stenosis in two and disc bulgings in 20 participants without significant differences at the age of 17 years between headache sufferers and headache-free controls or between headache sufferers with and without neck pain (2).
In the present follow-up study, the occurrence of DD (no/yes), DD of the upper neck (no/yes), DD of the lower neck (no/yes) and disc bulgings (no/yes) at the age of 17 years were analyzed as predictive factors of future pain and of persistence of pain. Although these degeneration factors are highly dependent of each other, this division of cervical degeneration was used to detect possible differences between the upper and the lower neck and between mild degeneration and a possible compression of the nerve, which may occur in disc bulging.
Statistical analysis
Descriptive values were expressed as medians and interquartile ranges (IQR), or frequencies and percentages. Because of skewed distributions, nonparametric tests were used. Figure 2 shows the factors of univariate analysis with DD variables at 17 years of age being predictive factors. Univariate associations between categorical predictive DD variables at the age of 17 years and outcome pain variables at the age of 22 years were evaluated using the Mann–Whitney U-test. Univariate associations were first analyzed for both genders together, then separately for boys and girls. Univariate associations between predictive DD variables and outcome pain variables were also analyzed separately for those with frequent headache (3–30/month), for those without headache, for those with ‘frequent headache and weekly neck pain’ and for those with infrequent neck pain in adolescence. Univariate associations between DD and the outcome of headache (persistent frequent headache compared with no headache from adolescence to young adulthood) and between DD and the outcome of neck pain (persistent weekly neck pain compared with persistent infrequent neck pain from adolescence to adulthood), were evaluated using chi-square and Fisher’s exact test when appropriate. A p value <0.05 was considered to be statistically significant. All p values were calculated with two-sided tests, and no adjustments were made for multiplicity. Statistical computations were done using the SAS System for Windows, release 8.02 (SAS Institute, Cary, NC, USA).
Ethics
The study design and the informed consent procedures were approved by the joint ethics review committee of the Turku University Medical Faculty and the Turku University Central Hospital in all phases of the study. This follow-up study at the age of 22 years was approved 15 January 2008 (record number 145/2007).
Results
Table 1 shows the changes of headache and neck pain frequency from adolescence to adulthood, when adolescents with frequent headache and without headache were compared. Although headache frequency decreased in many with frequent headache, headache continued to occur in all headache sufferers also at the age of 22 years. Of headache-free adolescents, 60% reported having incident headache in the follow-up phase. Eighty-six per cent of adolescents with headache and weekly neck pain still had weekly neck pain 5 years later, and in 61% of those with infrequent neck pain, neck pain remained infrequent also in the follow-up phase.
Degeneration of the cervical spine at the age of 17 years and future pain
Association of adolescent disc degeneration and adult pain.

values evaluated by the Mann–Whitney U-test.
values were calculated without adjustment for multiplicity.
mo: month.
p < 0.01.
p < 0.05.
Disc degeneration and adult pain in participants with frequent headache in adolescence.

p values evaluated by the Mann–Whitney U-test.
p values were calculated without adjustment for multiplicity.
Frequent HA = 3–30/mo.
mo: month.
p < 0.05.
In women, all degenerative predictive factors were associated with low neck pain frequency at the age of 22 years. There was a trend of DD associating with less frequent future neck pain also in participants with baseline frequent headache and weekly neck pain (p = 0.08) and in the incidence of neck pain (p = 0.05). When participants with persistent weekly neck pain were compared with those with persistent infrequent neck pain (both in adolescence and in adulthood), DD of the lower cervical spine was associated with persistent infrequent neck pain. No other significant associations were found between DD or disc bulging with analyzed outcome factors.
Discussion
Contrary to our hypothesis, adolescent disc degeneration (DD) or disc bulging of the cervical spine were not predictive of future frequent or intensive headache or neck pain. Surprisingly, adolescents with degenerative changes of the cervical spine reported neck pain less often after 5 years than those without degeneration. To our knowledge, this is the first follow-up study of the predictive value of adolescent cervical DD on adult headache or concurrent neck pain. Early degenerative changes of the lumbar spine have been suggested to cause back pain in adult years (4), and DD at level C6/7 has been associated to future neck pain in asymptomatic adults (5). On the other hand, our results are in line with a recent follow-up study of healthy adults, where the progression of mild disc degeneration was associated with the persistence of asymptomatic period when compared with the incidence of neck pain (1).
Provided that headache can be caused by degeneration in the cervical spine, the convergence between the trigeminal afferents and the upper three cervical nerves suggests that degenerative changes in the upper neck may more likely cause headache than degeneration in the lower cervical spine (9). In our study population, DD was more common in the lower part of the cervical spine, but mild DD of the upper neck (levels C2/C3 and C3/4) was not a predictor of future frequent or intensive headache either.
Our results are novel and need confirmation. Even if our results are in line with a follow-up study of healthy adults (5) and disc degeneration did not predict increasing pain, this is only the first study of the influence of adolescent disc degeneration on adult headache and neck pain and the power of our study is not sufficient to make definite conclusions. An open question is how DD might be a protective factor of neck pain. It is possible that in the future studies of the adolescent cervical spine, our finding of the association of cervical DD with favourable outcome of neck pain will not be confirmed and DD is not associated with future headache or future neck pain as a predictor or as a protecting factor. However, the spine undergoes continuous changes as a response to physiological axial loads (10). The high prevalence of cervical DD in recent MRI studies of young study populations (2,3) could be a consequence of changed requirements of adolescent cervical spine mobility. The cervical spine of adolescents is more flexible than that of adults (11) allowing extreme spinal movements and thus inducing excessive loading of the spine and muscles. This load may subsequently irritate the muscle-nerve system of the neck and lead to pain in sedentary hobbies (12,13). It has been thought that the large extent of motion and high joint loads of the spine, on the other hand, could lead to degeneration (14,15). Therefore, it is possible that degeneration progressing later in adult life could even prevent pain by inhibiting excessive motions, but mild degeneration of the cervical spine, as in our study population of adolescents, has rather been associated with segmental instability, not with a restrictive effect on the range of motion (16). In agreement with the previous findings in adults (1,14,16,17–19), degenerative changes in our study population were most common at level C5/6 (2), where the extension-flexion motion is considerable (14,15,20) and where also high joint loads are possible during muscle work (21).
In our study population DD was not associated with headache at the age of 17 years (2) nor was predicting more unfavourable prognosis of headache in young adults. In interpreting the relation of DD and neck pain in our study population, it is important to note that we did not study neck pain per se, but neck pain coexisting with headache. However, our results of neck pain are in agreement with adult neck pain studies, which failed to show any clear association between self-reported neck pain and DD (1,3,22,23). Foraminal stenosis of the lower cervical spine has been associated with neck pain (1,24), but in our study on the general adolescent population, degeneration of the spine was mild and caused no significant stenosis.
Headache frequency, not headache type was chosen as an inclusion criterion for MRI (2), because the fluctuation of headache type is common in this age group (25–27) and in adults, the type of headache has not been associated with the radiological changes of the cervical spine (28,29). In a telephone interview at the age of 22 years, excluding all confounding factors such as head injuries was not possible. Our results in the population of schoolchildren cannot directly be applied to patients suffering from chronic headache. As only a minority of headache sufferers ever consult a doctor for their headache symptoms (30,31), it is important to separate the risk factors of neck pain and headache from risk factors for seeking medical advice using a population-based approach as in our study.
Conclusion
Mild degenerative changes of the cervical spine in adolescents cannot be regarded as a cause of future headache or neck pain in young adults.
Funding
This study was supported by grants from the city of Turku, University of Turku and University Hospital of Turku.
Conflict of interest
None declared.
Clinical implications
Impact of early degenerative changes of the cervical spine on pain in adulthood is unknown. In our cohort study of schoolchildren, mild disc degeneration in adolescence was common, but was not associated with either frequent or intensive headache or neck pain in adulthood. Mild degenerative changes of the cervical spine in adolescents cannot be regarded as a cause of future headache or neck pain.
Footnotes
Acknowledgements
Appreciation is expressed to Olli Kaleva BSc for skilful computation of the data, and to Mrs Inger Vaihinen for her versatile assistance.