
Abstract
Headaches and neck pain are reported to be among the most prevalent musculoskeletal complaints in the general population. A significant body of research has reported a high prevalence of headaches and neck pain among adolescents. Sitting for lengthy periods in fixed postures such as at computer terminals may result in adolescent neck pain and headaches. The aim of this paper was to report the association between computer use (exposure) and headaches and neck pain (outcome) among adolescent school students in a developing country. A cross-sectional study was conducted and comprehensive description of the data collection instrument was used to collect the data from 1073 high-school students. Headaches were associated with high psychosocial scores and were more common among girls. We found a concerning association between neck pain and high hours of computing for school students, and have confirmed the need to educate new computer users (school students) about appropriate ergonomics and postural health.
Introduction
Headaches and neck pain are amongst the most prevalent musculoskeletal complaints in the general population and are considered to be a significant public health concern (1–3). A significant body of research has reported a high prevalence of headaches and neck pain among adolescents over the previous decade (4–6). There is also convincing research that regular adolescent headaches and neck pain are a primary predictor of chronic pain in adulthood (7, 8). The point prevalence of neck pain among adolescents is reported to range between 20 and 60% across developed and developing countries (9–15). Furthermore, it is estimated that about 5% of early to mid adolescents with neck pain experienced persistent neck pain over the next 4 years, supporting the consistency and longevity of this condition once it has become established (8, 9, 16).
Sedentary lifestyles and lengthy periods spent in fixed postures, such as at computer terminals, may result in adolescent neck pain and headaches (17). Since information and communication technology are becoming an integral component of formal school education, it is thus plausible that neck pain and headache could become more prevalent. In South Africa, computers are used in schools because of Government incentives to boost careers in science and technology as well as to address the increasing shortage of science and mathematics teachers in schools (18, 19). Adolescents using computers daily during school activities may become chronic headache and neck pain sufferers, with resultant negative impacts on adolescents’ tertiary education and work participation in adulthood.
Preventative initiatives should be based on sound understanding of the aetiology of neck pain and headaches (20). Although computer use is an increasingly reported risk factor in the literature, the aetiology of headaches and neck pain is usually multidimensional, and the complex interplay between causal relationships and risk factor mechanisms is not yet well understood (20–25). The furniture and computer equipment may be a contributing factor in the development of musculoskeletal pain among adolescents, as these will influence the postures assumed by students at the computer workstation (26). Prolonged stress and strain placed on the musculoskeletal structures may explain the high prevalence of musculoskeletal pain among computer users (27).
In addition to computer usage, other significant risk factors for adolescent musculoskeletal pain include increased age, female gender, family history of back pain (28), smoking (29), involvement in competitive sports (30) and psychosocial factors (9, 31). Although the prevalence of headaches and neck pain among adolescent computer users has been established (22, 23, 29, 32), only a few studies have reported on associations between computer usage and headaches and cervical pain among adolescents (21, 24). This study thus adds to the body of knowledge by reporting on the association between computer use (exposure) and headaches and neck pain (outcome) among adolescent school students in a developing country, where information and communication technology is implemented for curriculum delivery in schools.
Methodology
Ethics
This study obtained ethical approval from the Committee of Human Research at Stellenbosch University.
Sample selection
Sample size calculations using Statistica Version 7 indicated that 1600 students would be required in order to identify a minimum spinal pain prevalence of 40% (33) with 80% power, α 5% in an older adolescent population.
Students in grades 10–12 (aged 14–18 years) who attended high schools in the Western Cape metropolitan region of South Africa were eligible to participate. These schools may or may not have offered computer studies or compu-typing training to their students, and students at these schools may or may not have chosen to undertake computer studies. This provided a range of potential exposures to computer activities for analysis. To be eligible, schools should have a minimum of 80 students in each of grades 10–12 (at least 240 students in these three learner grades). A list of eligible schools (n = 124) was constructed in clusters of four educational regions (called Education Management and Development Centres), and two schools were randomly selected from each region in order to provide the required sample size (total eight schools, minimum sample size 1920 students). Schools were coded regarding whether or not they offered computer studies.
Brief description of the Computer Usage Questionnaire
A comprehensive description of the data collection instrument, the Computer Usage Questionnaire (CUQ), has been published elsewhere (34). It was developed and tested based on sound psychometric principles [with items based on available literature and validated by an expert reference group and a sample of students (end users)]. Test–retest reliability was assessed and the responses were found to be stable over a 1-week period. Students did not report any difficulty when responding to any questions.
For the purpose of the analysis reported in this study, data were extracted from the CUQ on the age and gender of students, computer-teaching status of schools, learner's computer use (cumulative hours of use in school and elsewhere), reports in the past month of headache and neck pain (considered separately and together), amount of time spent in sports activities and psychosocial factors.
Survey process
The CUQ was administered to the study sample between February and May 2006. The principal researcher and an assistant, who were both physiotherapists, collected the data. On the day of data collection at the schools, a short explanation and procedure were provided before administration of the questionnaire. Students were given 20 min to complete the questionnaire.
Hypothesis
The hypothesis underpinning testing reported in this paper was that high levels of computer use by school students would be strongly associated with neck pain and headaches. Age group, gender, computer-teaching status of school, amount of sport played and psychosocial factors were considered as potential confounders.
Symptoms
Neck pain or headaches occurring in the past month were identified by students on a body chart. These data were treated for analysis purposes as headache (or not), neck pain (or not), or headache and neck pain occurring concurrently. Where neck pain or headache was reported, students had the opportunity to specify severity in binary form (slight discomfort, or a lot of discomfort). An index of pain experience was calculated by scoring headache and neck pain events and multiplying this by the severity score.
Exposures
Data management procedures were undertaken to develop exposure values.
Primary exposure: Computer use was calculated as total hours spent per week using school computers and computers elsewhere (home, internet café, library, friends’ houses, etc.). School computer use was recorded by students in the CUQ in categories of ‘about 2 h per week’, ‘about 4 h per week’, ‘about 6 h per week’ or ‘about 8 h per week’. Hours of computer use elsewhere was derived from multiplying the answers to two questions:
‘On average, how many times per week do you use the computer (less than once per week, twice through to 5 times per week)’, and
‘On average, how many hours per day do you spend working on the computer outside school (less than 30 min, one hour through to 4 h or more)’.
The data were split at the median value of the total number of hours of computer use for analysis purposes (high use, low use).
Potential confounders
Psychosocial factors were measured by eight questions derived from Goodman et al. (35), comprising:
‘Do you care about other people and try to be nice to them? (reverse scoring)
‘Do you get a lot of headaches and stomach aches?’
‘Do you get very angry and lose your temper?’
‘Do you feel sad and tearful?’
‘Do you fight a lot?’
‘Do you feel nervous when meeting new people and going to new places?’
‘Do you get scared easily?’
‘Do you make new friends easily?’ (reverse scoring)
Responses to questions 2–7 were scored 3 (always), 2 (sometimes) or 1 (never), and questions 1 and 8 were scored similarly, but in reverse order. A total score was derived for psychosocial behaviour for each learner. For analysis purposes this score was divided at the median value (poor and good psychosocial behaviours).
Sport participation was calculated as the total number of hours playing sport per week, which was collected in categories of < 1 h, about 2 h, about 4 h and ≥ 6 h. Sports participation was categorized at the median value for analysis purposes as ≤ 2 h/week, 4 h or more.
Age was considered in two categories (14–16 years and 17–18 years). This approach was taken because in some literature, young people aged > 16 years are classified as adults because of their role in the workplace (36–38).
Data analysis
Data were entered into a purpose-built MSExcel file, and analysis was conducted using SAS Version 8.2 (SAS Inc., Cary, NC, USA). Crude associations between the primary exposure (computer use) and symptoms (headache, neck pain, and both symptoms together) were expressed as odds ratios (ORs) [95% confidence intervals (CIs)].
The univariate confounding influence of gender, age group, computer-teaching school or not, high levels of sports participation and poor psychosocial scores was tested using logistic regression models, which adjusted the crude association between computer use and symptoms and established the importance of each potential confounder. The variables with strong associations were then added in a stepwise manner (strongest predictor, followed by weaker predictors) in a multivariate predictive model of symptoms associated with high hours of computer use.
Results
Sample
The sample consisted of 1073 students, of whom 64.9% were girls [mean age 16.3 years (
Symptoms
Overall 26% students reported suffering headaches in the previous month, with girls reporting twice as many headaches as boys (30.3% compared with 16.1%). Of headache sufferers, 33.4% reported headache of a severe nature. Neck pain was reported by approximately 20% of students overall, with girls and boys suffering similarly (19.6% compared with 20.1%). Severe pain was reported by 12.3% students who suffered neck pain. A much smaller group of girls and boys reported suffering both headaches and neck pain in the previous month (7.1% overall, 7.7% girls, 5.9% boys). Of this group, 40% reported serious pain in either head or neck.
Computing exposure
The median computing exposure (considering school computer use, and computer use elsewhere) was 8.5 h/week (range 0–28 h/week). As expected from these figures, not every learner had regular access to a computer, with 52.3% students attending schools that did not offer computer training. Of these non-computing school students, only 5.5% used computers for > 8.5 h/week. This usage occurred in other places than school. Of the students whose schools offered computer training, 43% used computers for > 8.5 h/week. This usage occurred in school and elsewhere.
Computer use and neck pain
Figure 1 illustrates computer use and percentage of children with neck pain in each of the computer use categories.

Weekly hours of computer use and neck pain (n = 211).
Other potential associates
The mean score for the psychosocial factors was 13.6 (
Headache predictors
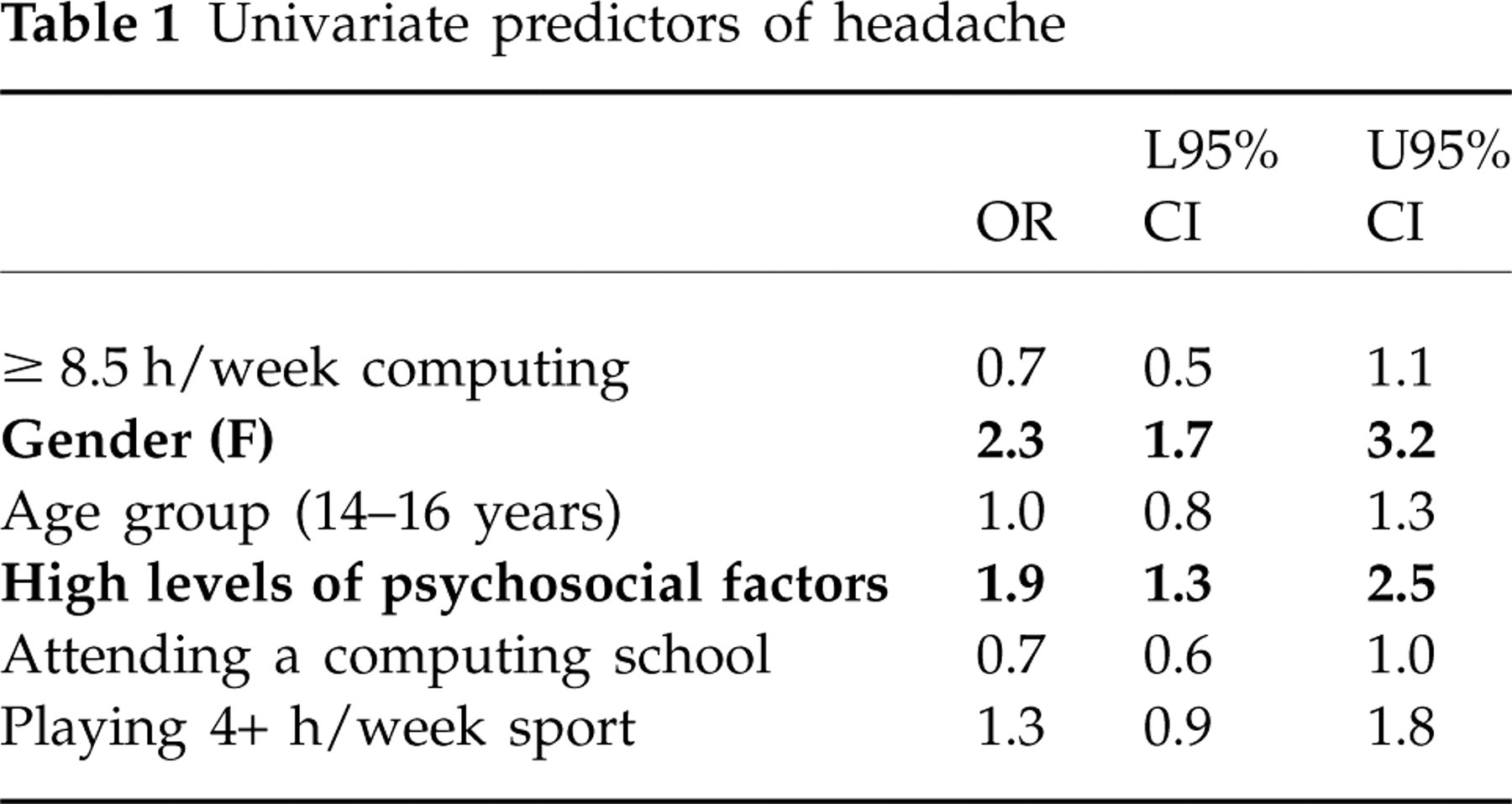
High hours of computer use were not significantly associated with headache. Girls were twice as likely as boys to suffer headache, and young people with high (poor) psychosocial scores were nearly twice as likely to suffer from headaches as young people with low scores. Age group, sporting activity or attending a computer-training school were not associated with headache. The ORs and 95% CI for the crude univariate predictors are reported in Table 1, with the significant associations in bold.
Univariate predictors of headache
There was a significant reduction in the variance of the model associating headaches and computing use when gender was added (significant change in the likelihood ratio P < 0.05), although the adjusted OR remained non-significant (AOR 0.9, 95% CI 0.6, 1.2). This suggested that gender could be important in the model in some capacity. There was a similar effect of high psychosocial scores on the association between headache and computing use (significant change in the likelihood ratio P < 0.05), although again the adjusted OR was non-significant (AOR 0.8, 95% CI 0.6, 1.1). By adding gender and psychosocial factors to a multivariate predictive model of high computing hours and headaches, no further significant adjustment of the association was found (AOR 0.9, 95% CI 0.6, 1.3).
Neck pain
High hours of computer use were the only factor associated with neck pain. This finding supported the hypothesis underpinning this research. No potential confounders were identified during univariate testing. The crude ORs and 95% CI are reported in Table 2.
Univariate predictors of neck pain

Headache and neck pain
There were no significant predictors of combined headaches and neck pain events. Whatever the predictors were of these two events occurring together, they had not been measured in this study. The crude ORs are reported in Table 3.
Univariate predictors of headache and neck pain occurring together

Discussion
This study reports a concerning association between neck pain and high hours of computing for a sample of South African school students. The factors associated with neck pain due to computer usage may be divided into two categories, namely ergonomics and education on both posture and computer habits (24, 26, 39). The posture assumed by students at computer workstations may be influenced by the equipment and furniture as well as by their own posture, muscle strength and inert habits (26, 40). In order to address the high prevalence of neck pain related to computer use, school computer laboratories should be assessed to determine whether the design and lay-out of these computer laboratories adhere to standard ergonomic guidelines.
The position of the computer pointing device, computer screen and keyboard placement may also influence the assumption of poor posture by school students (41, 42). The lack of best practice for placement of these items has meant that for many students the trapezius and levator scapulae muscles may have been placed in a shortened position (due to an elevated shoulder position) (41). In this position, overactivity of the muscles is required to enable use of the keyboard and pointing device on the computer desk (40). Overactivity of the cervical muscles has also been linked to pain, as the cumulative effect will lead to the development of muscle soreness and neck pain. Unnatural positions of the neck and upper thoracic spine may also affect the position and mobility of neural structures such as peripheral nerves and plexus (43, 44). In such instances, neural factors may contribute to the experience of neck pain.
Optimal length of computing sessions also needs to be considered to reduce the prevalence of neck pain. It is estimated that a school computer session in South Africa lasts at least 40 min (34). Biomechanical phenomena such as creep may explain why micro lengthening of the posterior cervical structures occurs in response to prolonged submaximal stretching of tissues (45, 46). The cumulative stretching effect may lead to micro breakdown of tissue structures and, in response, the muscles surrounding the cervical spine such as the trapezius may develop chronic muscle spasm (27, 46). The maintenance of extreme cervical angles for a period of time may cause asymmetrical loading on cervical joints, displacing the cervical spine from its normal lordotic neutral alignment (27, 47). This abnormal biomechanical loading of the skeletal cervical joint structures may further explain the development of pain (27, 47). Therefore, to prevent cervical dysfunction and discomfort, efforts should be made to investigate the use of adjustable furniture and computer equipment in school laboratories to fit the majority of students in computing classes. Furthermore, research into spinal health education and computing habits of school students is encouraged. The application of spinal health education should extend beyond the school setting, as students should be able to apply the basic principles of safe computing use in any setting.
The findings have also illustrated that young people appear to suffer considerably from headaches with or without neck pain. Headaches may be due to a variety of causes, ranging from physiological to biomechanical (20, 48, 49). A strong association between girls and headache has been illustrated in this study. This phenomenon may be influenced by the large sample of girls in this study, but also concurs with the findings from published reports on the prevalence of headaches and girls in developing countries (50). The underlying reasons for headaches among girls in developed and developing countries may be the same, as headaches tend to increase among girls around puberty. This phenomenon may be attributed to the effect of oestrogens in headache pathogenesis (51). A limitation of the current study is that we have not established the type of headache, which therefore limits understanding of these study findings.
The study findings indicate an association between high psychosocial scores and headaches. Findings from published reports indicate that adolescents who experience headaches demonstrate higher levels of stress, fatigue and depression compared with adolescents who have never had headaches (52). The high prevalence of traumatic events among adolescent South Africans may explain the relationship between headaches and psychosocial factors (53). Girls have also reported higher levels of negative psychosocial factors, which may further explain the high prevalence of headaches among girls in this sample (54). However, the term psychosocial is broad and encapsulates aspects of social and psychological behaviour (20). The measurement of psychosocial factors in this study did not fully explore all aspects of psychosocial factors, and valid psychosocial measurement tools should be incorporated in follow-up studies to enhance understanding of the interplay between psychosocial factors and headaches among adolescent computer users.
Conclusion
The findings of this study illustrates that neck pain is associated with computer usage, and in this study sample, high hours of computer exposure was the only predictor of neck pain. Cohort studies may provide further insight into the causation of neck pain among adolescent computer users. Although further information is required to improve our understanding of headaches and neck pain among computer users, proactive preventative strategies should also be developed and evaluated.