
Abstract
The objective of the study was to determine whether adolescents with headache have more disc degeneration in the cervical spine than headache-free controls. This study is part of a population-based follow-up study of adolescents with and without headache. At the age of 17 years, adolescents with headache at least three times a month (N = 47) and adolescents with no headache (N = 22) participated in a magnetic resonance imaging (MRI) study of the cervical spine. Of the 47 headache sufferers, 17 also had weekly neck pain and 30 had neck pain less than once a month. MRI scans were interpreted independently by three neuroradiologists. Disc degeneration was found in 67% of participants, with no difference between adolescents with and without headache. Most of the degenerative changes were located in the lower cervical spine. In adolescence, mild degenerative changes of the cervical spine are surprisingly common but do not contribute to headache.
Introduction
Neck pain (NP) and headache (HA) are common in adolescents (1–5) and they seem to be closely associated (6–11), even if the possible causal relationship of NP and HA is still unknown. Although NP has been found to be associated with HA, it is not known whether adolescent HA is also associated with degenerative changes of the cervical spine.
Most magnetic resonance imaging (MRI) studies of HA patients have focused on cranial MRI. In a MRI study of the cervical spine, no difference was seen in disc bulging between adult patients with cervicogenic HA and healthy controls (12). When radiological changes in tension-type HA were compared with those in other types of HA or spondylogenic complaints in adults, tension-type HA was not found to be associated with changes in the cervical spine (13).
While degenerative changes of the cervical spine are common in asymptomatic adults, increasing with age (14–17), the clinical significance of the degeneration is obscure. At the age of 24–26 years, disc degeneration of the cervical spine was common in both asymptomatic subjects (N = 15) and those with NP (N = 16) (18). The prevalence of disc degeneration in asymptomatic 20-year-olds was 17% for men and 12% for women (15). Our study is the first population-based MRI study of the adolescent cervical spine. As degeneration of the spine is thought to have its onset in adulthood (15–17), the confounding effect of age-dependent physiological degenerative changes can be minimized by studying adolescents. Degeneration of the cervical spine in this age group could be a pathological finding associated with adolescent HA, especially when NP co-occurs with HA. In MRI studies of the lumbar spine, degeneration has been associated with adolescent back pain (19, 20).
The purpose of the present study was to determine whether adolescents with HA have more degenerative changes in the cervical spine than headache-free controls.
Methods
The present study is part of a population-based follow-up study of HA in schoolchildren. The original source population covered all 12-year-old schoolchildren in the city of Turku (total population 170 931) in south-western Finland. The questionnaire on HA was completed acceptably by 1135 (81%) of the 1409 eligible children aged 12 years. The details of the study design have been published previously (7, 8, 21). A flow chart shows the participation rates of the follow-up studies (Fig. 1).

Flow chart of the study population. HA, Headache; NP, neck pain.
Adolescents with HA at least three times a month and adolescents with no HA at the age of 16 years were invited to undergo MRI of the cervical spine 1 year later. Of participants with HA (N = 47/59, participation rate 80%), 17 had weekly NP (>3 times/month) and 30 had infrequent NP (<1/month). In adolescents with no HA (N = 22/37, participation rate 59%), the frequency of NP was <1/month (infrequent NP). HA sufferers with NP 1–3 times/month and HA-free participants with NP at least once a month were excluded from the MRI study.
HA frequency was defined as the monthly number of HA episodes during the preceding 6 months (response options 0–30/month). NP was evaluated on the basis of self-reported frequency of NP in the preceding 6 months (response options no, <1/month, 1–3/month, weekly or more often). The mean HA frequency in HA sufferers was 5.7 times a month (SD 4.7), with 4.7/month (SD 2.5) for HA sufferers without NP and 7.5/month (SD 6.8) for HA sufferers with NP. The classification of HA was based on a structured interview, neurological examination and the criteria of the Committee of the International Headache Society (IHS) available at that time (22). Of participants with HA, 19 had migraine type HA (IHS 1), 27 had tension-type HA (IHS 2) and one had HA not classifiable (IHS 13). Five participants had two kinds of HA at the age of 16 years. Their HA type was classified according to the more frequent type of HA.
Magnetic resonance imaging
The 1.5-T imaging system (Symphony; Siemens, Erlangen, Germany) was used for imaging with sagittal T1-weighted and T2-weighted images covering planes from the posterior fossa to the upper thoracic level. In addition, T2∗-weighted and T1-weighted axial images were obtained from the cervical spine. All scans were interpreted independently by three neuroradiologists (M.E., R.P. and P.S.) blinded to the participants' pain histories.
The degree of disc degeneration (DD) was graded as normal, mild (a decrease in disc signal intensity), moderate (the disc darker than the vertebral corpus) or severe (decreased signal intensity and narrowed disc space). Localization of DD was analysed in four ways: first, the occurrence of DD in the whole imaging area from C2 to Th4; second, the occurrence of DD in the upper neck (levels C2/3 and C3/4); third, the occurrence of DD in the lower neck (from C4/5 to C6/7); fourth, the spread of DD was evaluated (no DD, DD at one level, two levels or three or more levels). Disc bulgings of the cervical spine were graded as normal, protrusion and disc herniation. Any compression of the root and spinal cord was also recorded. Annular tears and foraminal stenosis were recorded, if present.
Extent of agreement
To prevent the influence of variation in the analysis between neuroradiologists commonly seen in mild degenerative changes, three independent examiners were used. The result was assessed as normal if at least two of the three neuroradiologists regarded it as normal. In the assessment of DD, the proportion of agreement was 81%. The first and the second neuroradiologists were of the same opinion on approximately 91% of findings, the first and the third on 77%, and the second and third on 77% of findings. Agreement was better in the lower cervical spine than in the upper cervical spine. In the assessment of disc bulging, the first and the second neuroradiologist agreed on 96%, the first and third on 90%, and the second and third on 92% of findings.
Statistical analysis
The descriptive values were expressed as means and standard deviations (SD), or frequencies and percentages. Univariate associations between categorical variables were evaluated using χ2 test and Fisher's exact test, where appropriate. The association of explanatory factors (neuroradiological findings) with HA was analysed using logistic regression (23) after adjustment for gender. Among HA sufferers, the association of explanatory factors with NP was evaluated with same method. The reliability of the MRI analysis was tested by calculating the proportion of agreement between examiners. P-values <0.05 were considered to be statistically significant. Statistical computations were done using the SAS System for Windows, release 8.02 (SAS Institute, Cary, NC, USA).
The study design and the informed consent procedures were approved by the Joint Ethics Review Committee of the Turku University Medical Faculty and the Turku University Central Hospital. Informed consent was signed by both the parents and participants in all phases of the study.
Results
Degenerative findings of the cervical spine
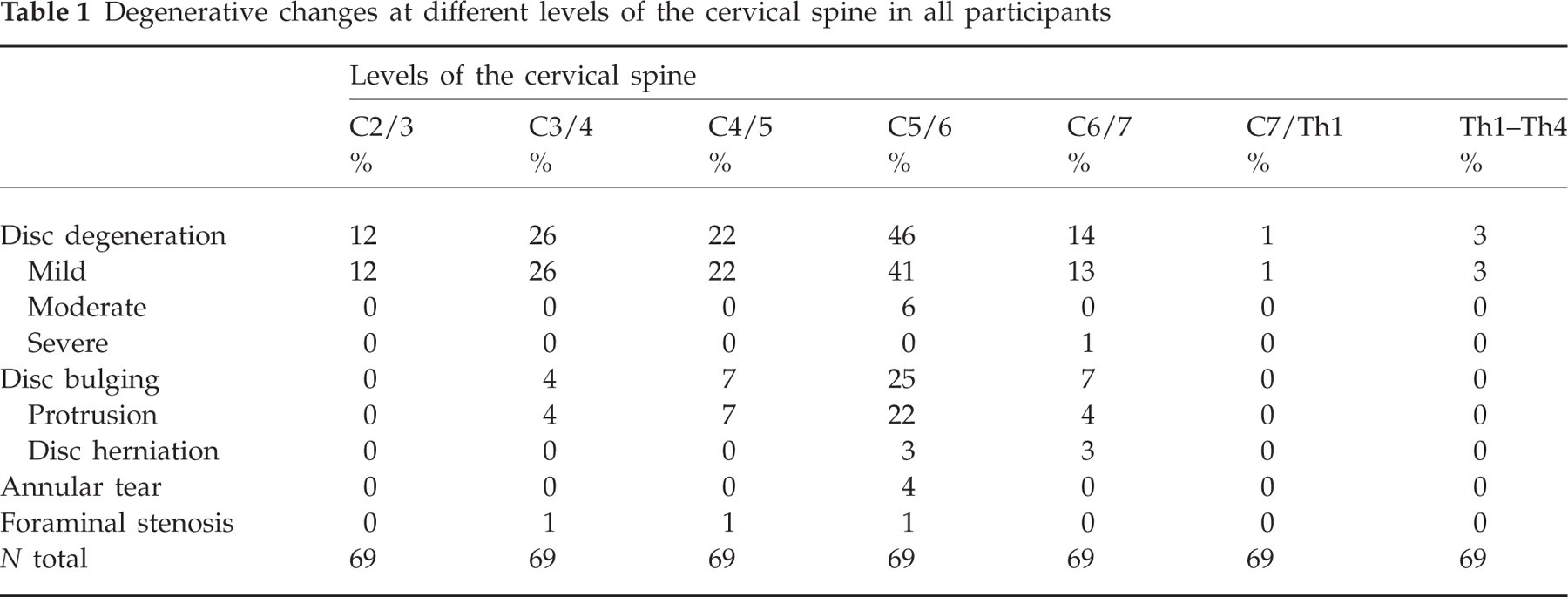
Of all participants, 67% had DD at least at one level from C2 to Th4. Table 1 shows the location of the degenerative changes in detail. DD was mainly mild and most commonly found at level C5/6 (46% of participants). Moderate DD was found in four participants and severe DD in one. Annular tears were found in three participants, all at level C5/C6. Mild foraminal stenosis was found in two participants at levels C3/4 to C5/6. Thirty disc bulgings were found in 20 participants, 57% of them at the C5/6 level. Four girls had disc herniations, but no compression of the nerve root or spinal cord was found. Annular tears were associated with concomitant disc bulgings and DD at the same level. Foraminal stenosis and 80% of disc bulgings were associated with DD at the same level. Because of the small number of discs with severe degeneration, mild, moderate and severe DD were combined in a DD group, and protrusions and herniations were combined in a disc bulging group for statistical analysis.
Degenerative changes at different levels of the cervical spine in all participants
Differences in degenerative findings between study groups
When HA sufferers were compared with HA-free controls, no significant differences were found in the occurrence or distribution of DD, disc bulging, foraminal stenosis or annular tears (Table 2). When HA sufferers with weekly NP were compared with HA sufferers with infrequent NP (Table 3), degenerative changes were not associated with concomitant weekly NP. Because of gender differences between the study groups, data were also analysed using gender-adjusted logistic regression. After adjustment for gender, no significant differences were seen in DD, disc bulging, foraminal stenosis or annular tears between HA sufferers and HA-free adolescents or between HA sufferers with weekly and infrequent NP. No significant differences were found in degenerative changes between participants with migraine (IHS 1) and those with tension-type HA (IHS 2).
Analysed factors in participants with and without headache

DD, Disc degeneration.
Analysed factors and headache with weekly or infrequent neck pain

DD, Disc degeneration.
Discussion
The most interesting finding in our study was that mild degenerative changes of the cervical spine were common at the age of 17 years in adolescents regardless of HA history. As far as we know, this is the first study of cervical spine degeneration in this age group. On the basis of previous studies of adults, it has been thought that degeneration of the cervical spine is a rare finding in the young (14–17, 24). As in our study, a recent study of young adults found that the rate of degeneration was higher than that of previous studies (18). This difference in the rate of degeneration can not be explained by the differences in MRI equipment. Improvements in MRI technology have increased sensitivity in the detection of small anatomical changes, such as disc bulging and root compression. In the detection of internal signal changes revealing disc degeneration, however, the use of faster sequence techniques and increased field strength in principle decrease tissue contrast rather than improve it. The increase in degeneration of the cervical spine as indicated by recent studies (18) is probably a true finding. The reason for this change could be the increasingly sedentary way of life and the increasing use of computers, inducing more stress to the cervical spine. The sitting position in using a computer could diminish the lordosis of the spine and, on the other hand, the forward position of the head could increase the stress on the neck muscles. The biomechanical models of the cervical spine support this hypothesis of the influence of the sitting position on the increase in degeneration. In these models, high joint loads on the spine have occurred during muscle contraction (25) and other types of external loading (26). High joint loads of the spine could lead to degenerative changes (27, 28).
Degenerative changes were most common at level C5/6, in agreement with previous findings in adults (15, 16, 28–30). At level C5/6, the extension–flexion motion is considerable (31) and it has been thought that the large extent of motion could induce degeneration. Degeneration at this level has also been associated with compression loading of the spine (28). Under axial compression loading, the dural sac has been shown to narrow, especially at the C5/6 interspace in asymptomatic individuals (32).
No previous studies have been published of HA and cervical MRI in adolescence. No association between HA and DD of the spine was seen in our study. Provided that HA can be caused by degeneration in the cervical spine, the convergence between the trigeminal afferents and the upper three cervical nerves suggests that degenerative changes in the upper neck may be more likely to cause HA than degeneration in the lower cervical spine (33). In our study population, however, degenerative changes were found in the lower part of the cervical spine. In adult HA patients, dynamic spinal X-rays have shown joint dysfunction and changes in posture both in migraine and tension-type HA (34). On the other hand, the MRI findings from the cervical spine did not correlate with cervicogenic HA compared with HA-free controls (12). As in previous studies of adults (12, 13, 34), our study found no significant association between HA type and DD. HA type was not included in the inclusion criteria of this MRI study, because the fluctuation of HA type is common in this age group (35, 36) and we assume that juvenile migraine and tension-type HA are not totally different entities and may represent a continuum.
It seems that the often reported association of self-reported NP with HA in adolescence (6–10) can not be explained by degenerative changes. In our study, HA with concomitant weekly NP was not associated with permanent structural changes of the spine. It could, however, be presumed that the flexible spine in this age group (37) is prone to become loaded, but the loads induce reversible dysfunction of the spine and muscles associating with HA and concomitant NP. These reversible, functional changes could be more important than the degeneration of the spine for pain symptoms in this age group. Also in previous adult studies, pathophysiological changes of the cervical spine have explained only a small proportion of pain, and no clear association has been found between self-reported NP and DD (18, 38, 39).
It is not known if headache can stem from disc degeneration in the cervical spine. Disc degeneration starting in adolescence could simply be an unpreventable normal process of the ageing body without severe consequences. However, early degenerative changes may lead to HA or NP later in adult years. In the adult study of Gore, degeneration at level C6/7 predicted the incidence of NP in a follow-up of 10 years (40).
In our study, disc protrusions or herniations were not associated with HA or with HA and concomitant NP. In a previous study of young adults (24–27 years old), only disc herniations, but not protrusions of the cervical spine were associated with NP (18). The slight difference between our study and that of young adults could result from different age groups and different inclusion criteria. In our study, the number of foraminal stenoses and annular tears was low, as expected. These few findings render statistical analysis insensitive. Thus, possible associations with symptoms remain unclear. When adults with and without pain symptoms in different age groups have been compared, foraminal stenosis of the lower cervical spine has been associated with pain (41).
It has been shown that intra- and interobserver differences in defining cervical degeneration in MRI can be remarkable (42). To reduce the influence of these errors, MRI scans were interpreted by three experienced, independent neuroradiologists. Although some differences were seen in their analyses, the rates of agreement were fairly good. No conclusions can be drawn on possible associations of degenerative changes and gender in this study population because of the different numbers of girls and boys in the study groups. The study has sufficient power to detect relevant differences in the prevalence of disc degeneration, but because of the low number of headache-free participants, the study is not sensitive to detect small differences.
Conclusion
Mild degenerative changes of the cervical spine seem to be common in 17-year-old adolescents, but they can not be regarded as a cause of headache.
Acknowledgements
This study was supported by grants from the city of Turku, University of Turku and University Hospital of Turku. Appreciation is expressed to Olli Kaleva BSc for skilful computation of the statistical analyses, and to Mrs Inger Vaihinen for her versatile assistance.