
Abstract
Objective
The objective of this article is to determine the monthly variation of emergency department (ED) visits for pediatric headache. We hypothesized youth have increased headache-related ED visits in the months associated with school attendance.
Methods
Using a United States representative sample of ED visits in the National Hospital Ambulatory Medical Care Survey from 1997 to 2009, we estimated number of visits associated with ICD-9 codes related to headache, migraine, status migrainosus, or tension-type headache in 5- to 18-year-olds. Age-stratified multivariate models are presented for month of visit (July as reference).
Results
There was a national estimate of 250,000 ED visits annually related to headache (2.1% of total visits) in 5- to 18-year-olds. In 5- to 11-year-olds, the adjusted rate of headache-related visits was lower in April (OR 0.42, 95% CI 0.20, 0.88). In 12- to 18-year-olds, there were higher rates in January (OR 1.92, 95% CI 1.16, 3.14) and September (OR 1.64, 95% CI 1.06, 2.55).
Conclusions
In adolescents we found higher ED utilization in January and September, the same months associated with school return from vacation for a majority of children nationally. No significant reduction in the summer suggests that school itself is not the issue, but rather changes in daily lifestyle and transitions.
Introduction
Headaches are a common problem in the pediatric population. Up to 10% of children and 28% of adolescents experience reoccurring headaches (1,2). These headaches result in significant disability affecting children and their families (3,4).
School-related issues often become the center point for the child or adolescent with headaches. For any child, school can be a source of stress and anxiety from the pressures of school work, sporting activities, and peers (5–7). For a child with recurrent headaches, additional distress may arise from missed school days and social activities due to headaches, relationships with teachers, and managing headaches while in school (8). School-related stress and sleep disturbance are commonly reported by patients and families as triggers for their headaches (9–11).
Transitions from vacation to the academic semester may be associated with increased stress related to school onset and changes in lifestyle behaviors. Despite subjective reports of school-related headache triggers, few have studied the seasonal variation of headache exacerbation in children and adolescents (12). The objective of the present study was to use a nationally representative survey to evaluate the monthly variation of emergency department (ED) visits for headache as a surrogate marker of headache exacerbation in children and adolescents. We hypothesized youth have increased headache-related ED visits in the months associated with school attendance.
Methods
We evaluated ED data from the 1997–2009 National Hospital Ambulatory Medical Care Survey (NHAMCS) for children and adolescents ages 5–18 years old. This study was exempt from institutional review board review. A full description of NHAMCS survey methods is published elsewhere (13). Briefly, the NHAMCS is a four-stage probability sample conducted annually by the National Center for Health Statistics of United States (US) noninstitutional, general, and short-stay hospitals. ED diagnoses were coded using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9 CM).
For this study, we defined ED visit for headache as any ED visit with the ICD-9-CM code for headache, migraine, tension-type headache, and cluster/trigeminal autonomic cephalalgia (784.00, 346.XX, 339.XX, and 307.81) in any of the three provided diagnostic fields. We excluded ED visits with any indication of infection, neoplasm, or trauma if any of the following ICD-9-CM codes were present in any of the diagnostic code fields: infectious and parasitic disease (001–139), central nervous system (CNS) infection (320–326), otitis media and mastoiditis (381–383), respiratory infections (460–466), pneumonia and flu (480–488), diarrhea/gastroenteritis (787.91), fever (780.6); neoplasms (140–239); fracture of skull (800–804), fracture of neck (805), intracranial injury (850–854), wound of head (873), contusion of face scalp, neck except eyes (920), contusion of eye and adenexa (921), and crushing injury of face, scalp and neck (925).
Covariates assessed demographic data including age, sex, race, ethnicity, US region (Northeast, Midwest, South and West), metropolitan statistical area (MSA) of the hospital (urban and nonurban), and ED disposition (admitted or discharged). Region and MSA categories represent standardized geographical divisions defined by the US Bureau of the Census.
Analysis
We used Stata 12.1 software (StatCorp, College Station, TX) to determine nationally representative estimates and 95% confidence intervals (CIs) using assigned patient weights, which adjust for selection probability. Chi-square was used to examine the relationship of headache compared to nonheadache-related ED visits for demographic variables and disposition. Multivariable logistic regression was used with July as reference to estimate the odds ratios (ORs) for ED visit for headache each month, adjusted for all other covariates in the analysis. A two-sided p value of 0.05 was considered significant and was not adjusted for multiple comparisons.
Results
There were a total of 43,688 ED visits with a national estimate of 12 million visits annually in 5- to 18-year-olds from 1997 to 2009. We excluded 18,005 ED visits for codes related to infection, neoplasm, and head trauma. The children and adolescents were 50% female and predominately non-Hispanic white (61.8%).
There were 909 (weighted 2.1%) ED visits related to headache with a national estimate of 250,000 (95% CI 220,000, 280,000) ED visits annually in individuals 5 to 18 years old from 1997 to 2009. We excluded 225 visits for secondary ICD-9-CM codes shown in Figure 1. Of the 909 headache-related ED visits, individuals were predominately female (57.1%) and non-Hispanic whites (57.0%) (Table 1). ED visits occurred primarily in urban settings (80.7%) and resulted in hospital admission in 4.5% of cases.
Headache case selection. Demographic data with number of visits, national estimate, and weighted percentage for headache- and nonheadache-related visits.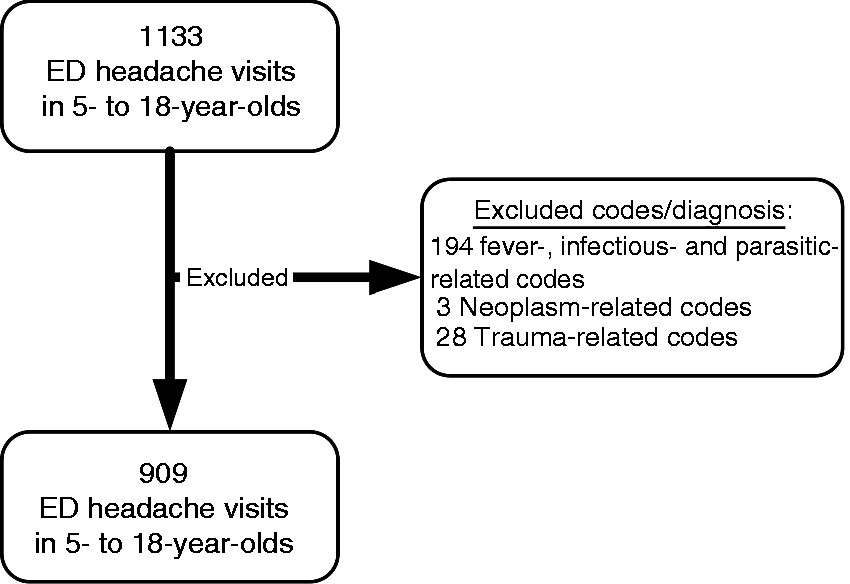

Overall, the highest proportion of visits related to headache occurred in January (3.0%) and the lowest in June (1.6%). With July as the reference month, January was the only month with significant increased adjusted odds of headache visits (OR 1.60, 95% CI 1.10, 2.31) in the overall cohort. Percentage and adjusted odds of ED visits for headache by month and age category are shown in Figure 2. In the 5- to 11-year-old subgroup, the highest proportion of ED visits for headache was in January (2.4%), although the difference from July was not significant (OR 1.16, 95% CI 0.70, 1.93). There were significantly lower ED visits in April (OR 0.42, 95% CI 0.20, 0.88). In the 12- to 18-year-old subgroup, there were significantly higher ED visits in January (OR 1.92, 95% CI 1.16, 3.14) and September (OR 1.64, 95% CI 1.06, 2.55).
Percentage (top row) and adjusted odds ratio (bottom row) of emergency department (ED) visits for headache in both age categories. HA: headache.
A sensitivity analysis was performed and the pattern observed was stable across individual years from 1997 to 2009 (data not shown). Our population showed no change in headache visit patterns when not excluding infectious-related codes (data not shown).
Discussion
Recurrent headaches are highly prevalent in children and adolescents. Patterns in pediatric headache exacerbation have not been well studied. We found increased proportions of ED visits in the US for headache in adolescents in January and September. Nationally, these are key months associated with transitions from school vacation to school onset. During these transitions, students are more apt to have changes in eating patterns, disruptions in sleep, and increases in stress (14–16). Meal skipping, poor sleep, and stress are also the most commonly reported headache triggers (9,11).
In contrast with adolescents, there was no monthly trend for ED exacerbation in younger children (5–11 years). These younger children may be prone to a set of triggers separate from their adolescent counterparts. Younger children may experience school-related anxiety at onset of the academic year; however, summertime competitive sports for younger children may contribute to anxiety during the summer. Overall, there was no seasonal trend in younger children. Compared to early childhood, adolescence is associated with increases in school-related stress, poor sleep patterns, sedentary behavior, and meal skipping (15–17). These all may be particularly relevant during transitions from vacation to school. Developmental and hormonal changes during puberty may contribute to these lifestyle behavior changes or adolescence ability to cope with pain (15,18).
Stress was initially defined broadly by Hans Selye as a nonspecific response of the body to any demand for change (19,20). A stressor can be either physical or psychological (21,22). The individual's perception of the stressor—modified by coping mechanisms and past experiences—subsequently produces a unique response to the stressor. In an adolescent with headaches, there likely is more than one stressor, including school, relationships, poor sleep, or the headache itself. Humans benefit from small levels of repeated stress; large changes in stress from baseline levels likely result in a stress-related disease (21,23,24), a phenomenon that may be occurring in adolescents as they transition from vacation to school onset. Research is needed to understand the physiological and psychological responses of stress in a child or adolescent suffering from headaches.
Sleep disturbance is a commonly reported trigger for pediatric headache. In adults, poor sleep quality, sleep disturbance, and insomnia are associated with primary headache disorders (25–29). Uniquely, Houle et al. (2012) found an additive effect of sleep and stress in triggering a headache (26). Sleep and headache share common physiological and neuroanatomical pathways and may contribute to the higher co-incidence of these two phenomena (30). Adolescents have high rates of sleep disturbance including difficulties in initiating and maintaining sleep, which is associated with poor school performance, impaired attention, and school absenteeism (31–33). Transitions from vacation to school may be a particularly vulnerable time for triggering headaches due to sleep disturbance.
Our results highlight that the transition from vacation to school onset may be particularly important in children and adolescents with headache. We observed increases only in September and January and not in months associated with transitions from school to vacation. In addition to changes in sleep and stress, changes in lifestyle habits also influencing this effect may include eating and hydration habits as well as physical exercise routines.
Headache exacerbations in these months may be due to the viral season in January or sports-related trauma during the summer months. However, in our study, we excluded cases with any indication of infection or trauma in the diagnosis fields. Furthermore, younger children, more prone to infection, showed no amplification of headache visits during the viral season months when we included infectious-related codes (data not shown). Individuals with headache frequently complain of weather and barometric shifts as triggers for their headaches (11). Although changes in weather may account for a portion of the relationship we saw, the precise timing with respect to school-onset suggests changes associated with transitions from vacation to school are making a major contribution.
Our use of a secondary database introduces limitations related to potential variation in the accuracy of diagnostic coding. We remained broad in our definition of headache cases to improve our sensitivity in detecting monthly variation of headaches, limiting our ability to make any conclusions on the subtype of headaches associated with the identified months. Prospective diaries with detailed accounts of stress, sleep, and eating patterns along with collection of biomarkers such as cortisol and actinography may help explain variation of headache exacerbation. We could not account for weather patterns in our analysis and these would be a consideration for future studies. Finally, headache visits in the ED are being used as a surrogate marker for headache exacerbation for children and adolescents in our study. It is unknown if total ED visits related to headache is a good marker for community burden of total headache; ED visits likely represent the more severe spectrum of headache disease. Different patterns could be seen for headaches treated with home therapy not requiring an emergency room visit.
Conclusions
In adolescents aged 12 to 18 we found higher ED use for headache in January and September, the same months associated with school onset in the US. Alternatively, there was no disproportionate use in these months for younger children. To help inform future interventions, this monthly variation of ED use should be explored further with detailed headache diaries for possible explanations including school-related stress, sleep patterns, and other lifestyle habits.
Clinical implications
Adolescents use the emergency department (ED) for headache more in January and September, which are key months associated with transitions from vacation to school. Developing behavioral and pharmacologic treatment plans with adolescents prior to this transition may decrease the number of headache-related ED visits seen during these months.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.