
Abstract
Background
Tension-type headaches (TTH) are common among children worldwide and mean a potential risk of disability and medication overuse headache. The associated mechanisms, however, remain unsolved. Our study investigated muscle strength in the neck-shoulder region, aerobic power and pericranial tenderness in girls with TTH compared with healthy controls.
Methods
A blinded case-control study comprising 41 girls with TTH and 41 age-matched healthy controls. Standardised testing of isometric maximal voluntary contraction (MVC) and force steadiness of neck flexion and extension, as well as MVC and rate-of-force development of dominant shoulder, was conducted. VO2 max was recorded by a submaximal ergometer test and pericranial tenderness by standardised manual palpation. Logistic regression analyses were applied.
Results
Girls with TTH demonstrated significantly higher pericranial tenderness than controls, in correlation with headache frequency (r = 0.66, p < 0.001). Results indicated that the odds ratio of girls having headache are 7.6 (95% CI 1.4–40.9) for weak to strong shoulder muscles; weak to average neck-shoulder strength OR 3.1 (95% CI 1.2–8.1); neck flexion strength OR 1.3 (95% CI 1.0–1.6) and 5.2 (95% CI: 1.4–19.6) for each unit of decrease in VO2 max.
Conclusions
Reduced neck-shoulder strength and aerobic power together with increased pericranial tenderness are associated with TTH in girls. Future interventions should be directed towards health promoting patient educational programmes on enhanced physical exercising. Much more exact and detailed research in young girls and boys are needed.
Keywords
Background
Frequent episodic and chronic tension-type headaches (TTH) are common disorders among children worldwide. The 1-year prevalence of frequent episodic TTH with headache 1 to 15 days a month is up to 18% in children, depending on age and sex (1,2). The prevalence of chronic TTH, which is defined as headache 15 or more days a month, is reported to be around 2% in a paediatric population (1,2). The most common risk factor for progression to chronic headache in children with TTH is medication overuse (2,3). Although important for planning a relevant intervention, knowledge of contributing physical and psychosocial factors and the consequences of pain in children is quite limited. A child with frequent or chronic pain is at serious risk of functional impairments in various areas (4,5) that influence the child's physical and psychological development. Until now the most reported difficulties are inattention, lack of concentration in school and emotional symptoms interfering with family and social life (5).
Pain and muscular functions
The neuromatrix model of pain redeveloped in the last decade by Ronald Melzack (4) describes chronic pain as the result of homeostasis-regulation patterns that have failed, where abnormal neural programmes of maintained alertness may produce sensory, motor, affective and cognitive responses. Changed motor output as a dimension of pain initially has the purpose of taking action by either stabilising the body with co-contractions or preparing for movements (6), but reorganisation of motor output in chronic pain conditions is not well understood.
In adults with chronic TTH, pathophysiological changes in the pericranial muscles are the most well known clinical findings of importance (7–9). Research concerning muscular functions in the neck-shoulder region in children and adolescents with TTH is in its initial stages. Oksanen et al. (10) investigated strength and mobility in the neck-shoulder region in adolescents and showed that girls with TTH had significantly weaker endurance in both dominant and non-dominant upper extremities than healthy girls. In another study (11), Oksanen et al. found differences in the neuromuscular co-activation patterns and force in the neck-shoulder muscles measured by electromyography and dynamometry comparing adolescent girls with TTH, with migraine and headache-free controls. They hypothesised that change in motor strategies and force imbalance in the neck-shoulder region with a reduced metabolism might contribute to headache (11). In a study including adult women with chronic TTH, Fernandez-de-las-Penas et al. (12) found lower force and higher co-activation of neck muscles in extension and flexion tests which reflects a more protective motor strategy than in healthy controls. Altogether, these results suggested changed motor strategies with a trend of lower force production and higher co-contraction patterns.
A similar trend is found in other pain conditions in the neck-shoulder region. Differences in isometric neck strength in women with chronic neck pain are documented with a significantly lowered peak force capacity by several researchers (13–15). In female workers with trapezius myalgia, Andersen et al. (15) investigated rapid muscle activation and force capacity compared with controls. The major findings were a reduced ability to rapidly activate the painful trapezius muscles measured by rate of force development (RFD). Rate of force seems to be a more sensitive parameter than strength (15,16). It is not known if any of these reported muscular functional changes in the neck and trapezius muscles are to be found in girls with TTH.
Physical activity and aerobic power
The existing knowledge about general health conditions, and especially aerobic power, in children with TTH is lacking. The Nord-Trondelag Health Study I (HUNT) revealed that physically inactive adults were more likely to suffer from non-migraine headache at follow-up 11 years later (17). In a subsequent cross-sectional study (HUNT II), a self-reported low level of physical activity (none or less than 1 hour per week) was associated with higher prevalence of migraine or non-migraine headaches (17), but the causal relationship is still unclear. Aerobic power measured by predicted oxygen uptake, however, has not yet been examined in relation to children and adults with TTH.
Pericranial tenderness and sensitivity
Combined with TTH, the descending part of the trapezius muscle is found to be the most tender muscle among the pericranial muscles for all age groups (1,7,18,19). Reports from a population-based study of 12-year-old Finnish children (1) showed that 35% of those children reporting episodic TTH also reported muscle tenderness in the neck-shoulder region compared with 21% of those without headache. Hypersensibility in pericranial muscles by palpation is likewise found in Swedish schoolchildren with episodic and especially chronic TTH (19). Based on a study of 25 children (boys and girls, mean age 8.9) with frequent episodic TTH, Fernandez-de-las-Penas et al. (20) found a widespread bilateral hypersensitivity and a significant negative relationship between pressure pain threshold over the upper trapezius muscle and years of headache compared with healthy controls. Their findings support the hypothesis that the pathophysiology of TTH is closely related to pericranial muscles in children. It is hypothesised that the initial stimulus may be either mental stress, motor stress or a local irritative process (7) leading to a peripheral and central sensitisation of the nervous system (8,18,20), most likely preceded by pericranial tenderness (9,18).
Aims
In order to be able to investigate a broader picture of the child's health and power status in contrast to exclusively assessing the neck-shoulder region, this study aimed at examining the combined measurements of muscle strength in the neck-shoulder region, aerobic power and pericranial tenderness in girls of 9 up to18 years of age, and their associations with frequent episodic or chronic TTH compared with healthy controls. We hypothesised that we would identify muscular and aerobic power dysfunctions associated with headache.
Methods
Design
A blinded clinical-based case-control study with report was conducted in accordance with the STROBE Statement (21). Registration number: ClinicalTrials.gov; H-3–2009–081.
Participants
A sample of 87 girls of 9 up to 18 years of age were available to enrol in the study, 44 of whom were exclusively diagnosed with either a frequent episodic TTH (10 episodes on ≥1 day but < 15 days per month for at least 3 months) or chronic TTH (≥15 days per month on average for >3 months), monitored in a diary, thus fulfilling the International Classification of Headache Disorders 2nd Edition criteria (22) All diagnosed after the first of May 2010, the participants were recruited from the Children's Headache Clinic, Glostrup and Herlev Hospitals. Exclusion criteria were migraine headache more than one episode per month for a period of 6 months, a history of trauma, arterial hypertension or intracranial hypertension, headache secondary to a cervical or other morbidity and headache associated with a psychiatric comorbidity. Another exclusion criterion was headache associated with a radical learning disability or complicated social situation that required special education and/or community involvement. Girls who had been or were enrolled in other treatment programmes at the Children's Headache Clinic were also excluded. All the girls with TTH underwent a clinical diagnostic and neurological examination including examination of the spine by the paediatric department's neuropaediatricians and one specialist physiotherapist. No preventive headache medication and/or analgesic overuse were allowed before and during the study period. None of the participants were allowed intake of analgesics within 12 hours before testing. Three of the enrolled girls with TTH failed to start.
As controls, 43 healthy girls were recruited from local schools following specific guidelines from the Danish National Committee on Biomedical Research Ethics. Sealed envelopes with information were distributed to the children by their teachers at school. In order for the children to participate, their parents had to actively contact the researcher. Two girls did not meet the inclusion criteria. Thus, 41 age and geographically matched healthy girls with no more than one episode of headache per month and no other illnesses participated as controls. Figure 1 provides a flow diagram of enrolment of participants.
Flow diagram of enrolment of participants in the case-control study. TTH: tension-type headache.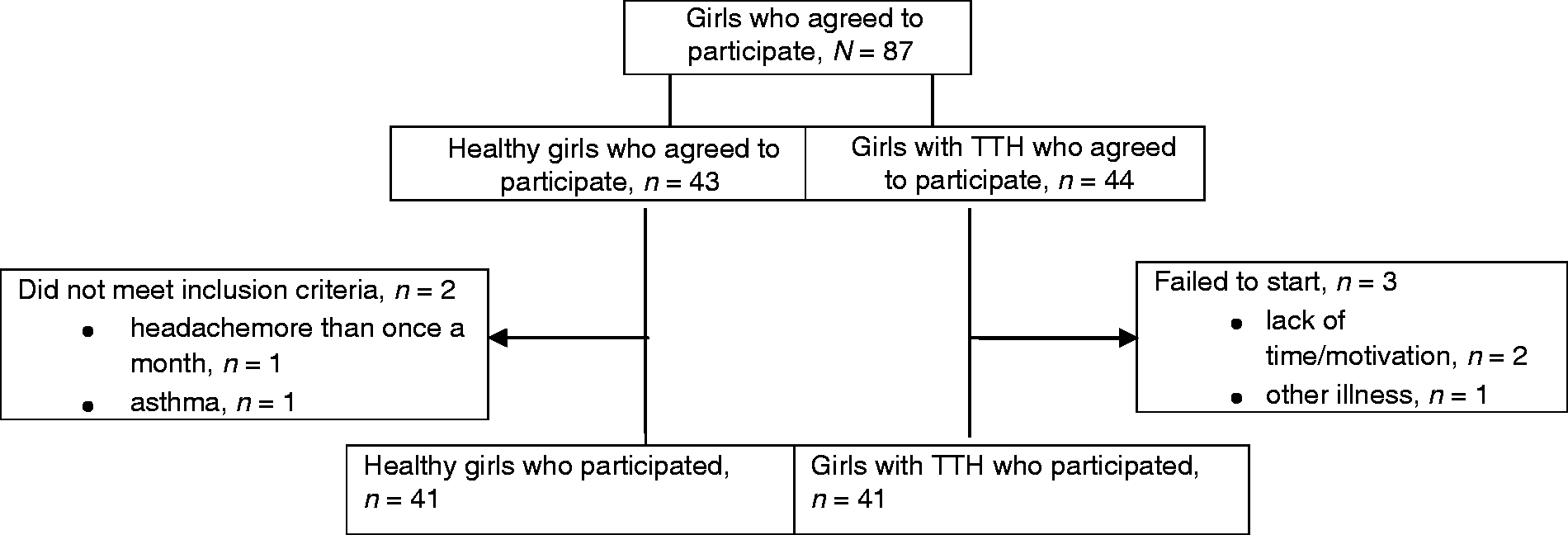
This study followed the ethical principles of the World Medical Association's 2008 Declaration of Helsinki (23), the United Nations 1989 Convention on the Rights of the Child (24), Danish National Committee on Biomedical Research Ethics for Hospitals in the Capital Region of Denmark and the Danish Data Protection Agency. The parents gave written informed consent and the children gave oral informed assent. According to the ethical guidelines, children over the age of 15 also received special age-appropriate information. Participants were informed about confidentiality and the right to withdraw from the study at any time without affecting their treatment.
Overall test procedures and measurement
A bio-analytic research assistant (HA) blinded to the participants' histories and trained and experienced in the following specific test methods, conducted the testing. The participants were given detailed information to familiarise them with the procedure. A co-assistant, also blinded, assisted the child during test procedures. The test procedures were conducted in a warm comfortable room and followed a standardised protocol:
Age and anthropometric measures were noted. Self-reports of headache were monitored daily using a visual analogue score (VAS) (25) in a monthly calendar. Baseline mean headache frequency, intensity and duration over 28 days prior to the test date were calculated for girls with TTH. In order to assess hypermobility as a potential confounder associated with headache, general joint mobility was screened using the Beighton Score (26) with nine points as a maximum. The cut-off for positive findings of hypermobility was 5/9. Tenderness of pericranial muscles was examined in a sitting position in a chair with adjustable neck and leg support using the Total Tenderness Score (TTS) system validated by Bendtsen et al. (18,27,28). A total score was calculated based on the standardised manual palpation procedures of seven bilateral sites (masseter, frontalis, temporalis, processus mastoideus, occipital insertion, trapezius and sternocleidomastoideus) using a four-point scale. The maximum possible total score was 42 points. Isometric muscular measurements were conducted using a computerised force transducer, model Vishay Nobel, type KIS-2, max. 2kN (Vishay Precision Group, Malvern, PA, USA) wall-mounted on a custom-built adjustable stand. The child was positioned on a chair with the upper and lower trunk fixed with belts. For neck flexion measurements, the lower edge of the padded force transducer corresponded with the line between the eyebrows, whereas for neck extension measurements, the pad was positioned with the lower edge corresponding with the protuberantia occipitalis. The testing included isometric maximal voluntary contraction (MVC) in neck flexion and extension from a neutral upright position, and the ability to stabilise (FS force steadiness) against a resistance of 30% of MVC for 25 seconds in the same directions. For shoulder measurements the child was asked to lie on a mattress in a supine position. The dominant shoulder was then positioned in external rotation and abduction, while the elbow was stretched to position the back of the wrist on the pad. The instruction to the child was to press as quickly and as forcefully against the pad, measuring, respectively, the rate of force development (RFD) and the MVC over three trials. Aerobic power was determined by a Monark Pendulum Ergomedic 939E PC bike (Monark Exercise AB, Stockholm, Sweden) using a submaximal Åstrand test procedure and nomogram for predicting VO2 max (29). Heart rate was monitored using an adjustable Polar pulse belt (Polar Electro Danmark ApS, Holte, Denmark) and recorded continuously on a computer.
Accurate details of the measurement system, calibrations and analyses of test-retest repeatability and variability are provided by Tornøe et al. (30).
Statistical analyses
A preliminary power calculation showed that 45 girls were required in each study group to be able to detect a significant difference between the groups with a power of 80%. Stratifying the girls into groups of FETTH and CTTH was deselected in order not to lose power. The distribution of data was examined by means of a Kolmogorov-Smirnov test (31) and normal distribution plots. Descriptive statistics were used to describe the central tendency, dispersal and trends of data. For each participant the maximum (peak) forces of three trials for strength and rate of force development test results were calculated. Shoulder data were missing from one healthy girl. Test results did not fulfil the assumption about normality and therefore comparisons of test results between girls with TTH and healthy girls were performed using a nonparametric independent-samples Mann-Whitney U test while Spearman's correlation analysis was used for correlations. A binary logistic regression analysis (32) was used to examine the associations between independent power capacity variables and the dependent variable headache frequency. Headache frequency was dichotomised into ‘headache’ or ‘no more than one episode/month of headache’. The independent variables comprised: (1) sum of all peak MVC forces; (2) sum of all peak neck MVC; (3) peak neck flex MVC; (4) peak shoulder MVC; and (5) peak shoulder RFD; (6) predicted maximal oxygen uptake. In the binary logistic regression the assumption of linearity between the independent variables and the log-odds of the dependent variable was examined by splitting the independent variables into ordered quartile categories. If the odds ratios of the categories showed a linear increase or decrease, the linearity was accepted; otherwise the ordered categories were used in the model. Results were adjusted for age and body mass index (BMI), which are the confounders related to growth. For all tests, the level of significance used was 0.05. No adjustments for multiple testing were applied.
SPSS 17.0+20.0 were used for all statistical analysis. Force steadiness variables were removed from the analysis, after our test-retest study showed systematic changes in the mean between two test occasions, and thus need further examination before applied in research studies (30).
Results
Age and anthropometric measures of girls in study groups; mean (SD), N = 82.
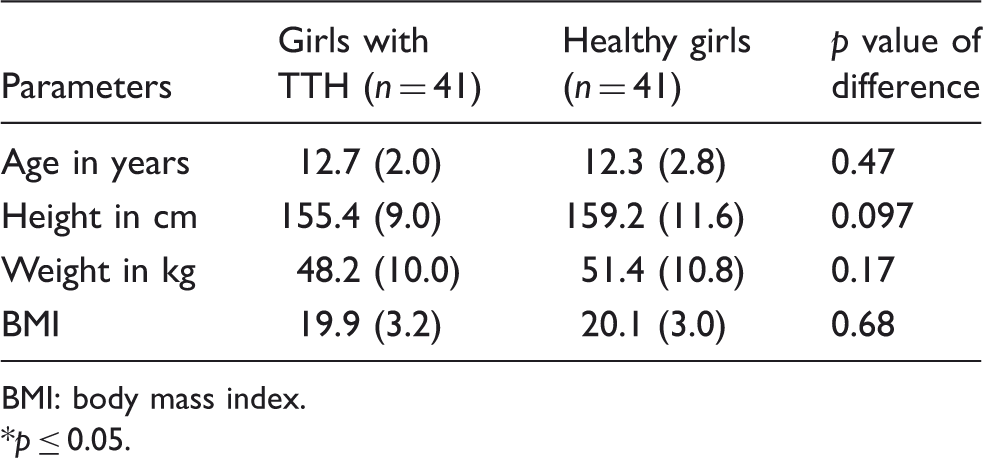
BMI: body mass index. *p ≤ 0.05.
Headache characteristics of girls with TTH; median (1–3 qrt.), n = 41.
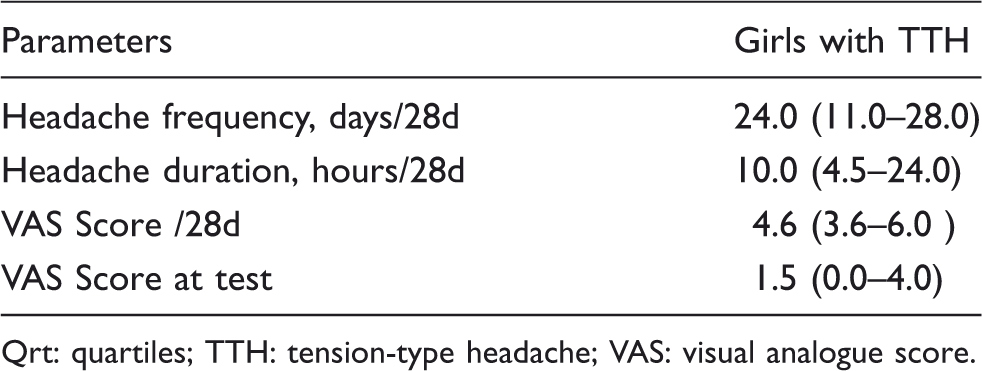
Qrt: quartiles; TTH: tension-type headache; VAS: visual analogue score.
Girls with headache demonstrated a statistically significantly higher TTS than controls (p < 0.001) (see Table 4). The seven palpation sites were all statistically significantly more tender in TTH girls compared with healthy girls (p ≤ 0.001 for trapezius, sternocleidomastoideus, temporalis, frontalis and masseter, and p ≤ 0.003 for occipital insertion and proc. mastoideus bilateral). The most tender locations were the upper trapezius, its occipital insertion and the sternocleidomastoideus. There was a highly significant and positive correlation between the TTS and headache frequency (r = 0.66, p < 0.001). The analysis did not show any correlation between tenderness and headache intensity by VAS (r = 0.16, p ≤ 0.33).
The relationship between headache and sum of peak MVC, peak neck MVC, peak neck flex MVC, peak shoulder MVC and RFD and oxygen uptake, respectively, N = 82.

MVC: maximal voluntary contraction; RFD: rate of force development.
*p ≤ 0.05; results are adjusted for age and BMI.
Differences between study groups; median (1–3 qrt.); independent-samples Mann-Whitney U test, N = 82.

MVC: maximal voluntary contraction; N: Newton; RFD: rate of force development; s: second; TTH: tension-type headache; VO2 max: predicted maximal oxygen uptake. *p ≤ 0.05.
Discussion
Expecting to find specific dysfunctions, we identified an association between reduced strength in the neck-shoulder muscles, aerobic power and TTH in girls. To the best of our knowledge, this is the first time that the combined measures of strength and aerobic power are associated with TTH in children. HUNT I and II were the first to discover physical activity as a risk factor in adults (17) and emphasise the close inverse relationship between physical activity and TTH, while Oksanen et al. was the first to address the association between a sedentary lifestyle in adolescents and TTH (33), together with more studies of neck-shoulder strength (10,11).
Our findings revealed a significant difference in girls with frequent episodic or chronic TTH compared with healthy girls with strongly significant increased pericranial tenderness by palpation. The difference in TTS supports the earlier findings that there is a positive relationship between headache frequency and pericranial tenderness in children as well in adults (7,9,20). The upper trapezius muscle and its occipital insertion are the most tender sites in the present study, which is similarly the case in prior studies in children (19) and corresponds with the findings in adults reported by Jensen and Bendtsen (7,8). Thus the results supplement the previous results and hypotheses about the relationship between pericranial tenderness and chronic TTH as symptoms of hypersensitivity (20). Discussing the applicability of the TTS, a study of adults with non-specific neck-shoulder pain found the levator scapulae, neck extensors and infraspinatus appearing to be more tender than the upper trapezius muscles (34) showing that discriminating between different groups of patients using manual palpation of tenderness is possible.
The findings in the present study also suggest that girls with frequent episodic or chronic TTH present a general picture of reduced physical capacities in both strength and aerobic power. We are unable to make any conclusions about the cause and the effect hereof in this clinical based case-control study, but it seems important to debate whether the decreased physical capacity relates to a developmental and exercise deficit in early childhood rather than pain avoidance. There is a strong need to further examine this aspect in children with headaches. Fear of pain and avoidance of activities have been debated in relation to the chronic pain mechanism in lower back pain (35) and also in the field of headache and neck-shoulder pain (15), but it remains undocumented. In a large survey done in the USA, Strine et al. (5) found that children with a frequent or severe headache condition were significantly disabled, being more likely to exhibit emotional symptoms that interfered with their home life and leisure time, not to mention inattention and restlessness at school. A decline in specific physical capacity was not investigated or reported. Anttila et al. (1) found that in 12-year-old Finnish children with TTH, 11.7% reported frequent physical activity aggravation compared with 39.9% in children with migraine. Based on a study of 130 Swedish children, Laurell et al. (36) reported that especially children with migraine headache reported additional physical pain complaints and that the group suffering from frequent TTH did not differ significantly from the group without headache except for neck pain. Physical functioning was not reported. In a study by Oksanen et al. (33), children were divided into groups based on whether they suffered from migraines, episodic TTH or were healthy children and were interviewed about leisure time activities, sports and intensity, physical activity and the use of screen time. Two-thirds of the children with TTH were boys, which is rather unusual in most studies. Children with episodic TTH or migraine used computers significantly more days per week than healthy controls. To date, we do not have strong evidence that children with frequent episodic or chronic TTH avoid physical activity to a degree that might affect their physical capacities significantly. Although it is a question of which came first, the cause or the effect, further research is needed that tests the hypothesis on exercise deficits and TTH in children. As a whole, the present study suggests that parameters such as neck-shoulder strength and aerobic power, which are reflecting the child's general health status as well as specific physical functions, do influence girls suffering from frequent or chronic TTH.
Limitations and comments
The testing in the present study was conducted by a single experienced research assistant blinded to the history of the child. The testing was conducted based on a standardised protocol and the procedures are highly reproducible. The tests used were examined for repeatability in a test-retest study and found stable (30). Muscle force related to posture habits is not examined in this study, nor does this study deal with coordinated motor patterns between specific muscles. Further research is needed in order to study postures in children with TTH and especially with regard to the functions of the trapezius and the sternocleidomastoideus muscles affecting the neck and scapulae. Detailed interviews and specific measurements of physical activity using an accelerometer would have provided information on the activity habits in the two groups of girls, but was not applied in the present study. Boys were not included in this study, because too few of them had been diagnosed with a primary TTH when the study took place. As a result, determining whether our findings are also evident in boys would also be of interest.
Conclusions and practical implications
The results indicate a significant association between reduced neck-shoulder muscle strength and aerobic power together with increased pericranial tenderness and TTH in girls. This emphasises the value and need of exercise as good health promotion in the paediatric area. It also stresses the need for a follow-up study on the efficacy of patient education empowering enhanced physical exercising in paediatric headache management. Results from additional interventions studies would likewise aid in improving physical therapy. Families might also play an important role with regard to prevention by becoming involved in meeting the child's need for regular physical exercise. Much more exact and detailed research is needed in young girls and boys.
Clinical implications
• Reduced neck-shoulder strength and aerobic power are associated with TTH in girls. • Pericranial tenderness is positively correlated with headache frequency. • There is a need for examining the relationship between exercise deficits and TTH in girls. • The effect of patient education on enhanced physical exercising is a relevant topic for future research.
Footnotes
Acknowledgements
We would like to thank all the children and parents who took the time to participate in this study, and also to extend our appreciation to the school boards for allowing the schools to participate. We would like to thank research lab technician Hanne Andresen (HA), the Danish Headache Centre, Glostrup Hospital, for conducting all the testing. We are also grateful to the nursing and physiotherapy students, Christian Tilsted, Pernille Hansen, May Bang and Marianne Villadsen, who assisted in the testing procedures. Thanks are also due to statistician Claus Jensen, MSc, the Danish Ministry of Education and Children/Huge Consulting for closely supervising the statistical analyses. Finally, we would also like to thank Nancy Aaen, MA, for participating in the editing process. On request original data can be accessed by the Department of Paediatrics E, University of Copenhagen, Herlev Hospital, Denmark.
Funding
This study was financed by support from the Master Carpenter Jørgen Holm and Wife Elisa F. Hansen's Memorial Trust, the Beckett-Foundation, the Lundbeck Foundation, the Axel Muusfeldt's Foundation, the Dagmar Marshalls Foundation, the European Movement/V-Foundation and the Danish foundation TrygFonden.
Conflict of interest
The authors report no conflicts of interest.