
Abstract
Background and aim
There are variations of migraine prevalence in cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) among different regions of the world. Previous studies on Asian CADASIL patients have not provided detailed descriptions of the characteristics of their headaches. The aims of this study were to determine prevalence and characteristics of headaches and to investigate associations between headache and other clinical symptoms or brain magnetic resonance imaging (MRI) findings among homogenous group of patients having the same R544C mutation.
Methods
In this cross-sectional study, we enrolled 53 CADASIL patients with the R544C mutation between May 2010 and April 2011. We obtained the history of headache using a structured questionnaire and detailed interview. Other clinical features and brain MRI findings were also assessed for potential associations.
Results
Overall headache prevalence was 45.3% (24 patients). Among them, 21 patients (87.5%) were classified as having tension-type headache, followed by migraine (two patients) and unclassifiable headaches (one patient). Except for alcohol consumption, no significant associations were observed between the headaches and other clinical features or brain MRI findings.
Conclusion
Migraine was found in only 3.8% of CADASIL patients with the R544C mutation. Such a low prevalence of migraine may hinder clinical detection of CADASIL among ethnically Asian patients.
Introduction
Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) is one of the most common genetic cerebrovascular diseases involving the small arteries of the brain (1,2). It is caused by a mutation of the NOTCH3 gene on the short arm of chromosome 19 (3). Main clinical manifestations include repeated strokes, disturbances in cognitive function, migraines, and psychiatric symptoms. Migraine is the most common initial symptom, which is present in 22%–77% of CADASIL patients (4–6). The prevalence of migraine in CADASIL is slightly higher than that of the general population, and the majority (80%–90%) of migraineurs with CADASIL have migraine with aura (7). Although most recurrent headaches in patients with CADASIL are reported as migraine with aura, a small number of patients experience other types of headache (5). Interestingly, research from Asia has shown a lower prevalence of migraine ranging from 4% to 30% in Korean, Japanese and Chinese populations (8–11). The exact reason for this difference is unknown. Unfortunately, previous reports on Asian patients have not provided detailed descriptions characterizing CADASIL-related headaches, which might explain the variation of clinical presentations of CADASIL in different regions of the world. We have reported several unique aspects of CADASIL patients in our population, including high prevalence of hemorrhagic stroke and the presence of a prevalent mutation, namely R544C, thought to be the result of a founder effect (12,13). The purposes of the present study are to describe prevalence and characteristics of headaches and to investigate associations between the headache and other clinical symptoms or brain magnetic resonance imaging (MRI) findings within a group of CADASIL patients with the R544C mutation.
Patients and methods
Study design and patient selection
A cross-sectional study design was used. This study was conducted at Jeju National University Hospital, the only university hospital on Jeju Island. Jeju Island is located off the southern coast of the Korean peninsula and has a population of 550,000 people. Subjects in this study were CADASIL patients 18 years or older who were diagnosed with CADASIL by genetic testing. We excluded patients who refused prospective testing, or were unavailable for examination because of severe disabilities. Informed consent was given by all patients, and this study was approved by the local ethics committee.
Between May 2010 and April 2011, we collected histories of headache from CADASIL patients using a structured questionnaire and detailed interview. We assessed the onset, frequency (including changes in frequency with aging and following strokes), location, features and severity of headache. For associated symptoms of headache, we asked about nausea or vomiting, sensitivity to light or sound, and presence and type of aura. The questionnaire included questions on treatment status including frequency of medication use per month (see Supplementary data online). Headaches were classified into migraine, tension-type headache (TTH), and other headache according to the second edition of the International Classification of Headache Disorders (14). Migraines were further categorized into migraine without aura, migraine with aura, chronic migraine, or probable migraine, while TTH was designated as infrequent episodic TTH, frequent episodic TTH, chronic TTH, or probable TTH.
Clinical and neuroimaging assessment
Detailed clinical assessment and brain MRI protocols have been published previously (13,15). We assessed clinical symptoms associated with CADASIL including stroke, dementia, seizures, and psychiatric symptoms. Stroke was further categorized into transient ischemic attack (TIA), cerebral infarction, and intracerebral hemorrhage. Global cognitive function was assessed using the Korean version of the Mini-Mental State Examination (MMSE). Dementia was defined according to the National Institute of Neurological Disorders and Stroke-Association Internationale pour la Recherché et l’Enseignement en Neurosciences (NINDS-AIREN) criteria for vascular dementia (16). We looked for patterns in risk factors of vascular disease: namely hypertension, diabetes, hyperlipidemia, alcohol consumption, and smoking status. Hypertension was defined as a blood pressure of at least 140/90 mm Hg on two separate measurements or the use of an antihypertensive agent. Diagnostic criteria for diabetes mellitus were fasting blood glucose level of at least 126 mg/dl or the use of antidiabetic medications. Hyperlipidemia was defined as fasting total cholesterol more than 240 mg/dl. Smoking status was divided into two categories, with nonsmoker in one group and current or ex-smokers in the second. Alcohol consumption was measured as none, light (more than one drink per month and below two drinks per day), or heavy (more than two drinks per day). DNA testing was performed by polymerase chain reaction using peripheral blood collected from patients. All patients were examined for brain MRI at our center (1.5 Tesla system; Siemens, Sonata, Germany). We evaluated the severity of white-matter hyperintensity (WMH) lesions, the involvement of anterior temporal lobe (17), the number of cerebral microbleeds (18), and the number of lacunar infarcts (19). WMH volumes were measured by an experienced image analyst using volumetry (Analyze 8.1, Biomedical Imaging, Mayo Clinic, Rochester, MN, USA). The volume of WMH lesions was calculated automatically by multiplying the lesion area by the section thickness. WMH volumes were then normalized for total brain volume by dividing the individual WMH volume by the intracranial cavity volume (normalized WMH volume [nWMH]) (15).
Statistical analysis
Stata 12 (Stata Corp, 2011, College Station, TX, USA) for Windows was used for statistical analyses. Descriptive statistics was used to report the characteristics of the patients with CADASIL and their headaches. To investigate associations between headache and other clinical symptoms or brain MRI findings, the patients were first grouped according to the presence or absence of headache. For comparison of continuous variables between groups, we used the Student t test or Mann-Whitney U test. The differences between categorical variables were analyzed using the chi square test or Fisher’s exact test for comparison. We performed a logistic regression analysis based on bivariate analyses. Covariates entered the model for p values less than 0.25. In all analyses, a p value of 0.05 or less was defined as statistically significant.
Results
Characteristics of the participants
Clinical characteristics and brain magnetic resonance imaging features of 53 CADASIL patients.

CADASIL: cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy; MMSE: Mini-Mental State Examination; MRI: magnetic resonance imaging; IQR: interquartile range; WMH: white matter hyperintensity. Data are n (%) or mean ± SD or median with IQR. aWMH volumetry was unavailable on eight patients.
Characteristics of headaches
Of 24 patients who had headaches, one patient did not explain symptoms associated with headache. Otherwise, there were no other missing responses to the headache questionnaires. Sixteen patients (69.8%) had experienced headaches within one month before the interview. The most common age at onset of recurrent headaches was in the 50s (45.8%). Only two patients had developed headaches before their 40s. Almost 95% of headache patients reported at least one episode per month with the median number of headache episode per month being 2.5 (IQR: 1.5–4.75) Only two patients (8.3%) had headaches for seven to 14 days out of each month and three patients (12.5%) had headaches for more than 14 days per month. Eight patients (33.3%) reported more frequent headaches with advancing age. Only three patients stated that they had experienced decreased frequency of headaches with time. Fourteen patients (60.9%) reported that the duration of headache was less than 30 minutes, which resulted in diagnosis of headache as probable TTH or probable migraine because they did not meet the criteria for the duration of headache.
Characteristics of headache in 24 CADASIL patients.

CADASIL: cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy; IQR, interquartile range. Data are n (%) or median with IQR.
One patient did not answer these items.
At the time of the interview, nine patients (37.5%) were using pharmacological treatment for headaches. The duration of headache did not differ significantly between the patients with pharmacologic treatment and those without treatment. Nine patients (37.5%) with headache had experienced strokes and only one patient had the stroke before the onset of headaches. Of the eight remaining stroke patients, three stated that frequency of headache increased after stroke; five patients reported no change in their headache frequency after stroke. Out of the 24 CADASIL patients who suffered headaches, most patients (87.5%) were classified as TTH, followed by migraine (two patients) and unclassifiable headaches (one patient). Of TTH, the most common sub-classification was probable TTH, which was present in 14 patients (Figure 1). Among them, 12 patients were classified as probable TTH solely because the duration of headache was less than 30 minutes.
Classification of headache in 24 CADASIL patients with R544C mutation.
Comparison of clinical and brain magnetic resonance imaging findings of 53 CADASIL patients by headache.
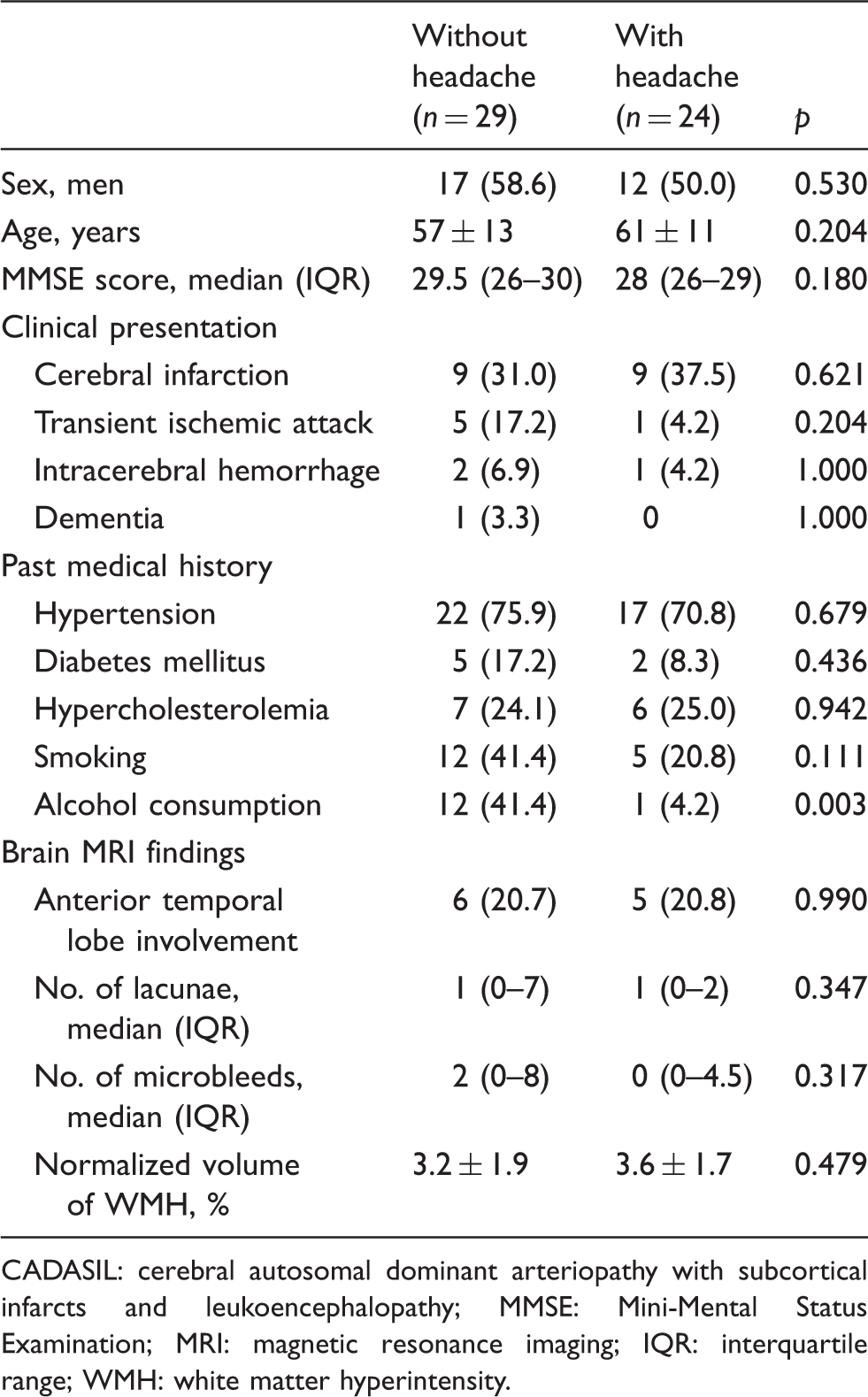
CADASIL: cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy; MMSE: Mini-Mental Status Examination; MRI: magnetic resonance imaging; IQR: interquartile range; WMH: white matter hyperintensity.
Bivariate and multivariable association between independent factors and headaches in 53 CADASIL patients.

CADASIL: cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy; OR: odd ratio; CI: confidence interval.
Discussion
Despite several reports that have mentioned the low prevalence of migraine in East Asian CADASIL patients, few attempts have been made to characterize headache symptoms and to evaluate associations with other clinical or neuroimaging findings among these patients. The main objectives of the present study were to describe the detailed characteristics of headaches using a structured questionnaire and to investigate association between headache and other risk factors among Korean CADASIL patients with the R544C mutation. Although headaches were reported in 45.3% of our patients, only two were classified as migraine. This result is consistent with previous reports on Korean, Japanese and Chinese patients with CADASIL (8–11). However, in the relative absence of migraine, other types of recurrent headaches appeared prevalent in our patients with CADASIL. The majority of these headaches were identified as probable TTH or frequent episodic TTH; together these types of headaches represented more than 80% of all reported headaches. Of the 14 patients who were classified as probable TTH, 12 patients showed headache durations of less than 30 minutes, which did not meet the criteria of TTH. Otherwise, headache cases were classified as frequent episodic TTH (11 patients) or chronic TTH (one patient). Patients with probable TTH have seldom reported classic features of migraine in the past, and since recurrent headaches typically started after patients were in their 40s, it is unlikely that instances of transformed migraine (now more commonly referred to as chronic migraine) were misclassified as probable TTH. A 2012 study reported that the one-year prevalence of all types of headaches in the general Korean population was 61.4% and the overall prevalence rates of migraine and TTH were 6.1% and 30.8% (20). Therefore, the overall prevalence of headaches in our patients with CADASIL does not appear to differ significantly from that of the general Korean population.
Studies have shown that migraines in the general population are overall less prevalent in Asia (1%–22%) than in Europe (10%–25%) or North America (9%–16%) (21). Possible explanations for varying migraine prevalence in different populations include methodological differences among studies, cultural differences in symptom reporting, variation in environmental risk factors, or race-related differences in genetic susceptibility to migraine. Stewart et al. indicated that race-related genetic differences may best account for this pattern by demonstrating a similar variation in migraine prevalence among Caucasians, African Americans, and Asian Americans in the United States (22). Following this explanation, the variation of migraine prevalence in patients with CADASIL may be a reflection of trends in the general population.
A patient’s history of migraine with aura and the involvement of the anterior temporal lobe in brain MRI are presently the two primary criteria used in differential diagnosis of CADASIL from sporadic small vessel diseases. The history of migraine with aura is important in clinical suspicion of CADASIL among patients who presented with clinical or neuroimaging features of small vessel diseases because migraine with aura is the most common initial symptom that is present in 22%–77% of CADASIL patients (4–6). In addition, WMH lesions are frequently found on brain MRI of CADASIL patients (23,24). Especially, WMH lesions at the anterior temporal lobe are characteristic in patients with CADASIL in contrast to sporadic ischemic WMH lesions. O’Sullivan et al. have reported that the sensitivity and specificity of WMH lesions on the anterior temporal lobe in CADASIL diagnosis were 90% and 100%, respectively (25). However, our data suggest that these indices may not be as robust for identifying CADASIL in patients of East Asian descent. Along with low prevalence of migraine with aura, the present study showed anterior temporal involvement in only 19.6% of our patients. A comparably low rate has also been reported in other studies involving Korean (23.1%) and Chinese populations (42.9%) (9,10). Furthermore, our study showed no significant difference in the frequency of anterior temporal lobe involvement between the patients with headache and those without headache. As pointed out by Pantoni et al., there is no single pathognomonic clinical or neuroimaging finding to distinguish CADASIL patients from sporadic small vessel diseases (26). The low prevalence of migraine with aura will make clinical detection of CADASIL more difficult among patients presenting with small vessel diseases in East Asian regions.
We found that alcohol consumption was significantly lower in patients experiencing recurrent headache. Previous reports show a trend of decreasing headache prevalence with increasing alcohol consumption (27). A positive association between alcohol consumption and frequent headache was found only in alcohol overusers. The 13 patients who reported drinking in our study indicated a light drinking habit. The significant association between headache and alcohol consumption is perhaps explained by the headache-precipitating effects of regular alcohol intake.
It is important to note the limitations of this study. First, although there is little relationship between phenotype and genotype in CADASIL, our findings may not be applicable to other populations of CADASIL patients who do not have the R544C mutation. Second, we could not assess long-term changes in headache characteristics because of the cross-sectional study design. It is possible, particularly among those reporting infrequent headaches, that patients may incorrectly recall details about the initial phase or other features of headache. Third, CADASIL patients with severe disability or death due to advanced illness were excluded because they could not complete the headache questionnaire. Therefore, our results do not reflect headache or neuroimaging trends in patients with severe disability or advanced cognitive dysfunction.
Clinical implications
Migraine was found only in 3.8% of Korean cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) patients having the R544C mutation. Low prevalence of migraine with aura will make clinical detection of CADASIL more difficult in East Asian patient groups than in other ethnicities.
Footnotes
Funding
This work was supported by a research grant from the Hyocheon Academic Research Fund of Jeju National University in 2010.
Conflict of interest
None declared.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.