
Abstract
Background
Red ear syndrome (RES), first described by Lance in 1996 in an adult series, may be primary or associated with headache syndromes, upper cervical disorders or vascular anomalies. Clinically the disease is characterised by recurrent episodes of reddening and burning pain in the auricle, usually elicited by different triggers. The prevalence of RES in the paediatric age group remains poorly understood. Several therapeutic approaches have been tried with heterogeneous clinical response.
Case results
We report a paediatric patient suffering from primary RES associated with debilitating cochleo-vestibular symptomatology causing severe discomfort. Three years after the disease onset, the patient also developed headache, with clinical features of migraine.
Discussion
The temporal and spatial association could suggest shared pathogenetic features between neurological (cochleo-vestibular) and vascular (red and burning ear) symptomatology, likely related to trigeminal autonomic reflex activation, although further studies are required for full comprehension of RES pathogenesis.
Introduction
Red ear syndrome (RES) was first described by Lance in adult patients more than 15 years ago; these patients were also suffering from temporomandibular joint (TMJ) dysfunction, trigeminal neuralgia and thalamic syndrome (1). Subsequently more than 50 cases have been published, mostly in adulthood. Clinically, the disease is characterised by recurrent attacks of redness and burning pain in the ear, usually unilateral, often triggered by heat exposure, physical activity, touching or rubbing the ear or neck movements. Although the pathogenetic mechanisms of RES still remain incompletely defined, the disease may be primary or secondary to several disorders, such as facet joint spondylosis, cervical root traction, herpes zoster virus infection, Chiari I malformation and posture-related kinking of the vertebral artery (2). An association with primary headache syndromes including migraine and chronic paroxysmal hemicrania has been reported in adult patients and, more recently, also in a paediatric series (3). An activation of cranial autonomic pathways has been suggested as a common pathogenetic mechanism for both disease types. Many therapeutic approaches have been attempted with different results, especially nonsteroidal anti-inflammatory drugs (NSAIDs), as well as antihypertensive and antiepileptic drugs. Herein we report a paediatric patient with a severe life-limiting form of RES associated with cochleo-vestibular symptoms, during a long-term follow-up period.
Case report
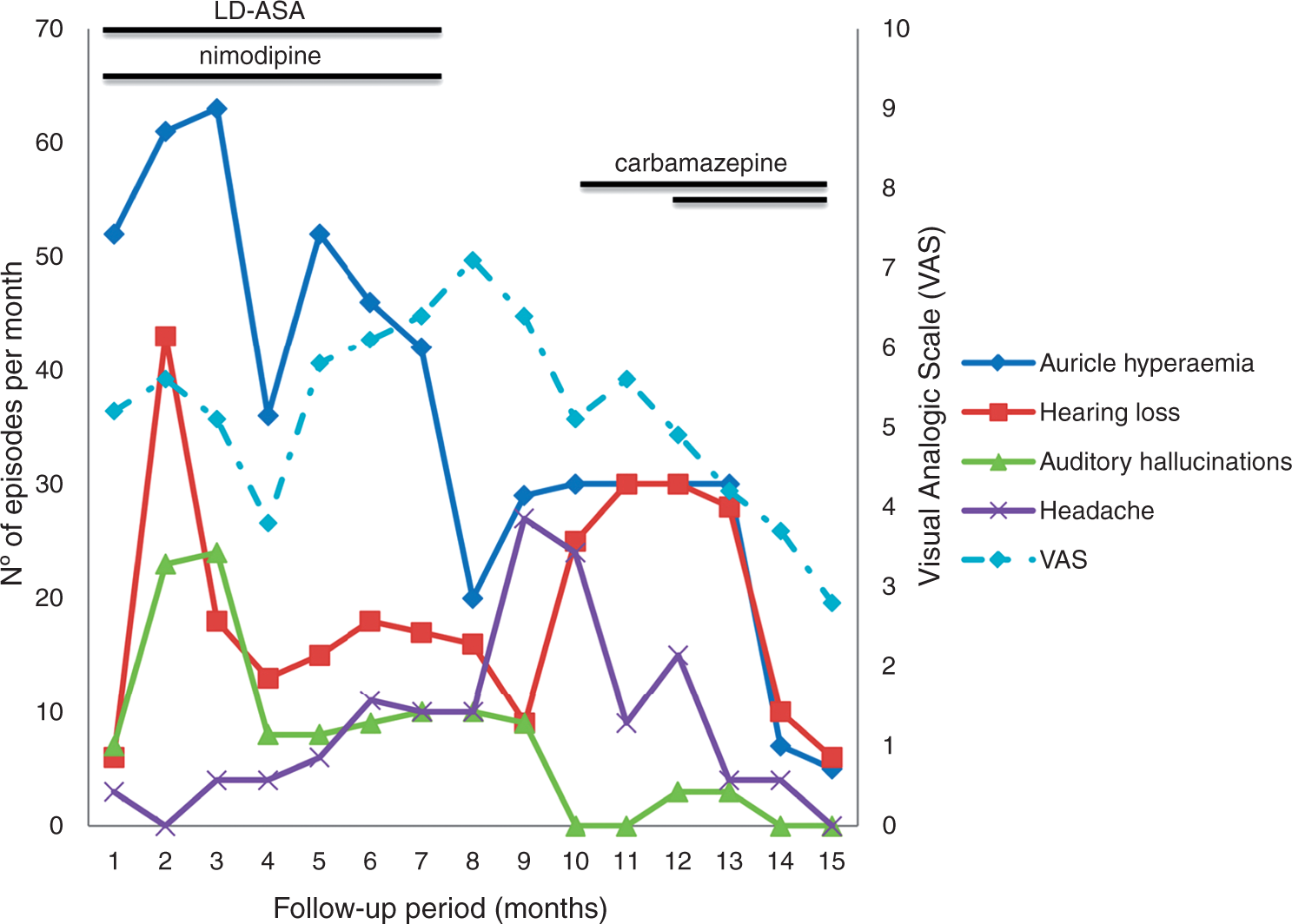
A 10-year-old boy was referred to us because of a four-year history of relapsing attacks of reddening in one ear, associated with burning sensation, pain and mild oedema (Figure 1). The attacks occurred one to two times daily, were always unilateral, albeit alternating in side location and lasted from 15 minutes to three hours. The episodes were either spontaneous or triggered mainly by heat exposure, especially when he used the hairdryer. Furthermore, pain was so severe that he couldn’t lay his head on the pillow during a night attack. There was no family history of primary headaches or autoimmune diseases. Patient history was also negative for traumatic events or TMJ dysfunction. Six months after the disease onset, the pain and reddening flare-ups were associated with tinnitus, transient hearing loss, auditory hallucinations, such as explosions, and vertigo. The child was evaluated by adult rheumatologists who suspected erythromelalgia and prescribed low-dose acetylsalicylic acid (75 mg/day). Due to inefficacy, nimodipine (20 mg/day) was added to the therapy. Unfortunately, RES-related symptoms remained unchanged over seven months; furthermore, the patient developed headache with the appearance of migraine episodes, without aura, not always associated with ear symptoms. Then he was admitted to our Institute. Acute-phase reactants, haemogram and autoantibody (antinuclear antibodies (ANAs), anti-neutrophil cytoplasmic (ANCA)) assay were negative. The neurological and otolaryngological assessment with electroencephalography, pure tone and vocal audiometry, tympanometry, stapedial reflex and auditory brain stem response were within the normal ranges. Cervical and brain angio-magnetic resonance imaging (MRI) pointed out a tortuous course of the vertebro-basilar junction without any other significant anatomic abnormalities. Finally he also underwent a psychological assessment which pointed out cognitive impairment mainly restricted to verbal comprehension (probably related to the severe life-limiting symptoms he reported), attention deficiency and phobic behaviour (the child felt booming in his ear or presence of dust or insects inside the ear). In agreement with the parents and the patient, we advised keeping a diary to record the duration and frequency of main symptoms exhibited by the child: namely, they were i) auricle hyperaemia, ii) transient hearing loss, iii) auditory hallucinations and iv) headache. Considering the severe life-limiting symptoms he described, the degree of discomfort associated with the attack was recorded on a visual analogue scale (VAS), going from 0 (no discomfort) to 10 (maximum discomfort), to allow a more objective and prospective evaluation of the clinical course. Seven months after admission, we documented the inefficacy of low-dose acetylsalicylic acid and nimodipine on RES and migraine; hence these drugs were stopped. Because of neurologic features of the pain related to the RES attacks, we scheduled a treatment with carbamazepine (CBZ) at a starting dose of 50 mg/day without convincing clinical amelioration. Hence, the CBZ dosage was increased to 100 mg/day. In the following months the patient experienced a progressive reduction of headache, auditory hallucinations, hearing loss and auricle hyperaemia, as recorded by his parents. Notably, today the child requires no more use of local ice application to induce remission of attacks (Figure 2).
Erythema of the left ear during a typical attack of red ear syndrome (RES). Disease flares during 15-month follow-up period; double strand means double dose, dotted line refers to mean values of VAS about patient discomfort during the attack. LD-ASA: low-dose acetylsalicylic acid; VAS: visual analogue scale.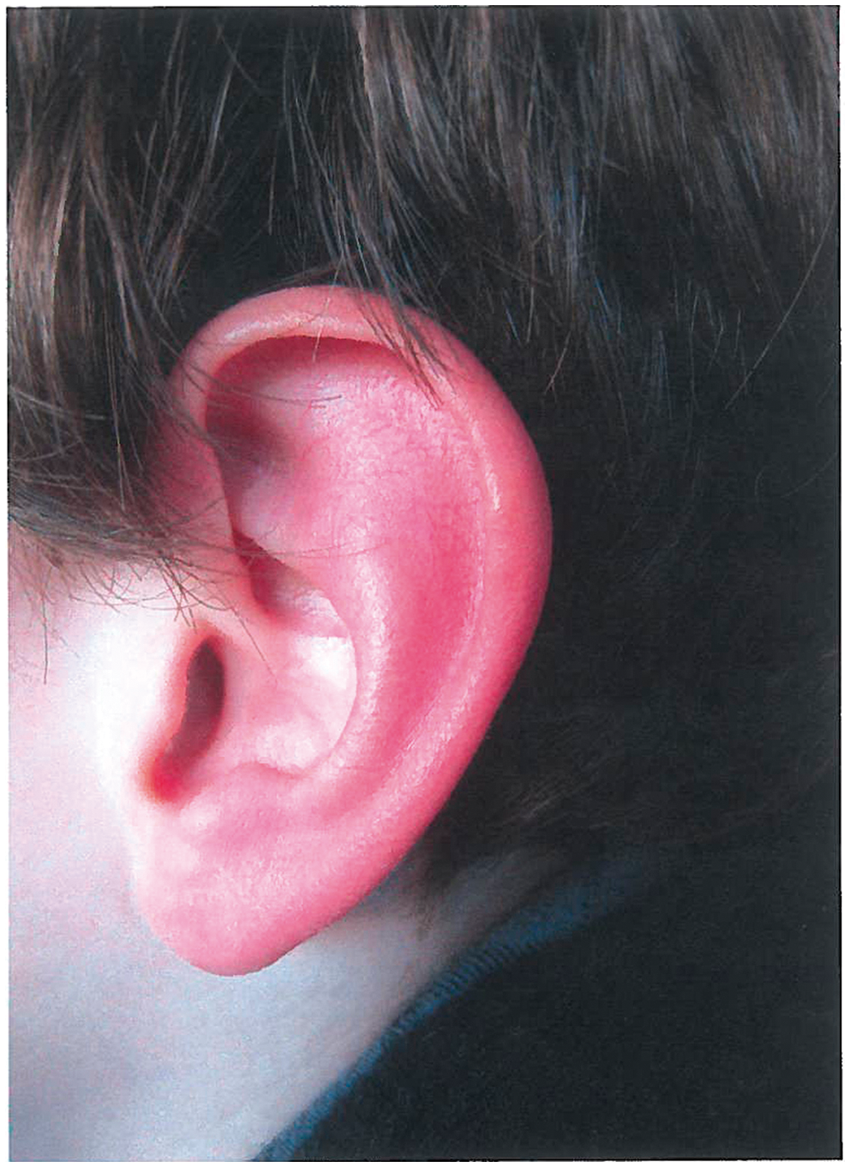
Discussion
RES is a recently identified neurological disease which may be primary or secondary to other diseases such as upper cervical disorders, anatomic malformations or TMJ dysfunction; this latter form seems more frequent in adult patients. So far no definitive data are available about RES prevalence in the paediatric population, being likely misdiagnosed. The pivotal clinical features of the disease are recurrent painful attacks of redness and burning pain in one ear, unilateral but sometimes alternating in side location, occasionally associated with auditory dysesthesias. During interictal periods the patients are usually asymptomatic. This intermittent course of the disease represents itself as a main clinical feature in differential diagnosis with other diseases such as relapsing polychondritis, streptococcal infections and granulomatous diseases. As previously reported in the literature, it seems that in adult patients the syndrome is more frequently due to other abnormalities, whereas in children RES is commonly primary and usually associated with migraine (2). Namely, Raieli et al. demonstrated that in paediatric patients the syndrome could be found with higher frequency in subjects suffering from migraine than in those affected by primary headache (3); this finding may be useful in paediatric ages for the diagnosis of migraine when a clinical history is more difficult to obtain and evaluate. Our patient was referred to us just for attacks of reddening ears associated with debilitating cochleo-vestibular symptoms, never reported previously in the literature. Indeed auditory hallucinations, transient hearing loss and vertigo were serious life-limiting symptoms as well as pain and reddening of the auricle. Since cochleo-vestibular symptoms occurred concurrently with attacks of red and burning ears, we may consider them as a part of RES spectrum. In addition the pathogenesis of cochleo-vestibular involvement in our patient remains still poorly understood.
It is noteworthy that a few cases of atypical forms of RES have been reported in the literature and have been described as RES plus (4). They were mostly clinically characterised by extra-auricular symptomatology, such as nasal blockage, tearing and conjunctival injection, all signs referred to trigeminal autonomic cephalalgia (TAC). Although our patient showed atypical clinical features of RES, they were all auricular related, so the diagnosis of RES may be formulated. The child also developed cognitive impairment focused on verbal comprehension, probably related to the aforementioned life-limiting symptoms. In our patient RES began as isolated and headache arose over three years later: this finding suggests that RES paediatric patients need a long-term observation focused on the prompt diagnosis of headache, since, as reported by Raieli et al., RES and migraine are strictly associated (3). Admittedly, in our anecdotal experience, RES has been a heralding symptom of migraine. From the first observation we planned to carefully collect all the symptoms the child described as associated with RES attacks that he recorded in his diary to prospectively evaluate the efficacy of the ongoing treatment and to compare it with different therapies, as there is no global consensus about RES treatment. At present many therapies have been tried: among them, NSAIDs as well as acetylsalicylic acid, ibuprofen, indomethacin for the painful symptoms; beta blockers such as propranolol for peripheral vascular dysfunction; amitriptyline and verapamil when headache was present; antiepileptic drugs such as gabapentin and topiramate for the treatment of neuropathic pain and a bite splint for TMJ disorders (2). The surgical blockade of the greater auricular nerve with anaesthetic and steroid mix or botulinum toxin has been attempted too (5,6). We decided to treat our patient with CBZ as we considered all symptoms related to a dysfunctional neuronal activation: furthermore, the drug is easy to use in paediatric ages. It remains unclear if the documented clinical improvement might be attributed to CBZ treatment or to the intermittent course of the disease. So far, the underlying pathophysiology of RES still remains unclear and different hypotheses have been proposed; however, the common pathophysiological mechanism seems related to the activation of the trigeminal autonomic reflex (2), probably due to pathological lowering of the axonal firing threshold. As is known, pharmacodynamic studies showed that CBZ acts by modifying Na+ conductance in excitable membranes, thus limiting sustained high-frequency neuronal discharges (7). Hence this could be hypothesised as the way CBZ acts on neurological and vascular RES symptoms. A longer follow-up period is needed for a better understanding of the patient’s clinical development, and more studies are required for full pathophysiological comprehension of RES.
Clinical implications
We described a paediatric patient afflicted by red ear syndrome (RES), associated with severe cochleo-vestibular symptomatology, never reported before in the literature. It is very important to follow up paediatric patients suffering from RES in absence of headache because it is likely that they’ll complain of headache afterwards. All RES symptoms could share common pathogenetic features probably related to trigeminal autonomic reflex activation.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.