
Abstract
Background: Previous studies have suggested a relationship between ‘red ear syndrome’ (RES) and pediatric migraine. Aims of this study were (i) to assess the frequency, specificity and sensitivity of RES in a population of pediatric migraineurs and (ii) to establish the pathophysiological mechanisms of RES associated with migraine.
Methods and results: A total of 226 children suffering from headache (aged 4–17 years) were enrolled. One hundred and seventy-two (76.4%) were affected by migraine, the remaining 54 (23.6%) by other primary headaches. RES was followed significantly more frequently by migraine (23.3%; p < .0001), and was characterized by high specificity and positive predictive value (96.3 and 95.3%, respectively). According to the univariate statistical analysis, RES showed a statistically significant association with male gender, throbbing quality of the pain, vomiting and phonophobia. It was confirmed by a multivariate stepwise logistic regression model only for the throbbing quality of the pain, vomiting and male gender.
Conclusions: Our study showed that (i) in children, RES is a highly specific sign for migraine. In addition, the evidence of an association of RES with some migraine features partially provoked by the parasympathetic system supports the hypothesis of a shared pathophysiological background (e.g. via the activation of the trigeminal-autonomic reflex).
Keywords
Introduction
Red ear syndrome (RES) was first described by Lance in 1996 (1). He reported 12 patients with recurrent attacks of unilateral ear pain or burning associated with erythema of the ipsilateral ear. In addition, he distinguished between idiopathic and secondary forms, and attributed the secondary ones to a range of disorders, including cervical arachnoiditis or spondylosis, traction injury of upper cervical roots, atypical neuralgias, temporomandibular joint dysfunction or thalamic syndrome. Following his description, almost 60 new cases of RES have been referred to in the literature (2). However, we were the first to report a possible association between RES and migraine (3), and more recently other authors hypothesized a crossover between RES and other primary headaches, such as trigeminal autonomic cephalalgias (TACs) (4,5). There are still few data, nevertheless, about the frequency of the RES in the general population, its semeiological value or its relationship with primary headaches. The aims of this study were to assess the prevalence of RES in a clinical sample of children affected by primary headaches and to establish its semeiological usefulness in the differentiation of migraine from other primary headaches. Moreover, we evaluated the possible association between RES and a series of typical migraine clinical features. Recent studies have shown that signs and symptoms of migraine are caused, at least in part, by different pathophysiological mechanisms (6,7). Therefore, we surmised that investigating the migraine clinical features correlated with the RES and speculating on the reasons for this correlation could be a useful contribution to the understanding of RES associated with migraine.
Methods
Patient population
A sample of 226 patients (115 male, 111 were female [aged 4–17 years]) were enrolled in this study. The patients were consecutively examined between December 2004 and November 2005 in our outpatient service for diagnosis and treatment of headache (in the Child and Adolescent Neuropsychiatry Department). Informed consent was obtained from parents; assent was obtained from child and teen participants.
Diagnostic investigations
A semi-structured interview about the main characteristics of his or her headache attacks was administered to each patient. Briefly, the interview, which had been validated in a previous study (8), covered biographical data, age, sex, family headache history, frequency and duration of the attacks, duration of migraine, quality and intensity of the pain, the influence of physical activity, occurrence of nausea, vomiting, photo-, phono-, and osmophobia, and the occurrence of aura and allodynia. General and neurological examinations were carried out in all children. Other diagnostic investigations (e.g. blood tests, neurophysiological and neuroimaging studies, other specialist visits) were performed if required. A short supplementary questionnaire investigating the presence of RES and its characteristics was administered to all children and their parents at the same time. The questionnaire explored (i) the occurrence of a reddened ear with burning ear pain before and/or during most of the headache attacks; (ii) the unilateral or bilateral localization of RES; and (iii) the duration of the whole episode. Patients were classified according to the 2004 International Headache Society (IHS) criteria (9).
Exclusion criteria
Those affected by secondary headaches were excluded from this study; therefore, our sample consisted only of children suffering from primary headaches.
Statistics
Chi-square and t-tests were used to compare the nominal and the continuous variables, respectively. In addition, sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated for RES. We also performed a logistic regression analysis to study the relationship between RES and other typical migraine features. Variables significantly associated with RES at the univariate analysis were included in a multivariate stepwise logistic regression model. A p value < .05 was considered statistically significant. Data were processed using SAS software (version 9.1.3 for Windows) (SAS, Cary, NC, USA).
Results
Two hundred and twenty-six children (115 males, 111 females, aged 4–17 years, mean ± standard deviation [SD] 11.1 ± 3.05) were enrolled in this study. In total, 172 children (76.4%) (92 males, 80 females) were found to be affected by migraine with/without aura, and 54 (23.6%) by other primary headaches (primary stabbing headache, episodic and chronic tension-type headache). RES was observed in 40 patients in the migraineurs’ group (23.3% [confidence interval{CI} 17–29.5]), and in only two patients in the group suffering from other primary headaches (3.7% [CI 0.6–6.8]), thus occurring significantly more frequently in migraine than in the other primary headaches (p < .0001). Hence, in the course of a migraine attack, RES was characterized by high specificity (96.3%) and PPV (95.3%) values versus low sensitivity (23.25%) and NPV (28.3%).
Features of RES in association with pediatric migraine
Features of red ear syndrome in children with migraine

RES = red ear syndrome.
Relationship between RES and migraine clinical features (univariate analysis)
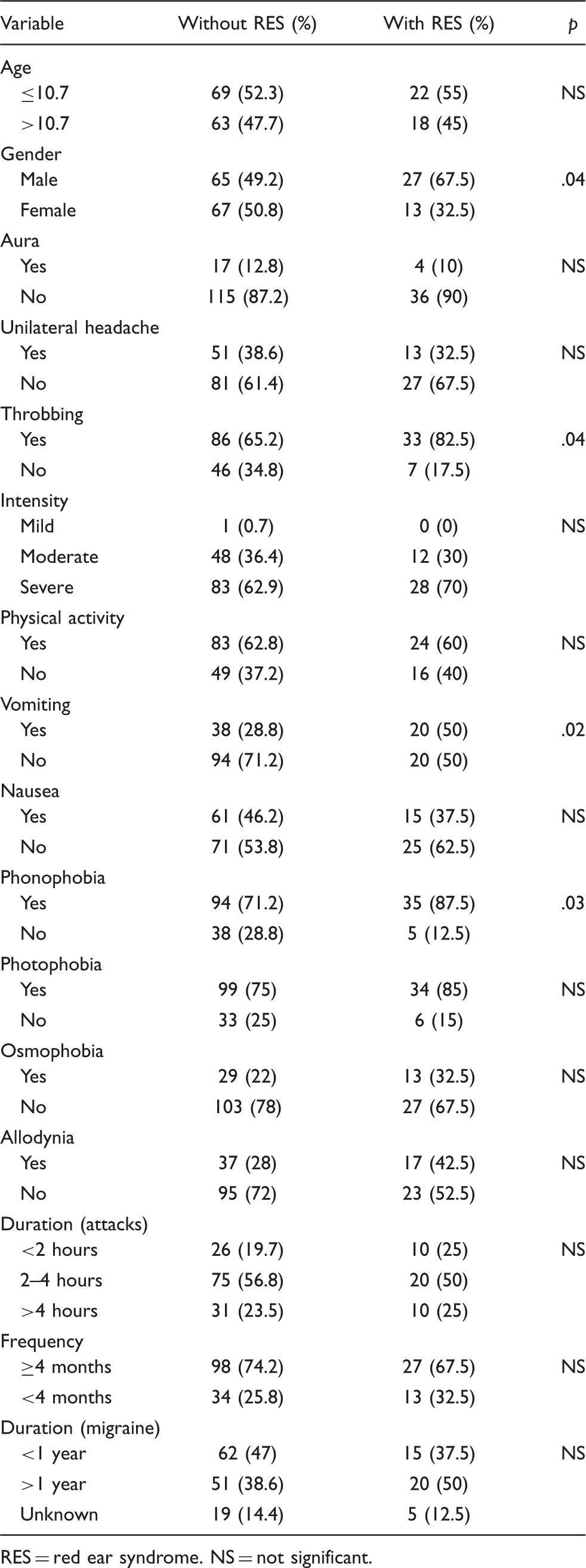
RES = red ear syndrome. NS = not significant.
Relationship between RES and migraine clinical features (univariate/multivariate analysis)

RES = red ear syndrome, CI = confidence interval, ORa = adjusted odds ratio.
Discussion
Since Lance’s initial description (1), RES has been considered a rare syndrome often associated with primary headaches, especially the forms characterized by a relevant autonomic dysfunction (e.g. TACs) (10). Nevertheless, with the exception of our preliminary findings (11), no new data has been published about the prevalence of RES either in primary headache sufferers or in the general population. In addition, the pathophysiological explanation of RES during a headache attack is only hypothetical, and physicians do not really know the potential usefulness of this sign as a diagnostic clinical marker. The present study evaluated the prevalence of the RES in young migraine sufferers. This is an interesting issue for several reasons. First, because findings from our 2002 survey (2), together with clinical experience gained in the subsequent years, showed us that RES is rather frequent in children affected by migraine. Moreover, in children, some typical migraine characteristics (e.g. duration, lateralization, quality of pain, associated symptoms) are less evident than in adult migraine sufferers, and a clinical history is more difficult to obtain and evaluate. Therefore, because of our hypothesis of a strong association between migraine and RES in children, RES could be a very useful objective clinical sign in distinguishing migraine from other primary headaches (e.g. tension-type headache). Finally, the discovery of a possible association between RES and migraine could yield a clue about the pathophysiology of migraine.
In our sample, about 20% of children affected by migraine had RES during migraine attacks. In addition, there was a statistically significant prevalence of RES in migraine as opposed to the other primary headaches. RES had high specificity and low sensitivity as a diagnostic marker for migraine, similarly to osmophobia (12,13), which has also been proposed as an additional migraine diagnostic marker. However, physicians can inquire into the occurrence of the RES more easily than osmophobia, and parents can obtain photographs and show them to the pediatrician or to the pediatric neurologist. Besides, the present study showed that RES and osmophobia are seldom associated in the same child. Therefore, because of the high diagnostic specificity of both of these features, the development of an ad hoc questionnaire assessing both these clinical features at the same time could improve our ability to diagnose migraine.
The pathophysiology of RES and its relationship with the mechanisms underlying a migraine attack remain still unknown. To this end, some notions about innervation and vascularization of the ear should be considered.
Innervation and vascularization of the ear
The ear lobe is innervated by the greater auricular nerve (branching from the 2nd and 3rd cervical roots), whereas the auriculotemporal nerve (from the third trigeminal division) provide sensory innervation to the anterosuperior aspect of the ear. Moreover, the trigeminal nerve also provides the sensory innervation of the auricular arteries (branches of external carotid artery), supplying the blood to the ear. These vessels are richly innervated by both sympathetic (vasoconstrictor) and parasympathetic (vasodilator) nerves. Therefore, we may hypothesize that, during migraine episodes, RES can be provoked by (i) a direct activation of the trigeminal fibers innervating the ear (trigemino-vascular mechanism) (14); (ii) a parasympathetic activation (i.e. a trigemino- or a cervico-autonomic reflex), (4,10); or (iii) a sympathetic inhibition. In order to understand which one/ones of these pathophysiological mechanisms could represent the best explanation of the observed relationship between RES and migraine, we analyzed in the detail the shown association between RES and some typical migraine features from a pathophysiological perspective.
Red ear syndrome and throbbing pain
The positive correlation between RES and throbbing pain was somewhat foreseeable. Various mechanisms have been proposed to explain the throbbing quality of pain in the course of migraine attacks. For example, pain has been ascribed to the peripheral sensitization of the first-order afferent neurons, which could increase the throbbing quality of the arterial vessels’ vascular tone (6,7). In this case
Red ear syndrome and vomiting
Vomiting is another clinical feature of migraine shown to have a significant correlation with RES. Vomiting is a very useful clinical sign in differentiating migraine from other primary headaches, especially tension-type headache. It is triggered by the activation of the vomiting center. This area receives important inputs from the vagal sensory pathways and, when activated, induces vomiting via stimulation of the salivary and respiratory centers and a vagal output to the pharyngeal, gastrointestinal and abdominal muscles (22,23). The positive correlation between RES and vomiting was consistent with these findings, and could be explained by the trigeminal-parasympathetic reflex, which is common to both these clinical features.
Red ear syndrome and male gender
The hypertonicity of the parasympathetic system could also explain the greater prevalence of RES in our male patients. In fact, a recent study by Slater et al. (24) showed that vomiting and nausea are more common in the male than in female migraineurs, and according to this author this is probably due to the direct involvement of the parasympathetic system
Red ear syndrome and phonophobia
Phonophobia turned out to be correlated with RES only according to the univariate analysis, but lost statistical significance in the multivariate analysis, perhaps indicating that phonophobia is associated with RES more weakly than are throbbing pain, vomiting or male gender. Actually, as it has been clearly shown in a recent paper (25), phonophobia is usually correlated with parasympathetic-related unilateral autonomic signs in patients affected by migraine. Furthermore, while the brain cortex activation is mandatory during photophobia, on the contrary, phonophobia requires the involvement of subcortical circuits, which are located in the brain stem, in a sort of “anatomophysiological contiguity” with other subcortical structures involved in the pathogenesis of the migraine attack and/or of the unilateral/bilateral autonomic signs (18,25).
Conclusions
RES showed an association with some parasympathetic-related migraine features, whereas we did not find a significant statistical correlation with other clinical features that do not require a direct involvement of the parasympathetic nervous system (e.g. an increase of pain with physical effort, allodynia, aura). Therefore, in our opinion, the findings of our study support the role of the trigeminal-autonomic reflex in the pathogenesis of RES in the course of a migraine attack. Moreover, this assumption is consistent with the observation that RES is a rather frequent clinical sign in primary headaches characterized by a relevant autonomic involvement (4,6,10).
A possible objection to the hypothetical relationship between RES and other parasympathetic-related migraine features may come from the observation that in our sample, child migraine with RES did not showed the RES in association with every migraine attack, but often sporadically. However, we believe that this observation could be explained by the so called “modulary theory” of headache proposed by Young et al. (26). This theory suggested that “groups of neurons, called modules, become activated to produce each symptom of a primary headache disorder and that each module is linked to other modules that together produce an individual’s headache”. Modules may be anatomically or functionally linked to each other and may be activated in a characteristic manner in an individual. Each module can be activated to a different degree and the level of symptoms may correlate with the degree of activation of the respective module. We propose that RES represents a clinical sign supporting this theory because it can be associated with or dissociated from a migraine attack in a single patient; it can be observed either before or during the attack, and it can be present in association with signs and symptoms that require the involvement of the autonomic nervous system.
To obtain a definitive confirmation of our model, we need further prospective studies regarding the correlation between RES and local autonomic signs during migraine, and a more systematic analysis of the anatomo-physiological background. There are also some limitations to consider. First, the use of a retrospective analysis methodology, especially in the developmental age, might influence the effective prevalence of the RES in the course of migraine. However
Another possible limitation is the lack of a systematic analysis of local autonomic symptoms. In fact, we performed a retrospective analysis and, if not quickly referred, some autonomic symptoms (e.g. miosis, ptosis, lacrimation or unilateral nasal obstruction) could be easily neglected, especially in children.
Finally, our study pertains to the developmental age, and therefore its results cannot be generalized to the adult migraineurs’ population. We do not know the real prevalence of RES in adulthood, and experts know that migraine features usually change, at least in part, when the young migraine sufferer becomes an adult.
In conclusion, our study shows that (i) in the pediatric age group, the RES is a rather frequent clinical sign during headache; (ii) in the group of primary headaches, it is more frequent during migraine; and (iii) it is a highly specific sign of a probable parasympathetic hyperactivation.
We believe that the presence of RES could be useful to identify a specific subtype of migraine in the near future, and it will probably have many implications for diagnosis and treatment of migraine.