
Abstract
Objective
Based on the capacity of the blood-resident enzyme glutamate oxaloacetate transaminase (GOT) to metabolize blood glutamate, our aim was to study the association of GOT activity with serum glutamate levels and clinical parameters in patients with migraine.
Methods
This case-control study included 45 episodic migraine patients (IHS 2004 criteria) and 16 control subjects. We analyzed glutamate and GOT activity in peripheral blood samples obtained during interictal periods and migraine attacks (n = 15). Frequency, severity, and duration of attacks and time of evolution were also recorded.
Results
Migraine patients showed lower GOT activity than controls (15.2 ± 2.9 vs. 18.7 ± 3.8 U/l) and higher levels of glutamate (153.7 ± 68.6 vs. 121.5 ± 59.2 μM) (all p < 0.05). A negative correlation was found between GOT activity and glutamate levels (r = −0.493; p < 0.0001) in interictal periods; however, this negative correlation was lost during attacks (r = −0.026; p = 0.925). During attacks, we found a positive correlation between the time elapsed from attack onset and glutamate levels (r = 0.738; p < 0.0001), but not for GOT activity (r = −0.075; p = 0.809).
Conclusions
Migraine patients showed reduced GOT activity and increased levels of blood glutamate levels as compared to control subjects. Furthermore, a negative correlation was found between GOT activity and glutamate levels in interictal periods.
Introduction
Migraine is a neurobiological disorder that affects 14.7% of Europeans, and its attacks manifest themselves from childhood to old age, with a decline among women during the postmenopausal years (1). Although the molecular mechanisms of migraine are not completely understood, it has been suggested that glutamatergic homeostasis is involved (2–5). An excessive glutamatergic signal induces an over-activation of N-methyl-D-aspartate (NMDA) receptors, which seems to be implicated in the triggering, propagation, and duration of cortical spreading depression (CSD) (5). Furthermore, NMDA-mediated glutamatergic transmission is probably implicated in the activation of the trigeminovascular system (6) and may cause the clinical symptoms of migraine attack and central sensitization (7). In this regard, NMDA receptor antagonists have been used as the most effective compounds for CSD suppression in experimental models (8); however, their use in humans has failed, mainly because of unacceptable side effects (9).
The critical role of glutamate in migraine has led some authors to suggest that systemic modifications of blood glutamate levels could reduce the excessive glutamatergic signal in the brain and therefore be used as a potential prophylactic treatment against migraine attacks (2). In line with this hypothesis, we and others have recently demonstrated that a decrease of blood glutamate levels leads to a larger natural glutamate gradient from brain to blood, which facilitates the decreases of extracellular levels of brain glutamate inducing a neuroprotective effect after ischemic insults (10,11). Reduction of blood glutamate is induced through the activity of the blood-resident enzyme glutamate-oxaloacetate transaminase (GOT), which catalyzes the reversible transformation of oxaloacetate and glutamate to aspartate and α-ketoglutarate (see Teichberg et al. (12) and Campos et al. (13) for review).
Based on the ability of GOT to metabolize blood glutamate, we aimed to study the association of GOT activity in blood with serum glutamate levels and clinical parameters in patients with migraine.
Methods
Study population
This was a case-control study including consecutive episodic migraine patients (n = 45) with (MA) (n = 12) or without aura (MWA) (n = 33) attending a headache clinic at a tertiary hospital, in whom migraine was diagnosed by a neurologist according to the International Headache Society criteria (14) and healthy control subjects (n = 16) without migraine or other type of headache, matched by gender and age. All subjects were ≥18 years old. Control subjects were recruited from the hospital and university staff, students, and general population. Clinical variables were recorded, and glutamate and GOT activity levels were determined. The period of recruitment was from June 2007 to November 2009.
Exclusion criteria were the following: 1) high blood pressure (known high blood pressure or two measurements greater than 140/90 mm Hg) (3 patients); 2) coronary disease (coronary lesions 50% determined by angiography, myocardial infarction, angina pectoris, or coronary recanalization) (0 patients); 3) diabetes mellitus (known diabetes mellitus or two fasting serum glucose determinations 126 mg/dl) (2 patients); 4) hypercholesterolemia (pharmacologically treated or fasting serum cholesterol 200 mg/dl) (1 patient); 5) infectious diseases (0 patients); 6) chronic inflammatory conditions (0 patients); 7) severe systemic diseases (0 patients); 8) oligomenorrhea, polymenorrhea, or polycystic ovarian syndrome (1 patient); 9) pregnancy or lactation (0 patients); 10) obesity (body mass index 35 kg/m2) (2 patients); 11) smoking habit (within the previous 12 months) (4 patients); 12) recent consumption of vasoactive drugs (four times the medium half-life of the active substance) (4 patients), and 13) hepatic diseases or treatments associated with transaminasemia (0 patients). No patient was receiving preventive treatment for any of these conditions.
Standard protocol approval, registration, and patient consent
The study was approved by the Research Ethics Committee of Servizo Galego de Saúde. All patients and control subjects provided written informed consent.
Study protocol
After a screening visit, eligible subjects were invited to perform a blood sample extraction. Patients were headache free from the previous 72 to 24 hours after the visit. If a migraine occurred within the first 24 hours, clinical measurements and blood extraction were repeated in another headache-free period. Subjects had not previously consumed anti-inflammatory or analgesic medication. In migraineurs with headache attack who visited the hospital within the first 24 hours from symptom onset, complete protocol was repeated again. Clinical measurements for control subjects and patients during the headache-free period were performed between 10:00 and 11:00 a.m. in a quiet, temperature-controlled room (22–24℃) by a single observer. Patients were admitted to the clinic during a migraine attack, and the duration of headache from onset was recorded. Symptomatic treatment was allowed after the study protocol was completed.
Clinical variables
Demographic and clinical data were recorded, including age, gender, type of migraine (MA or MWA), frequency of attacks, intensity of headaches (no effect on daily activities, pain limiting common tasks, or migraine preventing work), duration of attacks (four to eight, nine to 24, and 25–72 hours), and duration of the disease (years) (15). Clinical parameters of migraine were considered as an average of the patient’s episodes.
Laboratory tests
Blood samples were collected in chemistry test tubes, centrifuged at 3000 rpm for 15 minutes, and immediately frozen and stored at −80℃. Serum glutamate levels were determined by means of a Glutamate Assay Kit (Abnova, Taipei City, Taiwan). GOT activity was measured using an automated auto-analyzer (ADVIA 2400, Bayer Diagnostics, Leverkusen, Germany). The intra-assay and interassay coefficients of variation were 6.7% and 9.9% for glutamate, and 2.1% and 4.5% for GOT activity, respectively. Determinations were performed in an independent laboratory blinded to clinical and neuroimaging data.
Data and statistical analysis
Sample size was calculated with a precision level of 5%, confidence level of 95%, and test strength of 80% in order to detect a between-group difference of 20% in glutamate levels. Sample size was determined using EPIDAT software (http://dxsp.sergas.es/ApliEdatos/Epidat/cas/default.asp).
Results are expressed as percentages for categorical variables and mean (SD) or median (quartiles) for continuous variables, depending on the normal or not normal distribution of data. For all comparative analysis we have considered the following variables: serum levels of glutamate and GOT activity.
Differences between migraineurs and control subjects were analyzed using the Student t test. Differences among groups of the same population were determined by analysis of variance. Correlation between variables of the same group was calculated with regression lines with a 95% confidence interval. The Pearson coefficient for continuing variables (duration of disease, glutamate, and GOT activity levels) and the Spearman coefficient for categorical variables (intensity of pain and frequency of attacks) were used. A value of p < 0.05 was considered significant. Statistical analyses were performed with SPSS 16.0 for Mac software.
Results
Clinical characteristics of migraine patients and control subjects.
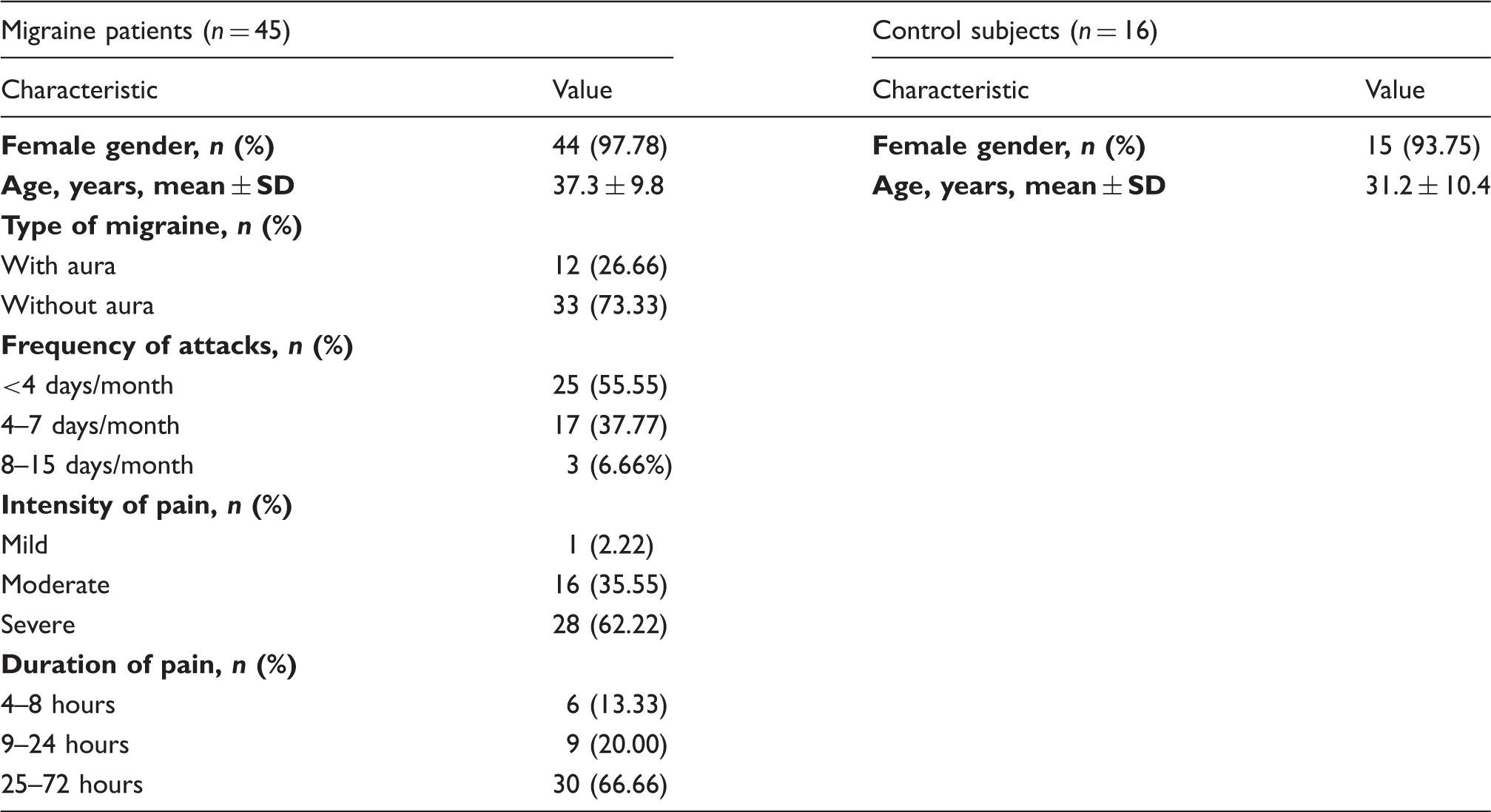
Migraine patients showed lower GOT activity levels (15.2 ± 2.9 vs. 18.7 ± 3.8 U/l; p < 0.0001) and higher levels of glutamate (153.7 ± 68.6 vs. 121.5 ± 59.2 μM; p < 0.05) compared with healthy subjects.
There were no significant differences between MWA and MA in relation to levels of GOT activity (15.0 ± 3.1 vs. 15.7 ± 2.8 U/l; p = 0.484) and glutamate levels (152.2 ± 64.1 vs. 157.7 ± 74.4 μM; p = 0.871).
Fifteen patients (nine MWA and six MA) were studied during a migraine attack. There were no significant differences between interictal and ictal periods in relation to levels of glutamate (145.1 ± 90.5 vs. 137.2 ± 96.2 μM; p = 0.947). Glutamate levels during interictal and ictal periods were higher than control subjects (all p < 0.05).
GOT activity was higher during ictal periods than interictal periods (21.2 ± 8.4 vs. 15.2 ± 3.5 U/l; p < 0.0001); however, GOT activity in migraine patients during headache attacks was not significantly different from GOT activity of control subjects (21.4 ± 8.4 vs. 18.7 ± 3.8 U/l, p = 0.324). Furthermore, triptan treatment (administered to 8 patients who suffered a headache attack) did not have an effect on GOT activity (p = 0.372) and glutamate levels during migraine attacks (p = 0.858).
On the other hand, no significant correlations were found between time of evolution and GOT activity (r = −0.099, p = 0.521) or glutamate levels (r = 0.118, p = 0.446). Likewise, no statistically significant association was found between intensity of pain and GOT activity and glutamate levels. However, if we compare only the groups of moderate and severe pain (considering that only one patient suffered from mild headaches), GOT activity (p = 0.058) and glutamate levels (p = 0.082) trend higher for the severe pain group. Furthermore, we found no relationship between frequency of migraines and GOT activity (p = 0.501) or glutamate levels (p = 0.891).
Finally, during attacks, we found a positive correlation between the time elapsed from attack onset and glutamate levels (r = 0.738; p < 0.0001) (Figure 1), but not for GOT levels (r = −0.075; p = 0.809). By contrast, a negative correlation has been found between GOT activity and glutamate levels (r = −0.493; p < 0.0001) in interictal periods (Figure 2); however, this negative correlation was lost during attacks (r = −0.026; p = 0.925).
Correlation between the time elapsed from attack onset and glutamate levels during ictal period. Correlation between GOT activity and glutamate levels during interictal period.

Discussion
In this study, we have found that migraine patients showed increased glutamate levels and lower GOT activity than control subjects. Furthermore, GOT activity was inversely associated with glutamate levels during interictal periods, while increased glutamate levels were associated with the duration of the pain during ictal periods, but no relationship was found for GOT activity. Based on the capacity of GOT to metabolize blood glutamate we propose that, during interictal periods, despite the low GOT activity and the high glutamate levels, there is still an adequate control of glutamate levels that appears reflected in a negative correlation between both parameters. However, such correlation disappears during migraine attacks because of the increase of glutamate. We hypothesize that although GOT activity increases during this period, it is not enough to reduce the glutamate levels that lead to a dysregulation of blood glutamate homeostasis and the subsequent migraine attack.
The negative correlation found between GOT activity and blood glutamate levels during interictal periods is also in agreement with our previous studies in stroke. Thus, in stroke, high brain and blood glutamate levels are tightly associated with neuronal damage. We have observed that ischemic stroke patients with good functional outcome showed lower glutamate levels and higher GOT activity in blood samples collected at admission (16,17), which seems to demonstrate the association between blood glutamate and GOT activity with brain glutamate levels.
The association between the dysregulation of glutamate and migraine attacks is widely described in the literature. Previous studies have observed that migraine patients present higher glutamate levels than controls in plasma, platelets, saliva or cerebrospinal fluid (CSF) (3,18–25), and this effect seems to be reflected in a reduction of urinary glutamate levels (26). It has been reported that in pathologic conditions associated with a large increase of glutamate in brain tissue (which has been shown to occur in pathologies such as ischemia, epilepsy, and presumably migraine), there is a diffusion of glutamate from the extracellular space to the blood following a gradient of concentration, which could explain the increase of systemic glutamate levels observed in these diseases.
Systemic increase in glutamate levels also seems to be associated with the occurrence of migraine attacks. In fact, it has been reported that diets rich in monosodium glutamate act as a potential trigger for migraine headaches (27). However, it is not clear how systemic changes of glutamate levels may affect the occurrence of migraine attacks by a dysregulation of the glutamate homeostasis in the brain. In this regard, glutamate transport at the blood-brain barrier (BBB) has been studied by both in vitro cell uptake assays and in vivo perfusion methods. The results demonstrate that the entrance of glutamate from the blood to the brain is rather limited in comparison to that observed for neutral amino acids (12,28). As a result, the BBB helps to protect the brain from changes in circulating plasma glutamate. However, stress situations, such as CSD in MA patients, are able to increase the permeability of the BBB through the activation of matrix metalloproteinases (MMPs), in particular MMP-9 (29–32), which could alter the permeability of the BBB allowing the diffusion of glutamate to the brain.
Therefore, due to the critical role of glutamate on migraine pathology, and the capacity of GOT to modulate glutamate homeostasis, we postulate that the treatment based on the administration of recombinant human GOT (hGOT) may be used as a potential prophylactic treatment to reduce blood and brain glutamate levels and consequently the duration of pain during migraine attacks.
Our study has several limitations. First, we did not determine the correlation of GOT activity with brain glutamate (CSF glutamate, for example), which would increase the significance of our results; however, glutamate CSF is not included in our clinical protocol for migraine patients, therefore such analysis was not possible to perform. Otherwise, experimental studies performed in our laboratory in ischemic model animals have demonstrated that modifications in blood glutamate levels were associated with brain glutamate changes that corroborate our conclusions in migraine. Another limitation of our study was that we did not determine GOT activity and glutamate levels at longer intervals after migraine attacks. In addition, the low number of patients from whom samples were obtained during a migraine attack should be taken into account, and this might weaken the strength of our conclusions. It is also possible that due to the small power, a type 2 error, a bias or the possibility of a chance finding may have occurred. Nevertheless, our statistical analysis showed with strong confidence that it is possible to associate GOT activity and glutamate levels during interictal periods. Therefore, the soundness of the present results might be relevant to evaluate the role of GOT as a new therapeutic tool for migraine patients.
In conclusion, this is, to the best of our knowledge, the first study that shows the involvement of the enzyme GOT on the dysregulation of glutamatergic homeostasis observed in migraine patients. Although further clinical trials are necessary to demonstrate our hypothesis, we suggest that the reduction of blood glutamate levels, based on the administration of recombinant hGOT, could be used as a potential therapeutic approach for migraine patients.
Clinical implications
Our aim was to study the association of GOT activity with serum glutamate levels and clinical parameters in patients with migraine. Migraine patients showed lower GOT activity than controls and higher levels of glutamate. A negative correlation was found between GOT activity and glutamate levels in interictal periods. During attacks, we found a positive correlation between the time elapsed from attack onset and glutamate levels but not for GOT activity.
Footnotes
Funding
This work was supported by the Instituto de Salud Carlos III: PI11/00909, CP12/03121 and Red de Enfermedades Vasculares Cerebrales INVICTUS (RD12/0014/0001); Xunta de Galicia (Consellería de Economía e Industria: 10PXIB918282PR; and Consellería de Educación: CN2011/010), and by the European Union program FEDER. Furthermore, T. Sobrino is recipient of a research contract from the Miguel Servet Program of the Instituto de Salud Carlos III. Sponsors did not participate in study design, collection, analysis or interpretation of the data, the writing of the report or in the decision to submit the paper for publication.
Conflict of interest
None declared.