
Abstract
Background
Headache associated with sexual activity is a well-known primary headache disorder. In contrast, some case reports in the literature suggest that sexual activity during a migraine or cluster headache attack might relieve the pain in at least some patients. We performed an observational study among patients of a tertiary headache clinic.
Methods
A questionnaire was sent to 800 unselected migraine patients and 200 unselected cluster headache patients. We asked for experience with sexual activity during a headache attack and its impact on headache intensity. The survey was strictly and completely anonymous.
Results
In total, 38% of the migraine patients and 48% of the patients with cluster headache responded. In migraine, 34% of the patients had experience with sexual activity during an attack; out of these patients, 60% reported an improvement of their migraine attack (70% of them reported moderate to complete relief) and 33% reported worsening. In cluster headache, 31% of the patients had experience with sexual activity during an attack; out of these patients, 37% reported an improvement of their cluster headache attack (91% of them reported moderate to complete relief) and 50% reported worsening. Some patients, in particular male migraine patients, even used sexual activity as a therapeutic tool.
Conclusions
The majority of patients with migraine or cluster headache do not have sexual activity during headache attacks. Our data suggest, however, that sexual activity can lead to partial or complete relief of headache in some migraine and a few cluster headache patients.
Introduction
Sexual activity can interact with headache in different ways. It can trigger headache, it can change the symptoms and semiology of preexisting headache, and it might be able to abort headache.
In particular, primary headache associated with sexual activity has been clearly described as an idiopathic headache disorder (1–4) and has been defined in the headache classification of the International Headache Society (IHS) (5). This headache occurs before or with orgasm and is differentiated into a preorgasm headache subtype and an orgasm headache subtype.
Furthermore, there are some reports that sexual activity can contribute to a relief of headache or even to a complete resolution (6–9). In a retrospective study, 57 out of 83 women reported that they had experience with sexual activity during migraine. About one-half (47.4%) of them reported a relief of the headache by this activity, 17.5% even reported complete relief (8). Similar single case reports exist for cluster headache (6,9).
Since only anecdotal data exist on the relief of headache by sexual activity, we performed a systematic study on the impact (i.e. improvement or worsening) of sexual activity on idiopathic headaches (migraine and cluster headache).
Methods
We contacted 800 migraine patients and 200 cluster headache patients who were registered at the headache outpatient clinic of the Department of Neurology, University of Münster and who had been personally examined in the two years before the study. The headache diagnosis was made according to the classification of the IHS (5). These patients received a standardized questionnaire together with the information that answering the questions is completely voluntary and anonymous. The questionnaires could not be linked to the charts of the patients or tracked in any other way. Only the main diagnosis (migraine or cluster headache) was noted on the questionnaire. The study was approved by the institutional study review board.
The questionnaire consisted of eight questions, with the first question about any experience with sexual activity during a headache attack. If this first question was answered with ‘yes,’ further questions should be answered. Patients were asked to send back the questionnaire in a free stamped envelope even if they had marked only a ‘no’ to the first question. The remaining questions asked for frequency of sexual activity during a headache attack, for improvement or worsening of headache during sexual activity and its reliability, for the necessity of having an orgasm to experience improvement, and for the therapeutic use of sexual activity during headache attacks. Sexual activity was defined as any sexual intercourse or masturbation with the aim of reaching an orgasm or an orgasm-like feeling.
In addition, we asked the patients for age, sex, age at onset of headache disorder, frequency of attacks, duration of attacks, presence of an aura, and presence of other headaches.
We used nonparametric testing for statistical analyses. For quantitative measures, we used the Mann-Whitney-U-test. For qualitative measures, we used the Χ2 test. The statistical significance level was set at p = 0.05.
Results
We received 402 questionnaires (migraine = 306; cluster headache = 96); all of them were suitable for analysis. One hundred and sixteen patients (migraine = 100; cluster headache = 16) could not be contacted by the registered postal address. The remaining 482 patients did not respond for unknown reasons. Since the survey was completely anonymous, we could not send the patients a reminder.
Demographic and clinical data of all patients presented as arithmetic mean with standard deviation or as percentage.

SA: sexual activity.
Demographic and clinical features of patients reporting having sexual activity during headache.
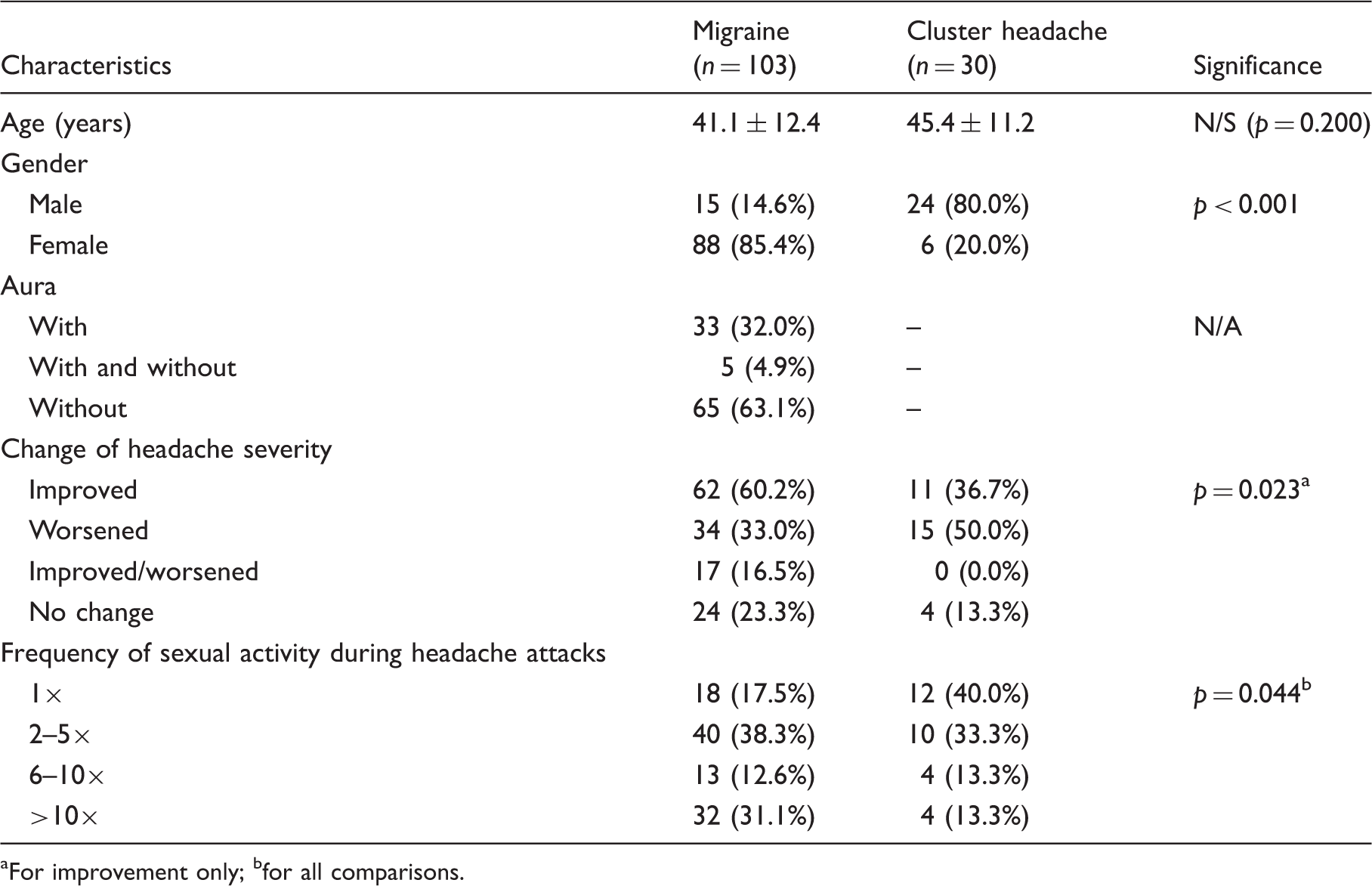
aFor improvement only; bfor all comparisons.
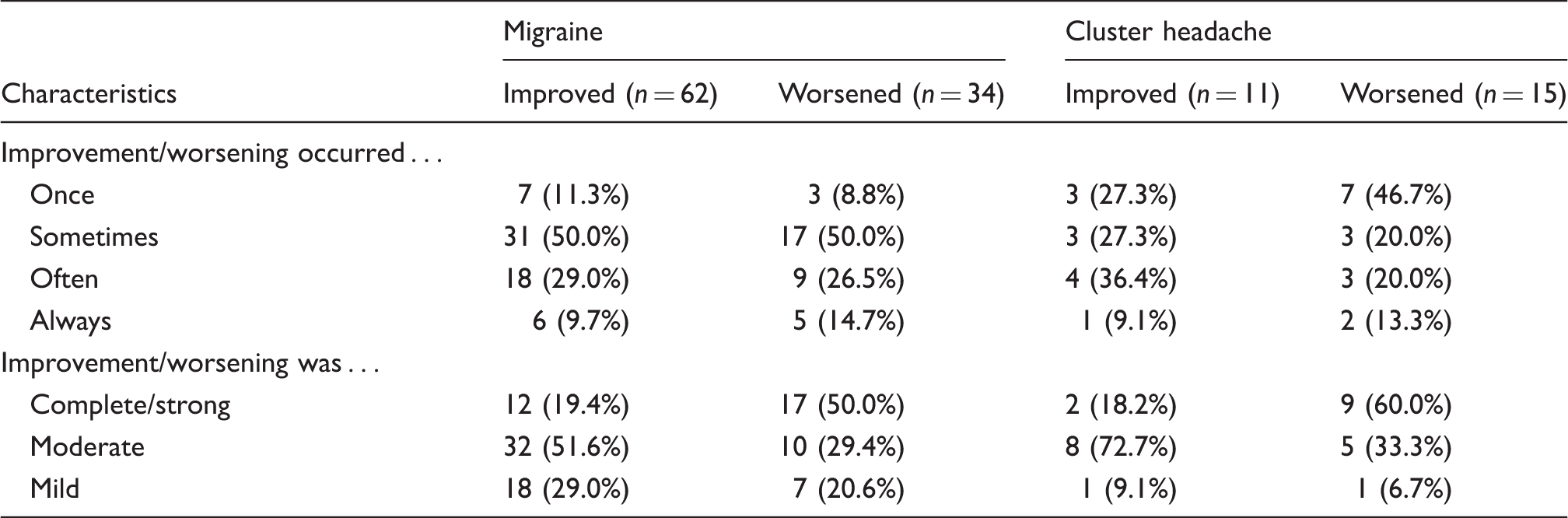
Degree and frequency of changes in migraine and cluster headache patients reporting improvement or worsening of pain during sexual activity.
Analyzing the circumstances of headache changes induced by sexual activity revealed that 43.0% of the migraine patients reported this change shortly after the time of orgasm or maximal excitement; 17.7% of the patients reported the change exactly with the time of orgasm, 20.3% at the beginning of sexual activity, and 20.3% within 30 minutes after orgasm or maximal excitement. This was similar in the cluster headache patients, with 73.1% having the change with or shortly after orgasm. The change of headache did not depend on the type of sexual activity (intercourse, masturbation, etc.), on the partner, on the time point during the headache attack, or on the position during the sexual activity.
Factors influencing improvement of headache in migraine patients reporting sexual activity during headache at least once.

In total, 36.4% of all male migraine patients experiencing improvement by sexual activity during the headache used this as a regular therapeutic tool, whereas only 13.7% of the female migraine patients did so. In cluster headache patients, 30.0% of those with an improvement of headache by sexual activity used this as a regular therapeutic tool (none of the female patients).
Discussion
This study was designed and performed in order to evaluate the impact of sexual activity during migraine or cluster headache attacks. Since this topic is a very intimate one, the study design ensured complete anonymity. Consequently, the number of responders was about as high as in other postal surveys on headache patients. However, we cannot exclude that more than the 133 patients in our sample ever had experience with sexual activity during headache but did not want to reveal it.
Comprehensibly, the headache attack and its associated symptoms (e.g. nausea in migraine) can discourage patients from being sexually active. However, the very high number of 103 migraine patients with experiences indicates that sexual activity in the presence of headache is not an unusual behavior. This is unexpected because migraine normally intensifies with physical activities such as walking or going upstairs, and patients often avoid any activity. It might reflect the patients’ observations that even severe migraine headache can be relieved by another stimulation of the central nervous system such as sexual orgasm (6).
The present survey shows that sexual activity during a migraine attack might relieve or even stop an attack in some cases. In particular, male patients (73.3%) feel migraine alleviation by sexual activity in contrast to 58.0% of the female patients. This result confirms reports in the literature reporting a similar outcome in a retrospective study (7); however, only female patients were included. About half of the participants (47.4%) in this study reported relief of headache.
Our data suggest that male migraine patients benefit more from sexual activity during headache than female migraine patients. The men showing a benefit had an average age of 43.9 ± 12.3 years and suffered from migraine without aura (54.5%) for 29.5 ± 15.8 years. On average, the headache attacks of these patients lasted up to 24 hours (45.5%) and appeared three times a month (54.5%). Also in cluster headache, male patients benefit more from sexual activity than female patients. Ten out of 11 cluster headache patients (90.9%) reporting relief were male. The average age of these patients was 43.5 ± 8.4 years, and they suffered from cluster headache for 15.7 ± 8.8 years. It remains unclear why men more frequently report headache relief by sexual activity. This cannot only be attributed to the fact that men have more experience with it. It could be due to sexual habits and the differences between men and women in reaching an orgasm. Consequently, more male migraine patients (36.4%) and cluster headache patients (30%) used sexual activity as an active therapeutic tool as compared to female migraine patients (13.7%). Besides the gender of the patients, we could not detect any prognostic factor that would determine which patient would benefit from sexual activity during headache attacks.
Furthermore, we also observed the typical differences between the two analyzed idiopathic headache disorders such as a converse rate of sex between the two headache disorders and a lower average age in the migraine group. However, the two headache disorders have in common the fact that about one-third of the patients had sexual activity during headache. More migraine patients seem to benefit from sexual activity than cluster headache patients. Further, more patients with cluster headache report worsening of the headache by sexual activity than migraine patients. This difference can be caused by several factors. First of all, the average pain intensity is lower in migraine as compared to cluster headache, making meaningful relief easier. For cluster headache, sexual stimulation might not be strong enough to influence the pain. Second, a migraine attack lasts longer than a cluster headache attack. In our study, 36.7% of the cluster patients and 14.6% of the migraine patients reported that the time of sexual activity during the headache attack influences the outcome. Thus, the probability of finding this best time point should be higher during migraine attacks.
In our study, the kind of sexual activity did not seem to have any influence on the particular reaction; 79.6% of the migraine patients and 60% of the cluster patients confirm this fact. Also, the primary headache associated with sexual activity appears to be independent of the specific sexual methods, e.g. while masturbating (2).
Furthermore, the degree of headache change differs between the patients (see Table 3). Some patients indicate a partial and others a complete relief of pain, similar as to that observed with drug treatment. Out of all migraine patients having had sexual activity during a headache attack, 60.2% felt an improvement of pain. This improvement could be divided in complete relief (19.4%), moderate relief (51.6%), and mild relief (29.0%). Thus, 42.7% of all migraine patients experienced at least 50% relief and can be classified as responders, a responder rate as high as in studies on acute medication.
The most obvious explanation of partial pain relief by sexual intercourse is just a distraction from pain. However, there are several other approaches in the literature explaining this phenomenon. Released endorphins, the postorgasmic relaxation, and extragenital reactions like blood pressure can cause pain relief, perhaps also in headache (10). For female patients, the stimulation of the posterior vagina, which is a physiologic reflex related to the birth process, could be a cause of pain relief in general (11). The alleviation of cluster headache intensity could be related to endorphin release, which occurs after sexual arousal and orgasm (12). Interestingly, magnetic resonance imaging (MRI) has shown a hypothalamic activation during cluster episodes (13,14). Similarly, it has been recognized that an orgasm is accompanied by intense hypothalamic activation (12). It has been postulated that an orgasm might influence the cluster headache by modulating the hypothalamic circulation (9).
Interestingly, it has been suggested that migraine patients show a higher level of sexual desire. As a possible reason, changes in the metabolism of the neurotransmitter serotonin have been proposed to be the underlying reason (15).
Our study has some limitations. The two most important are its retrospective nature and the subjective and uncontrolled answers of the patients. We chose a retrospective design since we wanted to have a database large enough for statistical analysis. Enrolling patients in a prospective study with these questions means interacting with their intimacy. Further, we made the survey completely anonymous. This meant we were not able to track the patients (e.g. we could not remind them to send back the questionnaire) and to compare their demographic or clinical answers with our records. Except for the baseline diagnosis (migraine or cluster headache), we had to rely on what the patients gave as demographic and clinical information. However, since our patients were all seen at least once in our headache clinic and educated with respect to their headache disorder, we believe that the demographic and clinical data can be relied on. There might be a bias with respect to the patients providing answers or not. In a conservative setting, it could be regarded as inappropriate to answer questions about sexual habits even if the answers are treated in a completely anonymous way.
A further limitation is that we enrolled only patients from a tertiary referral center. These patients are severely affected and do not represent the general migraine population. It cannot be differentiated whether patients with a milder form of migraine or cluster headache would benefit more or less by sexual activity during their headache attacks. Since we did not observe a correlation between headache severity/frequency and response to sexual activity, we assume that also milder forms of migraine or cluster headache would respond to sexual activity. Further, the definition of sexual activity remained somewhat arbitrary. We did not provide a strict definition as to what the term sexual activity comprises. Most of the patients referred to sexual intercourse or masturbation with orgasm. However, it could be that some patients thought of, for example, just touching or kissing with sexual intention.
In summary, the observed association between relief of headache disorders and sexual activity in some patients is not clear enough to derive the advice of sexual intercourse as a therapeutic mean for every patient. The individual patient has to test for herself or himself whether sexual activity is helpful in a specific headache attack. In order to make this decision, migraine and cluster headache patients should be informed on request about this association by their consulting physician. For future research, a prospective study including a headache diary and a control group with another type of activity during the headache attacks should be designed.
Clinical implications
Sexual activity can abort migraine and cluster headache attacks in some patients. Sexual activity is used by some patients as acute headache treatment.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.