
Abstract
Background
Migraine seems to be substantially related to hormonal changes. However, migraine, but also the use of combined oral contraceptives (COC), is associated with an increased risk for vascular events. Therefore progestagen-only contraception is an important alternative to combined preparations. Clinical observations and one pilot study demonstrate that the use of desogestrel 75 µg may have a positive impact on migraine.
Aim
The aim of this retrospective analysis of prospectively collected headache diaries was to study the effect of desogestrel 75 µg on headache frequency, intensity and use of acute medication in premenopausal women with migraine in a clinical setting.
Methods
Patients’ charts were included from women who wanted to use desogestrel 75 µg as a contraceptive and had kept headache diaries over six months (three months pretreatment and three months during treatment). Out of 58 women, 38 women had completed headache diaries for this period. Incomplete diaries (n = 12), side effects (n = 5) and loss to follow-up (n = 3) were the reasons for the exclusion of 20 women. The three months (total of 90 days) before and after initiation of the progestin were compared.
Results
Days with migraine (5.2 vs. 3.7), days with all kind of headache (8.3 vs. 6.5) and days with use of any headache medication (5.7 vs. 3.5) were significantly reduced at follow-up after three months. In addition there was a reduction in headache intensity (p < 0.0001). The reduction in number of days with use of triptans was not significant (p < 0.14).
Conclusion
In the 38/58 migraineurs with complete diaries there was a statistically significant decrease in migraine days, headache intensity and medication use. Tension-type headache days decreased but were not significant. Our preliminary data are promising, but should be interpreted cautiously because they were obtained in a small population of women visiting a specialty hormone and migraine clinic. Randomised controlled trials need to be conducted to substantiate our results.
Keywords
Introduction
Migraine with aura (MA), and to a lesser extent also migraine without aura (MO), may increase vascular risk, especially the risk for stroke in younger women (1–4). This risk may further increase when combined oral contraceptives (COCs) are used for the prevention of pregnancy (4–7). The cardiovascular risk of COCs, which contain ethinylestradiol and a synthetic progestin, has been mainly attributed to the oestrogen component which exerts a strong effect on the coagulation system. Progestagen-only pills (POP) and hormone-free intrauterine devices (IUD) have so far not been found to be associated with an increased risk for thromboembolic events (8).
Epidemiological and clinical data suggest that COCs eventually initiate or worsen migraine and headache in a subgroup of predisposed women (9–13). The incidence of migraine in women is highest during the reproductive years, and more than 50% of women report an association between their migraine and menstruation (14,15). The reproductive phase is also the life period during which most women need efficient contraception. Finding a well-tolerated form of contraception for headache patients, therefore, is an important issue to address.
Abrupt oestrogen withdrawal has for a long time been known to induce headaches in hormone-sensitive migraineurs, while steady levels of oestrogen on the other hand may play a protective role (16,17). During the normal menstrual cycle significant variations in the estradiol plasma levels occur after ovulation and 24–48 hours before onset of menstruation. During contraception with COCs, the hormone-withdrawal in the pill-free phase can trigger migraine attacks.
As the progestagen-only contraceptive pill, desogestrel 75 µg (Cerazette®; MSD Merck Sharp & Dohme AG, Luzern, Switzerland) combines continuous use with efficient inhibition of ovulation and maintenance of stable oestrogen levels, it seems to be qualified for use in migraineurs (16–18).
The motivation for the present study came from the frequent observation in daily clinical practice that migraine in many women improved with the use of desogestrel 75 µg. We therefore retrospectively analysed the headache diaries of women with migraine, before and after the initiated contraception with this POP.
Patients and methods
The study was performed at the division for family planning, subunit of the clinic for Reproductive Endocrinology, University Hospital Zürich, where one of the authors (GM) runs an outpatient clinic for migraine and hormones.
Patients’ records from July 2009 through June 2011 have been searched for women with MA and MO who were recommended to start POP desogestrel 75 µg for contraception. Migraine had been diagnosed according to the International Headache Society (HIS) criteria by the referring neurologists from the headache and pain unit, department of neurology, University Hospital Zürich or from the Headache Centre Hirslanden in Zürich (18). Headaches were all tension-type headaches according to the IHS classification.
Patients’ charts were identified from daily printouts of the patient lists in the clinic for migraine and hormones. Charts were included only when at least three monthly headache episodes were reported in the pretreatment period and complete headache diaries over the observation period of six months (three months before and three months after initiating hormonal treatment) were available. The patients in our clinical routine kept headache diaries including information on the number of migraine and headache days, the use of triptans and other pain medication, the use of hormones and monthly bleeding. Headache severity was rated in the diaries according to a four-point scale (0 = no pain, 3 = severe pain). For ethical reasons all diaries were anonymised before data evaluation. The evaluation of anonymised data in our setting was approved by the regional ethical committee.
Statistical analyses were made using IBM SPSS Statistics, version 19 (IBM, New York, NY, USA). Baseline data are presented as mean (SD). From the first day in the headache diaries onward we included 90 days for the pretreatment analysis. Analysis of the treatment period includes 90 days from the first day of desogestrel use onwards. Mean pain intensity was calculated as the sum of headache intensities for the pretreatment and treatment periods according to the above-mentioned four-point scale. For each period this sum was divided by three to obtain the mean monthly pain intensity. Number of monthly migraine days, headache days, headache intensity and use of pain medication were compared with within-patient paired nonparametric Wilcoxon-test.
Results
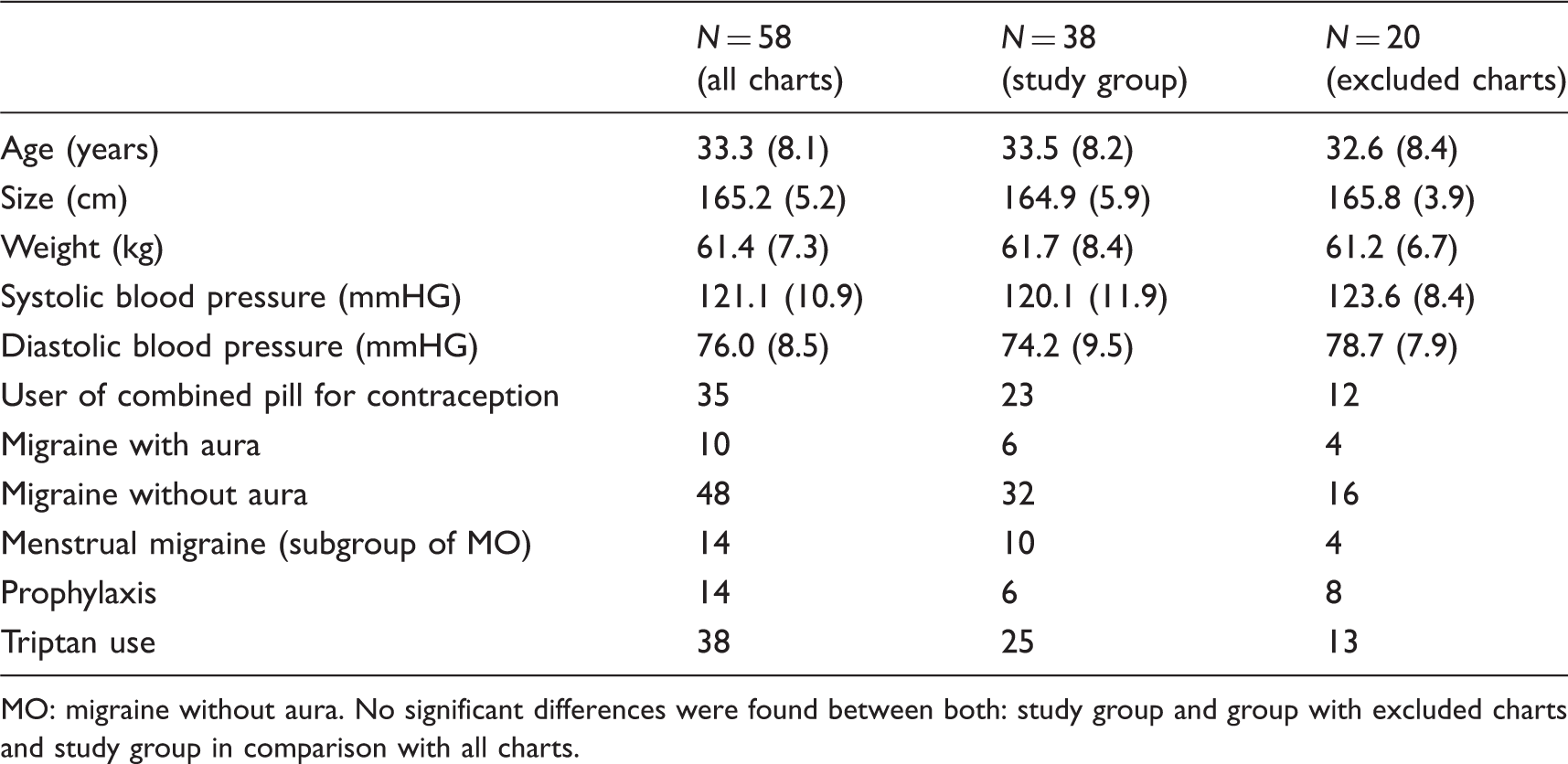
From a total of 58 patients with migraine and use of POP, complete diaries from 38 women were eligible for analysis (Figure 1). Twenty patients had to be excluded because of: loss of follow-up (n = 3), incomplete diaries (n = 12) and discontinuation of desogestrel earlier than three months because of side effects (prolonged bleeding n = 3, increase of headache n = 2). Baseline data of included and excluded patients, as well as their headache characteristics, are presented in Table 1. With regard to those data no differences were found between the two groups. MO was more common (n = 32) in comparison with MA (n = 6) within the study group. Number of monthly days with migraine, days with any kind of headache, and days with use of any pain medication were significantly reduced during contraception with desogestrel 75 µg, whereas the reduction in the number of nonmigrainous headache was not statistically significant (Table 2). The mean pain intensity decreased and the monthly number of days with severe pain declined from 4.9 (±4.0) to 2.1 (±2.7) during the three-month treatment period (p < 0.0001) (Table 2). Days with use of a triptan decreased nonsignificantly (pretreatment 10.4 (±10.4) vs. treatment 8.5 (±9.0) (p < 0.14)).
Flow diagram of patient charts. Demographic parameters and migraine characteristics for study group and charts not meeting the inclusion criteria. MO: migraine without aura. No significant differences were found between both: study group and group with excluded charts and study group in comparison with all charts. Tension-type headache days, migraine days, pain intensity,
a
frequency of triptan and any other pain medication in women with need for contraception before and during use of desogestrel 75 µg. Headache intensity was calculated as the 90-day sum of headache severities rated from a four-point scale (0 = no headache, 1 = mild headache, 2 = moderate headache and 3 = severe headache). For the monthly headache severity, we divided this sum by three.

Figures 2 and 3 provide detailed information on the absolute changes in migraine days, tension-type headache days, sum of all headache days and pain intensity for the 90-day interval before and during treatment. Within the study group of 38 women, the number of migraine days decreased in 33 patients, the total number of headache days in 28 patients and pain intensity in 35 out of 38 patients. Five women experienced a small increase in the number of migraine days. Three of them reported nevertheless an improvement in pain intensity and all headache days, whereas in another two in addition to migraine days, days with tension-type headaches and pain score worsened as well (patients number 5 and 26; Figures 2 and 3). An increase in number of days with tension-type headaches was observed in 13 women (Figure 2). Of concern might be the subgroup of five, who experienced more than five additional headache episodes within 90 days (Figure 2). However, a more detailed look at these patients reveals a considerable improvement in the number of migraine days and in pain intensity (range two to 20 days and six to 26 days), implying an overall positive effect of desogestrel for this group (Figures 2 and 3).
Individual patient data for absolute change in migraine and headache days after 90 days’ treatment with desogestrel 75 µg. Absolute difference in days of all types of headache compared in relation to change in pain intensity.a Baseline period compared to treatment period.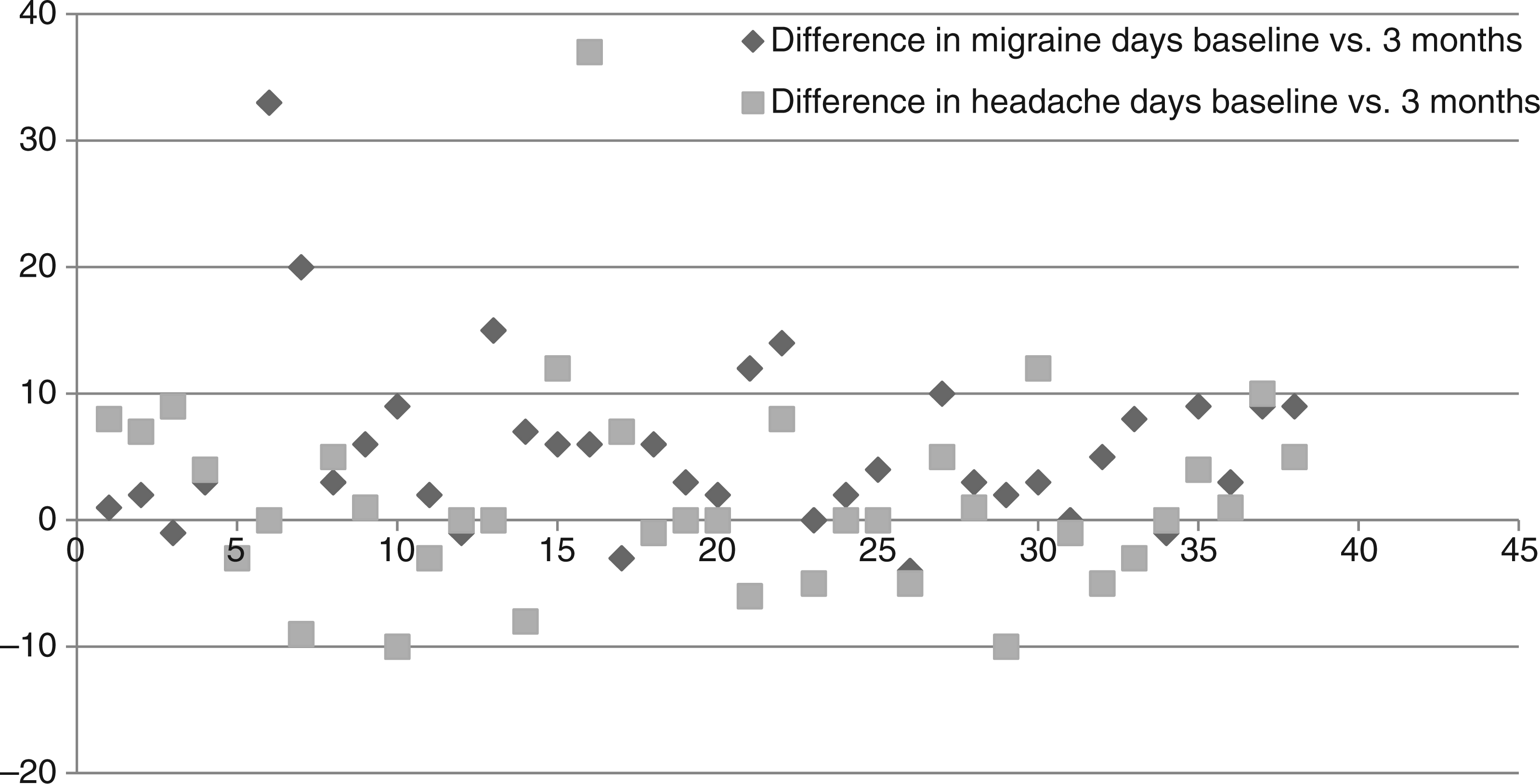

When women with MA were excluded, the subanalysis of only females with MO showed very similar results: reduction in migraine days (p < 0.003); reduction in all headache days (p < 0.02) reduction in days with pain medication (p < 0.03); reduction in pain intensity (0.0001) and reduction in the number of days with severe pain (p < 0.0001).
Discussion
The higher prevalence of headache in women compared to men has been attributed to the effect of sex hormones. High oestrogen levels and oestrogen withdrawal are thought to play a pivotal role in female migraine (19). However, sex differences extend beyond the effect of the menstrual cycle (15). In the present study we found that contraception with the oestrogen-free pill desogestrel 75 µg resulted in a significant reduction in migraine days and total days of headache in women with migraine. To our knowledge our subanalysis of MO patients (n + 32) demonstrates for the first time a positive effect of desogestrel 75 µg on this type of headache, too. We further observed a significant drop in days with use of acute pain medication and also in headache severity over the period of three months.
A more specific view on the individual patient data demonstrated a broad range of feasible reactions on the desogestrel pill (Figures 2 and 3). Our principally very positive results eventually could be compromised by the observation that five women experienced an increase in migraine days and another five an increase in more than five headache days over the period of three months. However, because the more detailed analyses of these individual cases in the results section show an improvement in other parameters like pain intensity or migraine frequency (eight of 10 women), we assess our overall results as promising. Interestingly, the subgroup of participants with more headaches includes predominantly women with a high frequency of migraine attacks. The reduction in migraine appears sometimes to induce an increase in less pain-intensive headache days.
Our overall observation of a significant decrease in pain medication is in line with the improvement in pain score. Decline in triptan use was not significant, probably because of the low number of triptan users in our study.
If replicated in more rigorous studies, we theorise that there are several explanations for a beneficial effect of desogestrel on migraine. From the pathophysiologic perspective of the hormonal side of headaches, it has been demonstrated that during the normal cycle the activity of neurotransmitter systems involved in the pathophysiology of migraine vary. Concomitant with the decline of oestrogen levels in the premenstrual phase, inhibitory systems like the serotonergic and gabaergic systems are at their nadir. This might explain why these days of the cycle are especially vulnerable for the occurrence of migraine attacks (20). To avoid estradiol withdrawal and high estradiol levels, an estradiol-free pill like desogestrel 75 µg could be regarded as suitable because it is used without hormone-free phases, inhibits ovulation and prevents hormone withdrawal. Oestrogen levels released from the ovary during its use are steady and low (16). Another approach to explain potential positive effects of desogestrel 75 µg focusses on direct effects of the progestin. Although the dosage of 75 µg desogestrel is rather low, the biological effects are significant because the complex steroid structure of this ethyl-gonane delays liver metabolism and prolongs the half-life of the substance (21). Progestins are known to antagonise oestrogen actions in reproductive tissues and the brain by lowering oestrogen receptor expression (22–25).
Female reproductive hormones have been associated with neuronal excitability with oestrogen acting as an inducer and progesterone as a depressor (26). Thus the daily administration of a progestin might, independent of its effect on estradiol levels, contribute to a positive effect on migraine.
Finocchi and Ferrari mainly attributed the hormonal effects to MA via cortical spreading depression as suggested by underlying pathophysiology (26). If our data are confirmed in further trials, this hypothesis has to be challenged, as we observed also in MO patients a reduction in migraine days.
In patients with MA, Nappi et al. demonstrated a significant improvement of MA symptoms with use of desogestrel 75 µg (27). The beneficial effects in this study were obtained over six months; however, no substantial further improvements after three months have been observed. Our study for the first time reports data from patients mainly suffering from all types of migraine.
The use of POP can be associated with unscheduled bleeding, which can be uncomfortable and a reason for withdrawal of this form of contraception. This side effect demands good counselling and in some cases treatment. Prolonged withdrawal bleeding mostly stops with longer duration of use. In analogy to Nappi et al. we observed very rarely an aggravation of headache symptoms in the early phase of contraception with desogestrel (27). This supports the view that this POP might not only improve migraines, but can also act as a trigger for more headaches in a few hormone-sensitive migraineurs. Altogether we saw a broad variety of reactions on desogestrel 75 µg. Besides a few cases with worsening, the improvement of migraine frequency ranged from 20% to 100%. Some women reported no change in headache, but still were using a more healthy form of contraception than COCs (3,28,29). The genetic variability of oestrogen receptors with some polymorphisms being a significant risk factor for migraine eventually could be involved in this different type of reaction on a progestin (30).
Some authors have suggested that the continuous use of COCs or the shortening of the hormone-free interval exerts a positive impact on hormonal types of migraine (31–33). This treatment approach does make sense from the perspective of preventing hormone withdrawal. However, the increased vascular risk, which rises multiplicatively if migraineurs have additional cardiovascular risk factors like age, obesity or smoking, should definitely be considered (34,35). The impact of extended cycle regimens on long-term safety especially with regard to breast cancer and fertility after discontinuation still has to be assessed (36). Therefore the use of extended COC regimens is an off-label use in most countries.
The findings of this study must be interpreted in the context of its strengths and limitations. Even if our results are based on precisely kept headache diaries, a prospective placebo-controlled study design using electronic diaries would have been of advantage. Twelve women could not be included because of incomplete diaries. Results might not be representative for all women with migraine because of the small study size including women from a specialised clinic. Furthermore it remains to be demonstrated in the future whether the beneficial effects of desogestrel on migraine are maintained during longer treatment. At the moment the data from Nappi et al. support the view that the highest improvement occurs within the initial three months of use and that the positive effects persist at least for six months (27).
In conclusion our preliminary data indicate that contraception with desogestrel 75 µg not only provides efficient contraception but also exerts a positive impact on migraine frequency, intensity and use of pain medication in the majority of patients in our clinical setting. We strongly propose further investigation of this issue in prospective randomised trials.
Clinical implications
Combined oral contraceptives (COC) usually are considered as absolutely or relatively contraindicated in migraineurs because of the increased risk for cardiovascular events. Furthermore these preparations might initiate or worsen headache and migraine in a few hormone-sensitive women. Our data indicate that the progestin-only pill desogestrel 75 µg in addition to providing efficient contraception tends to improve migraine frequency and intensity in female migraineurs. Because of the limitations of our study with regard to sample size and design as an observational investigation, these results are at too early a stage to draw definite conclusions. Nevertheless we strongly propose further investigation of this issue in prospective randomised trials.
Footnotes
Acknowledgement
We thank Burkhardt Seifert for his help and comments on statistics.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for -profit sectors.
Conflicts of interest
Gabriele S. Merki-Feld had a financial relationship (lecturer, member of advisory boards and/or consultant) with Bayer-Schering Pharma and MSD AG.
B.I., R.L., P.S. and A.G. declare no conflicts of interest.