
Abstract
Background
The pathophysiology of idiopathic sudden sensorineural hearing loss (SSNHL) is poorly understood. Few case reports have proposed a possible link between migraine and SSNHL.
Objectives
This study aimed to explore the risk of idiopathic SSNHL in patients with migraine in a nationwide, population-based cohort study.
Methods
We identified patients with migraine from the Taiwan National Health Insurance Research Database (NHIRD) between 2000 and 2009. Each migraine patient was matched with four randomly selected subjects without migraine for age, sex, and comorbidities. Both cohorts were followed up until the end of 2009. We compared the incidence rates of SSNHL in the two cohorts and identified the risk factors.
Results
A total of 10,280 migraine patients and 41,120 matched controls were enrolled with a median follow-up of five years. The migraine cohort had a greater risk of developing SSNHL than the matched cohort (81.6 vs. 45.7 per 100,000 person-years, incidence rate ratio (IRR) = 1.8; 95% confidence interval (CI) 1.22–2.61, p = 0.002). The Cox proportional hazards analysis revealed that among migraine subjects, comorbidity with hypertension was associated with a trend of developing SSNHL (hazard ratio (HR) = 1.92, 95% CI 0.97–3.79, p = 0.06).
Conclusions
This population-based study demonstrates that migraine is associated with an increased risk of idiopathic SSNHL, which, however, is a rare condition.
Introduction
Sudden sensorineural hearing loss (SSNHL) is a frightening symptom characterized by rapid deterioration of hearing within a very short period of time. It is one of the most common emergencies in the daily practice of otorhinolaryngologists. The incidence is estimated at 20 per 100,000 person-years, but may vary from five to 160 per 100,000 person-years (1–6). SSNHL is usually defined as an unexplained sensorineural hearing loss greater than 30 decibels (dB) in three consecutive audiometric frequencies occurring over a 72-hour period (7). Any age group may be affected, but the peak incidence occurs in the fifth or sixth decade of life, and there is an equal gender distribution (4). The hearing impairment is mostly unilateral, with bilateral involvement in less than 5% of cases (8). Approximately half of the patients completely or partially recover; however, those who present with severe or profound hearing loss have a particularly poor prognosis regardless of the type of treatment (9). Permanent hearing loss due to SSNHL, though unilateral and having a variable degree, is usually an incapacitating event that greatly impacts the quality of life and the ability to interact socially and causes severe morbidity (10).
The pathophysiology of SSNHL is poorly understood. Up to 85% of the cases are idiopathic (4). Previous studies have suggested numerous possible pathophysiological mechanisms for SSNHL, including viral infections, ischemic insults, and autoimmune diseases. Vascular etiology has gradually gained popularity because of the abrupt onset of the clinical presentation and the correlation between SSNHL and certain vascular events (11–13). One population-based study demonstrated that patients hospitalized because of SSNHL were 1.6 times more likely to develop stroke in the following five years (11).
Migraine, especially migraine with aura, has been shown to be a risk factor for cardiovascular events (14,15). Recently, a few case reports have suggested a possible link between migraine and SSNHL (12,16). Therefore, to explore the risk of idiopathic SSNHL in migraine patients, we conducted a nationwide population-based cohort study and analyzed data from a large nationwide medical database, the National Health Insurance Research Database (NHIRD) in Taiwan.
Materials and methods
Data sources
Taiwan launched the National Health Insurance (NHI) program in 1995 to finance health care for all citizens, with a coverage rate of up to 98% (17). The NHI is a mandatory universal health insurance program offering comprehensive medical care. It includes coverage for outpatient, inpatient, emergency, dental, traditional Chinese medicine services, and prescription drugs. The multiple NHI databases (i.e. NHI enrollment files, claims data, and registry of drug prescriptions) provide comprehensive utilization and enrollment information for all patients under the NHI program. This study used NHI databases that are managed and publicly released by the National Health Research Institute of Taiwan. The confidentiality of the data abides by the regulations of the Bureau of the NHI and the National Health Research Institute. All information that would potentially expose a specific individual to be identified has been encrypted. Since the NHI dataset consists of de-identified secondary data for research purposes, this study was exempt from full review by the institutional review board.
Study population
We conducted a retrospective cohort study from January 1, 2000, to December 31, 2009. We enrolled patients who were diagnosed with migraine by a neurologist according to the migraine diagnosis codes (346.0x, 346.1x, and 346.9x) in the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). Patients who were diagnosed with migraine at an age <20 or ≥65 years old were excluded. Patients with antecedent cerebrovascular disease or antecedent SSNHL were excluded. In addition, those who were diagnosed with acoustic neuroma or Meniere's disease at any time within the study period were also excluded from the analysis. The information on comorbidities and migraine medications, such as non-steroidal anti-inflammatory drugs (NSAIDs), triptans, and ergot alkaloids, were collected for analysis as well. Drug usage was defined as a prescription for 28 days or more within one year before the endpoint of the study. Both the migraine cohort (n = 10,280) and the matched cohort (n = 41,120) were followed up until the development of SSNHL, transfer out of the NHI program, death, or the end of the year 2009.
Control cohort
Subjects without migraine were used as the matched (non-exposure) cohort. The subjects in the non-exposure cohort were randomly selected from the same database. Each migraine patient was matched with four non-exposure subjects by age, sex, and comorbidities within the same observational period. These comorbidities, which included diabetes, hypertension, dyslipidemia, and atrial fibrillation, were chosen because they are known to be associated with SSNHL based on previous publications (18). The same exclusion criteria described above were also applied to the control subjects.
SSNHL
The outcome variable of this study was the new occurrence of SSNHL, as defined by a compatible ICD-9-CM code 388.2 that was coded by an otorhinolaryngologist.
Statistical analysis
The incidence rates (per 100,000 person-years) with 95% confidence intervals (CIs) and incidence rate ratios (IRRs) of SSNHL in both groups were analyzed. The Kaplan-Meier method and the Cox proportional hazards models were conducted. We used univariate analysis to explore the associations between each possible confounding factor and SSNHL. All statistically significant covariates (p < 0.1) in univariate analyses were then included in a Cox multivariable model. Extraction and computation of data were performed with the Perl programming language (version 5.12.2). Microsoft SQL Server 2005 (Microsoft Corp., Redmond, WA, USA) was used for data linkage, processing, and sampling. All statistical analyses were carried out with IBM SPSS statistical software version 19.0 for Windows (IBM Corp., New York, NY, USA). Statistical significance was defined as a p value of less than 0.05.
Results
Clinical characteristics of the study population
Baseline characteristics of patients with migraine and matched cohort.

Comparisons of the incidence rates of SSNHL between migraine patients and the matched cohort
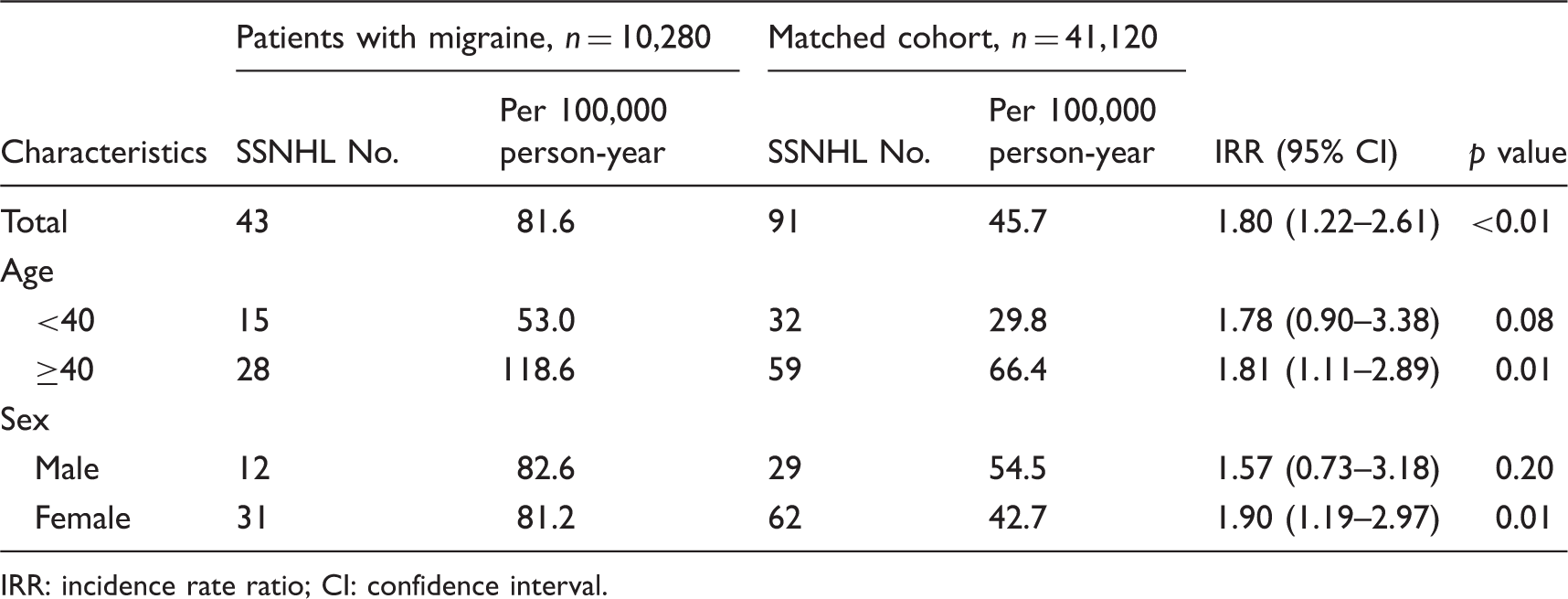
Among the 51,400 subjects, 134 (0.3%) developed SSNHL during the follow-up. Within each cohort, 43 (0.4%) subjects from the migraine cohort and 91 (0.2%) subjects from the matched cohort developed SSNHL (Fisher’s exact test, p = 0.001) (Table 2). The average onset ages of SSNHL in the migraine (45.1 years old) and the matched cohorts (45.72 years old) did not differ (p = 0.76). Kaplan-Meier estimates showed that the cumulative incidence of SSNHL in the migraine cohort was significantly higher than that in the matched cohort (log rank, p = 0.002; Figure 1). The incidence rate of SSNHL was 81.6 (95% CI 81.3–81.9) per 100,000 person-years of follow-up in the migraine cohort and 45.7 (95% CI 45.5–45.9) in the matched cohort. The migraine cohort had a greater risk of developing SSNHL than the matched cohort (IRR = 1.8; 95% CI 1.22–2.61, p < 0.01).
Cumulative incidence of sudden sensorineural hearing loss (SSNHL) in migraine and matched cohorts. The risk of sudden sensorineural hearing loss (SSNHL) for patients with migraine and matched cohort. IRR: incidence rate ratio; CI: confidence interval.
Subgroup analysis
Patients aged ≥40 years had a higher incidence than those under 40 (118.6 vs. 53.0 per 100,000 person-years) in migraine subjects. However, the IRR values were almost the same for these two subgroups, and statistical significance was reached only in those aged ≥40 years (Fisher’s exact test, p = 0.01; Table 2).
The incidence rates of SSNHL in female and male migraine subgroups (81.2 vs. 82.6 per 100,000 person-years) were similar. The female migraine subgroup had a higher IRR than the male subgroup, and only the former reached statistical significance (Fisher’s exact test, p = 0.01; Table 2).
Subjects diagnosed as having migraine without aura had a significantly higher IRR in comparison to age-, sex-, and comorbidity-matched controls (IRR 1.77, 95% CI 1.18–2.60, p = 0.004). Only three of the 959 patients who had migraine with aura developed SSNHL (IRR 2.28, 95% CI 0.35–11.74, p = 0.29).
Risk factors for SSNHL in migraine patients
Risk factors for sudden sensorineural hearing loss (SSNHL) in patients with migraine.

All factors with p < 0.1 in univariate analyses were selected for Cox multivariable analysis.
HR: hazard ratio; CI: confidence interval; NSAIDs: non-steroidal anti-inflammatory drugs.
Discussion
Our nationwide, population-based, cohort study demonstrated that migraine was associated with an increased risk of developing SSNHL that was 1.8 times higher than that of the matched controls. The incidence rate was 81.6 per 100,000 person-years in the migraine cohort in contrast to 45.7 in the matched control cohort. Furthermore, migraineurs comorbid with hypertension had a trend of developing SSNHL (HR = 1.92) while those without did not. To our knowledge, this research is the first to demonstrate that migraine is associated with an increased risk of idiopathic SSNHL.
The major strength of this study was its population-based design, which examined a representative cohort of 1,000,000 citizens covered under the NHI in Taiwan. The large sample size and long observation period offered enough power to delineate the differences between the two study groups. To achieve a high validity, the enrolled migraine patients were diagnosed only by neurologists, and the outcome variable, new-onset SSNHL, had to be coded by an otorhinolaryngologist. Additionally, patients with Meniere’s disease or acoustic neuroma at any time within the study period were excluded since SSNHL might be the initial manifestation in these diseases. The strict inclusion and exclusion criteria minimized possible coding deviations in this claims dataset.
The incidence rate of SSNHL in our control cohort was at the higher level among prior epidemiological studies (1,2,4–6). This difference could be explained by the easy accessibility and comprehensive coverage of the NHI in Taiwan. In fact, the average number of clinic visits was as high as 15.6 visits per person per year in 2010 (19). The equal occurrence of SSNHL in males and females demonstrated in our analysis was comparable with previous studies (3,4). In the subgroup analysis, only female migraine patients showed a significant rate of developing SSNHL. This observation is likely because only one quarter of the study participants were male. The female predominant pattern was also consistent with migraine epidemiology (20). Those who were diagnosed as having migraine without aura had a significantly higher IRR to develop SSNHL. The number of cases of new-onset SSNHL in the migraine with aura cohort was too small (n = 3) to reach any statistical inference. Moreover, risk factors such as hypertension, diabetes mellitus and dyslipidemia were not significantly associated with the development of SSNHL, but they indeed yielded similar trends (18).
The exact mechanism linking migraine and SSNHL is unknown. In 1987, Lipkin et al. first described a 62-year-old woman who had recurrent hearing loss in conjunction with migraine attacks (16). Viirre and Baloh later presented 13 cases of individuals with unexplained SSNHL who met the diagnostic criteria for migraine (13), and they suspected that the disturbance of cochlear microvasculature might be the cause. In 2003, Lee et al. observed two otherwise healthy, young patients who had migraine attacks with acute hearing loss, and they speculated that the auditory symptom was part of the prodrome in migrainous infarction (21). The only histopathology evidence connecting migraine and SSNHL was provided by Lee et al. in 2000 (12). The authors presented a man with long-standing migraine who developed SSNHL at age 50. Postmortem examination of the cochlea showed prominent fibrosis in the stria vascularis and spiral ligament, which are the characteristics of an ischemic insult. Thus, the authors postulated that the deafness might have resulted from migraine-associated vasospasm. Nevertheless, a number of histopathological studies regarding the etiologies of SSNHL provided conflicting findings (22–24), and it is of note that the diagnosis of migraine was never documented in these reports.
It is worth mentioning that in our research, the migraine cohort enrolled from the NHIRD was made up of active migraineurs who sought medical help during the study period. After controlling for the major cardiovascular comorbidities and excluding antecedent cerebrovascular disease, the difference in the vascular components in both cohorts was minimized as much as possible. Under this circumstance, however, migraine was still associated with an increased risk for SSNHL. Thus it is inferred that there are some unknown mechanisms other than vascular components connecting migraine and SSNHL. It has once been proposed that pathologic activation of cellular stress pathways involving nuclear factor-kappa B within the cochlea could possibly contribute to SSNHL (24). Recent evidence also indicated that SSNHL was related to certain inflammatory mediator genes (25). The hypothesis that migraine-associated inflammation (26) or neurovascular dysfunction (27) in response to certain triggers gives rise to the occurrence of idiopathic SSNHL should be probed in future research. Further studies would also be needed to investigate the prognosis of SSNHL in migraine patients as well as to clarify the underlying causes for the link between migraine and SSNHL.
Our study has a number of implications. Migraine is comorbid with several cardiovascular disorders, and most of these disorders are also associated with SSNHL (18,28). Therefore, controlling these risk factors in migraine patients might reduce the occurrence of SSNHL. In addition, physicians must be more alert to auditory complaints of migraine patients, especially in those with vascular risk factors, since they are more likely to develop SSNHL. Early recognition and prompt management of SSNHL can improve hearing recovery (7). Finally, migraine history should be routinely inquired about in patients with SSNHL. Examining migraine history can be used to clarify the etiology and to delineate whether SSNHL development in migraineurs could have a different prognosis.
The following are limitations of this study. First, deviations in coding of the claims data were inevitable. We used a matched control cohort to offset the possible coding errors and to minimize bias. Additionally, the NHI routinely and randomly samples medical charts from every contracted medical institution. The accuracy of medical coding was audited by an independent group of physicians. Second, it is difficult to explore the prognosis of SSNHL, since the NHIRD is an administrative database that lacks detailed clinical data on the severity and outcome of hearing loss. Third, the small sample size of certain subgroups might have contributed to failure in showing migraine as a significant risk factor in the subgroup analyses.
In conclusion, our study demonstrated that patients with migraine had a 1.8-fold greater risk of developing idiopathic SSNHL compared to the age-, sex-, and comorbidity-matched control cohort. Though idiopathic SSNHL is a rare condition, auditory symptoms in migraine patients should still alert physicians to the possibility of developing SSNHL, especially in those comorbid with vascular risk factors.
Clinical implications
The pathophysiology of idiopathic sudden sensorineural hearing loss (SSNHL), a common emergency in otolaryngology, is poorly understood. This research is the first population-based study to demonstrate that migraine is associated with an increased risk for idiopathic SSNHL. Patients with migraine had a 1.8-fold greater risk of developing idiopathic SSNHL during a median follow-up of five years. Migraine is comorbid with several cardiovascular disorders, and most of them are also associated with SSNHL. Therefore, controlling some risk factors, i.e., diabetes and hypertension, in migraine patients might reduce the occurrence of SSNHL. Physicians are advised to be more alert to auditory complaints of migraine patients, especially in those with vascular risk factors, since they are more likely to develop SSNHL, which, however, is a rare condition.
Footnotes
Acknowledgement
Miss Chiu-Mei Yeh made a great contribution to the revision of this manuscript on the calculation and interpretation of statistical analyses.
Funding
This study was supported in part by grants from the Taiwan National Science Council (100-2314-B-010-019-MY2, 100-2314-B-010-018-MY3), Taipei Veterans General Hospital (VGHUST101-G7-1-1, V101C-106, V101E7-003), NSC support for the Center for Dynamical Biomarkers and Translational Medicine, National Central University, Taiwan (NSC 100-2911-I-008-001), Brain Research Center, National Yang-Ming University and a grant from Ministry of Education, Aim for the Top University Plan.
Conflict of interest
None declared.