
Abstract
Objectives:
To investigate the prevalence, characteristics and clinical correlates of transient visual disturbances (TVDs) in adolescents with headaches.
Methods:
We surveyed headache-related TVDs in the past three months in two middle schools. All the ninth-grade students filled-in the questionnaires including demographics, a validated headache questionnaire, and visual phenomenon questions embedding the Visual Aura Rating Scale (VARS). TVDs were defined as transient visual phenomena corresponding to a headache attack, but not visual aura, i.e. VARS <four.
Results:
Six hundred and sixty-three adolescents (341 boys and 322 girls; mean age 15.1 ± 0.3 years old) participated in this study. In subjects reporting at least one headache during the past three months (N = 371), 33.4% reported TVDs, which accounted for 18.7% in total participants. TVDs were described mainly as flickering lights or scotoma, movable, monochromatic, occurring over bilateral visual fields, developing and lasting <30 seconds, and experienced during the headache phase. Subjects with migraines reported a higher frequency of TVDs than those with non-migraine headaches (67.1% vs. 31.2%, p < 0.001). TVDs were independently associated with photophobia (OR = 12.6, p < 0.001) and pulsatile headache (OR = 2.1, p = 0.012).
Conclusions:
The major features of TVDs were distinguishable from visual aura. TVDs were common in adolescents with headaches, especially in migraineurs.
Introduction
Visual aura is a reversible visual symptom that usually precedes or sometimes accompanies a headache (1). It develops over 5 to 20 minutes, lasts less than 60 minutes, is located in the homonymous visual field, and is characterized by positive (e.g. flickering lights, spots or lines) or negative features (i.e. loss of vision). Cortical spreading depression, starting from the occipital cortex, likely generates visual auras in the human brain (2). The headache associated with visual auras commonly carries migrainous features, but it can also present without them, and in some occasions, the headache could be completely absent (1).
Transient visual disturbances (TVDs) are also visual phenomena associated with headaches; however, there is no universal definition for TVDs, and the exact origin remains unclear. There are only a few research groups studying epidemiology and symptomatology of TVDs, but their definition of TVDs and reported TVD symptoms varied (3,4). In one study investigating the TVDs in subjects with migraine without aura (MO), reported TVD symptoms were different from visual auras in shorter duration and occurring during the headache phase; however, it also concluded that TVDs might actually be misinterpreted as visual aura on occasion (4).
In our previous epidemiological study of headache (5), we found that many adolescent participants reported TVDs during their headaches. However, research regarding TVDs in this age group is lacking. Therefore, the purpose of the current study was to investigate the prevalence and characteristics of the TVDs and their clinical associations with headaches in a sample of adolescents.
Methods
Study design
This study was conducted by self-administered questionnaires among the ninth-grade students in two selected middle schools in Taitung County, Taiwan, in 2009. It was part of the Taitung County Adolescent Headache Survey, which was designed to investigate migraine and chronic daily headache epidemiology as well as psychological disturbances in adolescents. Details of the survey have previously been reported (5). The Institutional Review Board of the Kaohsiung Medical University Hospital approved this research protocol.
Sampled population
Compared to the other counties in Taiwan, Taitung County is less developed and less populated. Regarding the Taiwan education system, children ages 6–15 are obligated to complete schooling, with more than 90% of children enrolled in public schools and the remaining 10% attending private schools. Students ages 12–15 attend middle schools (seventh to ninth grades). For our study, we selected students from two public middle schools in Taitung County: 1) Tunghai Middle School, which is located in an urban area; and 2) Chihpen Middle School, which is located in a rural area. Official letters describing our study objectives and methodologies were mailed to the Education Department of the Taitung County Government and the school principals for their approval. All the students in the ninth grade of the two schools were invited to participate in our study, and this adolescent cohort generally represented as a community-based sample.
Survey questionnaire design
The self-administered questionnaires consisted of two parts:
A validated headache questionnaire, based on the International Classification of Headache Disorders, 2nd edition (ICHD-II) (1), to collect data on diagnosed headaches and to assess headache profiles during the past three months (including headache severity, duration, frequency, characteristics, location of the headache, accompanying symptoms and usage of painkillers). A visual phenomenon questionnaire to assess visual auras and TVDs, including patterns (zig-zag lines, flickering lights, or scotoma), laterality of the visual fields, colors, presence of movement, development time, duration and temporal relationship with headaches. More than one answer could be chosen regarding the different patterns of TVDs. The five items of the Visual Aura Rating Scale (VARS) (6) were embedded in the questionnaires and scored as follows: Duration 5–60 minutes (three points), developing gradually ≥5 minutes (two points), scotoma (two points), zig-zag lines (two points) and unilateral visual field (one point).
Visual aura and validation of VARS in an adolescent sample
The VARS score is the weighted sum of the five-item scale, with a maximum score of 10 points. A cutoff score of five or more points is used to diagnose migraine with aura (MA), with a sensitivity of 91% and a specificity of 96% in an adult population (6). We conducted a parallel study to validate the VARS-based aura diagnoses in an adolescent sample. Neurologists, who were blinded to the VARS scores, used semi-structured questionnaires to interview 59 randomly selected students: 26 of them selected from subjects with VARS score ≥ five, and 33 selected from the VARS < five group. MA diagnoses made by neurologists based on ICHD-II code 1.2 (1) were used as the gold standard. A VARS score ≥ five diagnosed as MA had a sensitivity of 73.7% and a specificity of 70%, while a VARS score ≥ four had a sensitivity of 84.2% and a specificity of 37.5%. By using a VARS score of four, the positive predictive value (PPV) for MA was 0.05 and the negative predictive value (NPV) was 0.98 based on the prevalence of MA being 3.5% in adolescents (5).
Definition of TVDs
TVDs were defined as transient visual phenomena related in time to the occurrence of a headache attack, but not visual aura. In this study, TVDs included only visual phenomena with VARS < four to exclude the potential inclusion of true visual aura.
Headache diagnoses and validation of headache questionnaires
A computer algorithm for headache diagnoses analyzed the headache questionnaires. The diagnoses of MO were based on ICHD-II code 1.1, tension-type headache (TTH) code 2.1, 2.2, 2.3, and probable migraine (PM) code 1.6, respectively (1). Those subjects who experienced headaches in the past three months but did not fulfill MO, PM or TTH requirements were defined as “other headache” (OH). In this study, migraine headaches included MO and PM, while non-migraine headaches included TTH and OH.
The sensitivity and specificity of the headache questionnaires for diagnosis of MO were 82.8% and 75.4%. As for MA, the sensitivity and specificity were 78.6% and 81.8%; and for TTH, the sensitivity and specificity were 75.8% and 77.1%, respectively (5,7).
Statistical methods
SPSS software, version 15.0, was used to conduct all statistics analyses. VARS validity was assessed by sensitivity, specificity, PPV and NPV. The Student t test, Chi square test and Chi-square for trends were used for comparisons when appropriate. The potential predicting variables for the presence of TVDs included gender, headache frequency, headache severity, headache duration, migraine diagnosis and migrainous features. Logistic regressions were used to calculate adjusted odds ratios (AORs) with 95% confidence intervals (CIs) after controlling for potential confounders. Statistical significance was established when p < 0.05 (two-tailed test).
Results
Of the total of 679 ninth graders, 663 students participated in this study, with a response rate of 97.6% (322 girls vs. 341 boys, female ratio: 47%; mean age: 15.1 ± 0.3 years old).
Prevalence of TVDs in headache subjects
For the prior three-month period, 371 adolescents (56%; 212 girls vs. 159 boys; female ratio: 57.1%) reported having at least one headache. Among them, 178 subjects (48%) experienced headache-related visual phenomena: 54 (14.6% of the 371 headache subjects; 8.1% of all the participants) had VARS score ≥four, whereas 124 (33.4% of the headache subjects; 18.7% of all the participants) had VARS <four, which we defined as TVDs. The prevalence of TVDs was higher in girls than in boys (38.2% vs. 27%, p = 0.024) among the headache subjects.
Characteristics of TVDs
The most commonly reported TVD patterns were scotoma (81 subjects, 65.3%), followed by flickering lights (73 subjects, 58.9%), and then zig-zag lines (19 subjects, 15.3%). Forty-nine subjects (39.5%) experienced two patterns of TVDs (13 had both zig-zag lines and flickering lights; whereas 36 had both flickering lights and scotoma). No one had three patterns of TVDs. Subjects with TVD of flickering lights were more likely to have TVD of zig-zag lines (17.8% vs. 2.5%, p < 0.001) or scotoma (49.3% vs. 18.4%, p < 0.001) than those without. In contrast, subjects with TVD of zig-zag lines were less likely to have TVD of scotoma than those without (0% vs. 27.2%, p = 0.008).
TVD characteristics.

The data represent the number of students who answered each questionnaire; unanswered questionnaires were interpreted as missing data; TVDs: transient visual disturbances.
Clinical correlates of TVDs
After excluding the 54 subjects with VARS ≥four, the remaining 317 adolescents with headaches were grouped into those with TVDs (n = 124, 39.1%) and those without TVDs (n = 193, 60.9%) for additional analyses. Results showed that subjects with TVDs had more frequent headaches compared to subjects without TVDs (2.7 vs. 1.6 days/month, p = 0.002). No associations were found between TVDs and headache duration (p = 0.41) or headache severity (p = 0.50).
Migraine diagnosis
The frequency of TVDs in migraine and non-migraine headaches.

TVDs: transient visual disturbances.
Migrainous features
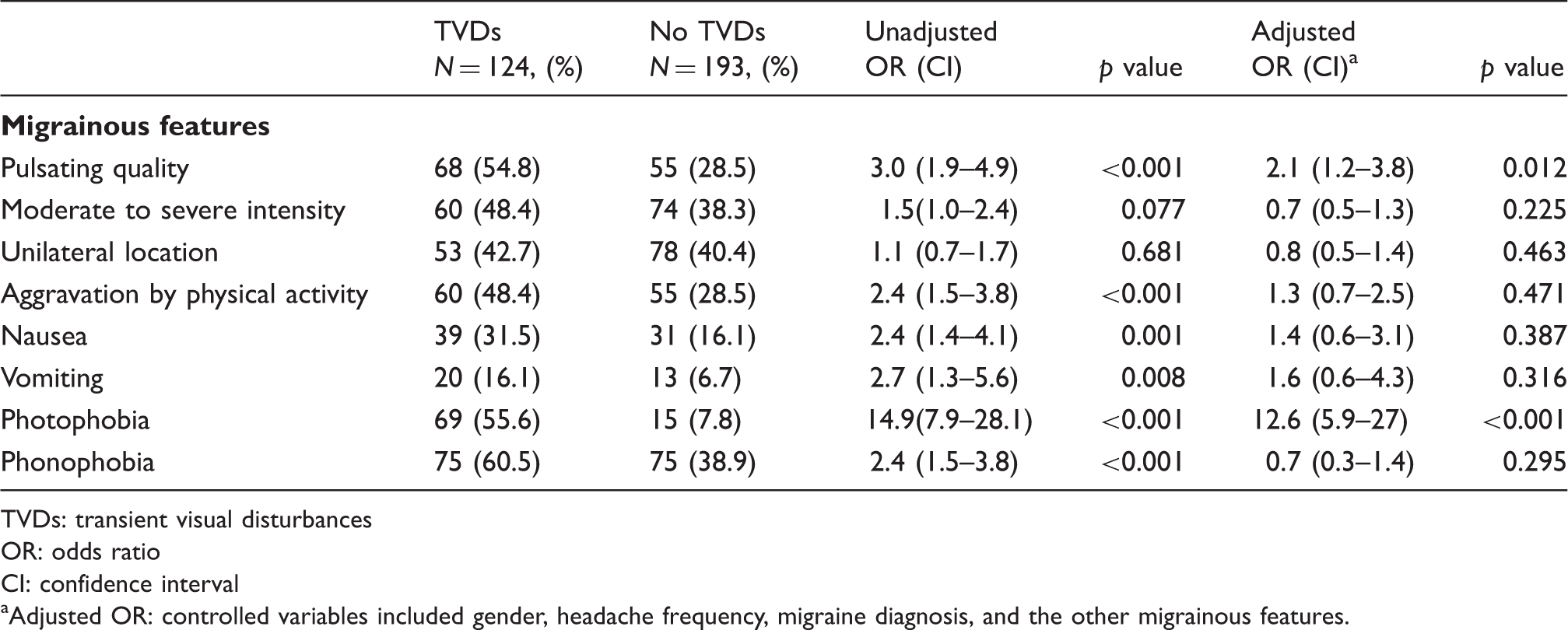
Table 3 shows the frequency of each migrainous feature between headache subjects with and without TVDs. TVDs were associated with pulsatile headache (OR = 3 (1.9–4.9)), headache aggravated by physical activities (OR = 2.4 (1.5–3.8)), nausea (OR = 2.4 (1.4–4.1)), vomiting (OR = 2.7 (1.3–5.6)), photophobia (OR = 14.9 (7.9–28.1)) and phonophobia (OR = 2.4 (1.5–3.8)). After controlling for gender, headache frequency and the presence of migraine diagnosis, TVDs were associated with pulsatile headache (AOR = 2.1 (1.2–3.8)) and photophobia (AOR = 12.6 (5.9–27)), but not the other migrainous features. In addition, we found a trend for increasing TVD frequency with increasing migrainous features (p < 0.001; numbers of migrainous features ranged from 0 to 6; moderate to severe intensity, pulsating quality, unilateral, aggravation by physical activity, nausea or vomiting, photophobia and phonophobia; see Figure 1).
The frequency of TVDs in subjects with different numbers of migrainous features (range of numbers: 0–6; moderate to severe intensity, pulsating quality, unilateral, aggravation by physical activity, nausea or vomiting, photophobia and phonophobia). Frequency and association of migrainous feature in headache subjects with and without TVDs. TVDs: transient visual disturbances OR: odds ratio CI: confidence interval Adjusted OR: controlled variables included gender, headache frequency, migraine diagnosis, and the other migrainous features.
Discussion
Our results showed that approximately one third (33.4%) of the ninth-grade students who reported headaches in the past three months also experienced TVDs. This group accounted for 18.7% of all study participants. Subjects described TVD characteristics as mainly flickering lights or scotoma; movable; monochromatic; developing and lasting less than 30 seconds; occurring over bilateral visual fields; and occurring during the headache phase. Migraineurs had a higher frequency of TVDs than non-migraineurs. In addition, as migrainous features increased, so did the TVDs frequency. Moreover, TVDs were independently associated with photophobia and pulsatile headache.
The characteristics were fairly similar among the three patterns of TVDs, but were quite different from visual aura. The co-existence of two patterns of TVDs (39.5%) in the same subject and the exclusion of the potential cases of visual aura (VARS score ≥four) may both contribute to the relatively similar features of different TVDs. Of note, the characteristics of TVDs in adults (4) were similar to those in the current adolescent sample. For example, both populations reported TVDs lasting less than 30 seconds and experienced during the headache phase. The TVD patterns in adults presented as phosphenes (53.9%), blurred vision (23.1%), scintillating scotoma (15.4%), phosphenes + scintillating scotoma (3.8%) and others (3.8%) (4). Phosphenes are similar to flickering lights, and blurred vision and scintillating scotoma may be interpreted as scotoma in our adolescents. In contrast, our adolescent subjects with migraine had a much higher frequency of TVDs than in adults with migraine (67.1% vs. 13.6%) (4). Moreover, TVDs were common in our adolescents with non-migraine headaches (31.2%). Since TVDs were associated with photophobia and pulsatile headache, a longitudinal follow-up study among non-migraine headache subjects with TVDs may determine whether TVDs predict migraines in adolescents.
The underlying mechanisms of TVDs remain unclear. The role of visual cortex hyper-excitability in migraineurs has long been debated among studies with different methodologies, including research using visual-evoked responses and transcranial magnetic stimulation (8–17). A recent neuroimaging study using H215O positron emission tomography (PET) showed that light-induced activation (600 and 1200 Cd/m2) of the visual cortex was observed in migraine subjects during the interictal phase but not in controls (18). This finding supports visual cortex hyper-excitability in migraineurs. However, this study also found that trigeminal pain potentiated visual cortex activation in migraineurs and controls (18), suggesting that trigeminal nociception may modulate visual cortex activity. We postulate that visual cortex hyper-excitability may be associated with the occurrence of TVDs, which explains why we observed TVDs more often in migraineurs than in non-migraineurs. In addition, the modulation of visual cortex activity by trigeminal pain may explain why TVDs occurred more frequently during the headache phase. Since the prevalence of TVDs is much higher in our adolescents with headaches or migraines, further research is needed to determine if the visual cortex is more hyper-excitable in adolescents than in adults.
In clinical practice, the headache-related transient visual phenomena may be misinterpreted as a visual aura (4,19–22). However, similar to research with adult subjects, our study showed that TVDs characteristics differed from visual auras in that they had shorter development time and shorter duration. Moreover, TVDs affected bilateral rather than the unilateral visual fields, and occurred during, rather than before, the headache. In addition to visual auras, epilepsy should also be differentiated from TVDs (23–25), especially childhood occipital epilepsy of Gastaut. This rare disorder has a mean age onset of 8.5 years and is characterized by brief seizures with mainly visual symptoms, such as elementary visual hallucination or less commonly, complex visual illusions (23,24). However, as distinguished from TVDs, the visual symptoms are multicolored, start from the periphery of a visual field and move to the other side, and are combined with a variety of other symptoms including ictal deviation of the eyes, eyelids closure or blinking, hemiclonic movement, automatism and secondary generalization (21,23,24). It is important to note that migraine-like headaches may occur immediately or minutes after the seizure in half of these patients (24). Transient visual phenomena have also been reported in other rare conditions, such as cerebral blood vessel diseases (26,27); and headache may also accompany these disorders.
We acknowledge that our study has several limitations. First, self-reported measurements are subject to recall bias. However, we attempted to minimize the errors in the subjects’ memory by assessing headache profiles and visual phenomena during the past three months. Second, we cannot ignore the possibility that TVDs may be secondary symptoms in a minority of subjects because we did not conduct neuroimaging, electroencephalography or neurological examinations on the participants. Third, although we had excluded subjects with VARS score ≥four, a certain portion of subjects with TVDs might still experience visual aura. Since this study adopted a retrospective rather than a prospective design, with subjects recalling but not recording the characteristics of the visual phenomenon, such as duration and unilateral or bilateral involvement of visual fields, there might be misclassification of the diagnoses. However, this chance is low (2%) since the NPV was 0.98 for MA in subjects with VARS <four. Likewise, MA subjects may have had visual aura and TVDs, but they were excluded from the TVDs cases. A fourth limitation may be our assessment of the three TVDs patterns (zig-zag lines, flickering lights, scotoma), as subjects may have experienced other patterns not addressed by the questionnaires. Finally, due to the questionnaire-based diagnosis of MO, PM and TTH, there is the possibility of headache misclassification even though the sensitivity and specificity of the headache questionnaire were more than appropriate.
In conclusion, our results showed that TVDs were common in adolescents with headaches, especially in migraineurs. Moreover, TVDs were associated with photophobia and pulsatile headache, and both were independent of migraine diagnosis.
Footnotes
Funding
This study was supported in part by grants from Taiwan National Science Council (100-2314-B-010-019-MY2, 100-2314-B-010-018-MY3), Taipei-Veterans General Hospital (VGHUST101-G7-1-1, V101C-106, V101E7-003), NSC support for the Center for Dynamical Biomarkers and Translational Medicine, National Central University, Taiwan (NSC 100-2911-I-008-001), Brain Research Center, National Yang-Ming University and a grant from Ministry of Education, Aim for the Top University Plan.
Conflict of interest
Dr S-J Wang has served on the advisory boards of Pfizer, Allergan, and Elli Lilly, Taiwan. He has received speaking honoraria from local companies (Taiwan branches) of Pfizer, Elli Lilly, Boehringer Ingelheim and GSK. He has received research grants from the Taiwan National Science Council, Taipei-Veterans General Hospital and Taiwan Headache Society. Dr J-L Fuh is a member of a scientific advisory board of Elli Lilly, and has as well received research support from the Taiwan National Science Council, Taipei-Veterans General Hospital and Elli Lilly.