
Abstract
Background:
Takotsubo cardiomyopathy is a form of non-ischemic cardiomyopathy that may be acutely precipitated by stress. A number of neurologic conditions have been implicated in precipitating this disease such as subarachnoid hemorrhage, stroke, and seizures. Its association with status migrainosus, however, has never been described before.
Case:
We report a case of a 25-year-old female presenting with status migrainosus followed by takotsubo cardiomyopathy. Supportive management was instituted in this patient and she made an excellent recovery.
Conclusion:
The intense pain associated with migraine may have acted as a stressor, thereby precipitating takotsubo cardiomyopathy. To our knowledge, this is the first reported case demonstrating a relationship between status migrainosus and takotsubo cardiomyopathy.
Keywords
Introduction
Takotsubo cardiomyopathy (TC), also known as stress-induced cardiomyopathy (SICM), broken heart syndrome, or apical ballooning syndrome has been described in the setting of intense physiologic or emotional stress (1). It has also been reported in the setting of a number of acute neurological illnesses including subarachnoid hemorrhage, stroke, and seizures (1). The presentation of TC is similar to that of acute coronary syndrome but without evidence of coronary artery stenosis on coronary angiogram. We report a case of TC apparently precipitated by status migrainosus.
Case report
A 25-year-old female presented with a 4-day history of intense, throbbing, holocranial headache associated with photophonophobia and intense nausea. There were no visual or sensory auras. The headache was similar to her previous headaches except that it was unremitting with acetaminophen and ibuprofen. She had a history of episodic headaches since her early teens. On average, she would get one severe headache and three mild headaches per week, each lasting a few hours to a day. However, this was her first severe headache lasting for more than 3 days. She had been treated with amitriptyline, topiramate, propranolol, and doxepin with no improvement in her headache frequency and/or intensity. At presentation, she was taking valproic acid (VPA) 500 mg twice a day for prophylaxis against migraines. For abortive therapy, she was treated with sumatriptan and eletriptan, which did not abort her headaches; therefore she had stopped taking them. She used over the counter non-steroidal anti-inflammatory agents for abortive therapy more than three times a week. She smoked cigarettes and occasionally used marijuana but there was no history of excessive caffeine intake or undue stressors. On the fourth day of continuous headaches, she presented to the hospital with sudden onset of chest pain and shortness of breath. She denied any social stressors preceding the event except for disabling headaches causing significant distress. She had no other past medical history except for hypertension for 5 years. She had had a work up for secondary hypertension in the past, but this was negative. Her plasma-free metanephrine and normetanephrine were normal. Abdominal magnetic resonance imaging (MRI) did not show any evidence of pheochromocytoma. Metaiodobenzylguanidine (MIBG) radionuclide scan was not performed, as extraadrenal pheochromocytoma was not suspected. Her gynecological and obstetric history was not significant. On examination, her blood pressure (BP) was 150/76 mmHg and she was tachycardic with a heart rate of 120 beats per minute. Neurologic examination was normal, including a normal fundoscopic exam.
She had diffuse ST elevation in leads II, III, aVF, V2-4 on electrocardiogram (EKG) (Figure 1) and elevated troponins at 0.69 (normal range 0.00–0.04 ng/ml) with an elevated B-type natriuretic peptide (BNP) of 2829 pg/ml (normal 0–120 pg/ml). A transthoracic echocardiogram revealed severe hypokinesis of mid to distal segments with dilatation of the apex; suggestive of apical ballooning or takotsubo cardiomyopathy (Figure 2). Her left ventricular ejection fraction was estimated at 25–30%. Her coronary arteries were normal on angiogram. There was no evidence of fixed coronary stenosis nor was there any evidence of spontaneous coronary artery spasms. However, provocative agents were not used to induce spasms.
A 12-lead electrocardiogram showing diffuse ST segment elevation; most prominent in leads II, III, and aVF, V2, V3, and V4. Transthoracic echocardiogram (a) depicting left ventricular apical ballooning and hypokinesia during systole. The shape has been outlined in white marking. Note the characteristic resemblance to the “takotsubo” or the “octopus trap”. Cardiac MRI (b) of the patient showing dilated left ventricle during diastole.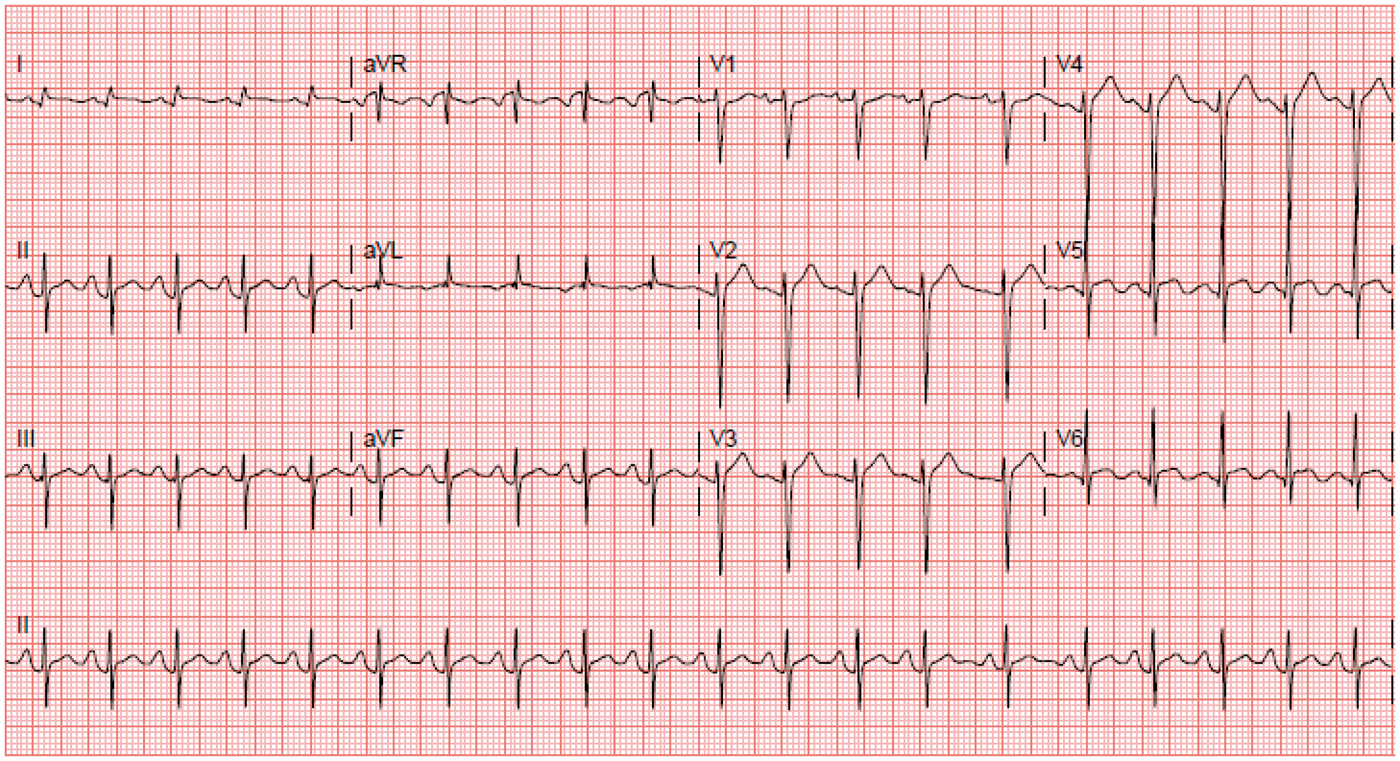

She also underwent cardiac MRI, which showed similar findings of left ventricular dysfunction (Figure 2). She was treated with oxygen, beta-blocker, angiotensin converting enzyme (ACE) inhibitor, and aspirin. Her symptoms of chest pain and dyspnea improved in a day but she continued to complain of headaches during her hospital stay. She underwent MRI of the brain and magnetic resonance venogram (MRV) of the head to look for possible venous sinus thrombosis; both of which were normal. Her cerebrospinal fluid (CSF) studies including opening pressures were also normal. Her urine toxicology was negative for illicit drugs. A diagnosis of status migrainosus was made based on the International Classification of Headache Disorders-2 (ICHD-2). She was treated with intravenous infusion of VPA, to which she responded well. A transthoracic echocardiogram was repeated a week later, and showed improving left ventricular function. Her estimated left ventricular ejection fraction was about 35% and her headaches and dyspnea had improved at discharge. However, her EKG changes were still present at discharge. She was discharged with instructions to quit smoking, maintain a low salt diet, and medicines that included aspirin, carvedilol, VPA, and lisinopril. As she had responded well to intravenous VPA in the hospital, she was discharged on VPA 750 mg twice a day for prophylaxis against migraines. She was also instructed to have a close follow up in our neurology and cardiology clinics.
On a subsequent clinic visit, her BP was 130/74 mmHg. After 6 weeks, a repeat EKG showed normal sinus rhythm. However, she failed to attend the repeat echocardiogram. As other potential causes for her cardiomyopathy were investigated and ruled out, this makes TC the most plausible cause for her presentation.
Discussion
A “takotsubo” is a pot used to trap octopus in Japan (1). The abnormalities on echocardiogram, cardiac MRI, and left ventriculogram seen in TC resemble a flask with a short neck and a wide, rounded body, hence the name “takotsubo” (1,2). Initial reports of this condition have been mainly from Asian countries, but more recently it has been recognized all over the world. It is more prevalent in postmenopausal women and has a female preponderance (1). It has been associated with a variety of conditions, some of which may be as trivial as coughing (3) and diving (4). The exact pathophysiology is debatable, but catecholamine-induced myocardial stunning is the most favored of the proposed mechanisms (5).
TC is a reversible acute heart failure that mimics acute coronary syndrome. Elevated cardiac troponins and BNP, ischemic abnormalities on EKG, apical to mid ventricular ballooning but sparing of basal myocardium on echocardiogram, and no significant coronary artery stenosis or thrombus on coronary angiography are helpful for diagnosis (1). There is an increasing literature on the role of serum level of N-terminal prohormone of brain natriuretic peptide (NT-pro BNP) as both a diagnostic and prognostic marker. It has been shown to correlate well with the extent of catecholamine release in TC and the severity of left ventricular dysfunction. Lower levels of NT pro-BNP at admission are associated with favorable prognosis in patients with TC (6). NT-pro BNP was not measured in our patient, as the presentation and the echocardiogram were highly suggestive for TC.
The differential diagnosis in this case includes viral myocarditis (VM), given the clinical presentation. A preceding viral illness is seen in most cases; however, our patient denied any preceding illness. Coxsackie virus, Epstein Barr virus, and cytomegalovirus serology were negative. Cardiac MRI showed no enhancement within the myocardium but myocardial biopsy was not pursued. Ischemic cardiomyopathy was also an unlikely diagnosis given the young age of the patient and absence of coronary disease on coronary angiography. Cocaine use has been implicated as a cause of acute cardiomyopathy in young patients (7). Our patient underwent a urine toxic screen, which was negative.
Various pharmacologic agents have been associated with TC. Drugs reported to have association with TC include dobutamine, duloxetine, venlafaxine, 5-flurouracil, epinephrine, and a few others mentioned in a report by Amariles (8). The patient was not currently on any drugs that have been linked to TC. It is plausible that some drugs that increase circulating catecholamines by blocking their reuptake may present a risk for developing TC. Amitriptyline, nortriptyline, and doxepin, commonly used for migraine prevention, can cause an increase in circulating plasma catecholamines. However, no cases of such association have been reported with the commonly used dosages. Our patient was on amitriptyline and doxepin 2 years prior to presentation. Hence, it is less likely that the TC was related to this.
It is unusual for TC to occur at this age. In one systematic review, the age of presentation of TC varied from 10 to 89 years with a median age of 58–77 years. About 2.7% of cases do occur in patients under 50 years of age, and 88% occur in postmenopausal women (2).
Autonomic nervous system function in patients with TC has shown a transient increase in sympathetic activity and decrease in vagal activity. In rat models the electrographic and left ventriculographic changes can be prevented by combined blockade of alpha and beta adrenoceptors. Estrogen supplementation may also partially block this effect of TC. Estrogen treatment in rat models has been shown to increase levels of cardioprotective substances, such as atrial natriuretic peptide and heat shock protein 70, in the heart. These data from rat models suggest that a decline in estrogen level post menopause may be the primary cause of TC, both by the indirect action on the nervous system and also by direct action on the heart (9). Hence, estrogen may have a protective effect on the development of TC, as it is much more common in postmenopausal women.
It is interesting to note that vasospasm has been linked to the pathogenesis of both migraine and TC. However, the fact that region of wall motion abnormalities in TC do not correspond to a single coronary artery territory argues against the hypothesis of epimyocardial vasospasm as a pathogenesis of TC. Also, in a systematic review, only 1.4% of patients were found to have spontaneous multivessel epicardial spasm. Using provocative tests with the use of ergonovine and acetylcholine, only 28% had multivessel spasms; hence vasospasm as a pathogenesis for TC seems unlikely (2). Related to the pathophysiology of migraine, it was once believed that migraine aura was primarily due to cerebral ischemia as a result of cerebral vasospasm and the headache itself was the result of reactive vasodilatation. However, blood flow studies do not entirely support this theory, hence the role of vasospasm in migraine is less likely (10).
The majority of patients make an excellent recovery with supportive management without the need for thrombolytics. For example, heart failure is effectively treated with beta-blockers, ACE inhibitors, and diuretics. Cardiac function typically recovers in less than a month (2). In one series, heart failure with or without pulmonary edema was the most common complication (2) but mortality rates were quite low, ranging from 0% to 8% (1). In one systematic review, the rate of recurrence was about 3.5% (2).
In our patient, we felt that the status migrainosus may have triggered takotsubo cardiomyopathy based on the observation that symptoms of her intractable headaches preceded the cardiomyopathy. Although it is plausible that status migrainosus did not precipitate TC in this patient, the intense headaches leading to undue distress and the lack of any other obvious stressors argue in favor of a causal relationship between the two disease states. Furthermore, increased catecholamine levels have been proposed as the underlying pathophysiologic basis for TC (5). Interestingly, increased catecholamine levels are also seen in patients with migraine (11). However, catecholamine levels were not measured during the current admission.
Conclusion
TC has been described in the setting of ischemic stroke, hemorrhagic stroke, seizures, and subarachnoid hemorrhage (1,12). There are no reported cases of migraine being associated with this condition. Its association in the setting of migraines may be under-recognized. Complaints of chest pain and shortness of breath are often attributed to anxiety in the setting of migraines, especially in younger patients. Neurologists should be aware of the possibility of stress-induced cardiomyopathy while treating patients with migraine.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.