
Abstract
Objective: This study was conducted to characterize prescription refill patterns for triptans among European patients with new prescriptions of triptans.
Background: Persistency with prescriptions of triptan monotherapy for migraine headache among newly prescribed users in European primary-care practices has not been well described.
Methods: Using electronic medical databases in the UK (N = 3618), France (N = 2051) and Germany (N = 954), we conducted a retrospective cohort analysis to identify refill patterns over 2 years among migraineurs receiving new prescriptions of triptan monotherapy in 2006.
Results: Of all patients, >33% of migraineurs with new triptan prescriptions received ≥1 refill of their index triptan prescriptions (UK, 44.3%; France, 34.2%; Germany, 37.7%). More than 50% never received index-triptan refill prescriptions (UK, 55.7%; France, 65.8%; Germany, 63.3%). Small proportions of patients (<7.0%) switched to alternative triptans, and even fewer switched to different prescription-medication classes (UK and Germany, 2.3%; France, 4.0%). More than 48% of patients received no further prescriptions for migraine after index prescriptions (UK, 48.5%; France, 54.9%; Germany, 54.7%). After the second year, >83.0% of patients in each country had no further prescriptions for migraine medications, <14.0% remained persistent with index prescriptions, <4.0% switched to other triptans, and <3.0% switched to alternative medication classes.
Conclusions: In migraine patients who received new prescriptions of triptan monotherapy from their primary-care physicians, poor triptan prescription refill frequency was observed in Europe. Although consistent with potential clinical challenges in migraine management, our findings should be interpreted with caution given certain inherent limitations associated with the database study design. Further research is warranted to confirm our findings and to identify reasons for, or predictors of, triptan discontinuation.
Introduction
Migraine headache is a disabling, chronic-intermittent, neurovascular condition that is considered one of the most common neurological disorders in Europe (1–3). Marked by acute paroxysmal attacks lasting from 4 hours to 3 days, migraine results in neurological, gastrointestinal and/or autonomic changes (4). The disorder affects 12–28% of Western Europeans at some time in their lives, with a female: male proclivity of 3:1; symptoms are also generally more severe in women (4–9).
Across the world, approximately 324 million patients have migraine; of the 41 million migraine patients in Europe, there are approximately 5.4 million in the UK, 4.9 million in France, and 7.1 million in Germany (4,9,10). Headache disorders, including migraine, rank among the top 10 causes of disability in Europe, and the degree of debilitation from severe migraine has been compared to that of psychosis or dementia (11–13).
Migraine often strikes patients during their most productive years (14); is frequently comorbid with depression, anxiety or increased irritability (15); and is characterized by variable and unpredictable attacks (16). Given these factors, migraine perhaps uniquely compromises quality of life, limiting a patient’s ability to work, study, interact with family, and enjoy social and leisure time, as well as eliciting anxiety between attacks (12,17,18). By various estimates, the annual societal cost of migraine is €27 billion in Europe, including €3.2 billion in the UK, €3.6 billion in France and €6.1 billion in Germany (8,10).
Consensus guidelines for acute migraine management have been issued by the British Association for the Study of Headache (BASH), the European Federation of Neurological Societies (EFNS) and the European Headache Federation (EHF), in collaboration with the World Health Organization and other treatment panels (5,8,19–21). Migraine-specific agents such as serotonin (5-hydroxytryptamine/5-HT1B/1D) agonists (triptans) and ergot alkaloids are considered first-line therapies for patients who have no contraindications and experience moderate-to-severe (MIDAS [Migraine Disability Assessment] (22) Grades III–IV) migraine or less severe migraine that is refractory to treatment with non-specific (non-opioid) analgesics (5,23–25).
Oral triptans rapidly relieve headache and associated symptoms when administered early in the attack, conferring pain relief at the second post-treatment hour in approximately 60–70% of patients (with most triptans) and complete freedom from pain at this time point in up to 40% (with rizatriptan 10 mg) (5,26–32). In clinical studies, these medications also ameliorated a broad spectrum of patient-centered outcomes (33,34).
In general, medication treatment outcomes are influenced by both the degree of agreement between a patient’s own, and prescribed, medication-taking behaviours (i.e. compliance or adherence) as well as the duration of medication use (i.e. persistency). Compliance or adherence signifies ‘the extent to which a patient acts in accordance with the prescribed interval and dose of a … regimen’, whereas persistency denotes the ‘time from initiation to discontinuation of therapy’ and is consistent with a patient continuing to take any amount of medication over time (35,36). Persistency can be expressed as either a continuous variable (e.g. days persistent) or as a dichotomous variable defined as a percent persistency over a pre-specified interval (e.g. 12 months) (35).
In a recent US pharmacy claims database analysis, 53.8% of patients receiving initial triptan prescriptions for migraine from 2001 to 2005 did not persistently refill these index prescriptions even once over 2 years (36). Approximately one-quarter (25.5%) discontinued prescription migraine therapy altogether, 67.0% switched to non-triptans, and 7.4% switched to alternative triptans. Only 10% of American triptan-naïve patients remained persistent to index triptans over the 2-year follow-up period. It is unknown whether the US triptan persistency pattern is also observed in non–US societies, including within Western Europe. The present, similarly designed, study of an electronic medical database was undertaken to assess triptan persistency and other migraine prescription drug use patterns among a large European cohort of newly prescribed triptan users in primary-care settings over a 2-year observation period.
Methods
Study design
This analysis was a retrospective cohort study of the IMS Disease Analyzer (IMSDA; Norwalk, CT; www.imshealth.com), a longitudinal electronic patient database containing de-identified (anonymized) records of patients seen by office-based physicians (mainly general practitioners [GPs]) in France, Germany and the UK. IMSDA provided access to a representative panel of approximately 630 physicians treating 3.6 million patients in the UK; 977 physicians treating 1.8 million patients in France; and 1045 physicians treating 6 million patients in Germany. The database included 15.7 million individual patient records with up to 19 years of history each. Patient record data were extracted directly from physicians’ computer systems. Data included drug names, indications for prescribing, administration routes, dosage strengths, fill dates and days of supply.
Study sample
Eligible for inclusion were migraineurs initiated on triptans in 2006 and followed for up to 2 years from the date of the first triptan prescription (i.e. ‘index date’). To preserve homogeneity within the cohort, the index date marked the day of the first prescription of oral triptan monotherapy and not of oral triptans in combination with other formulations or medications.
Data for each patient were collected for each interval over a total of 3 years: 1 year before the index date (i.e. ‘baseline period’) and 2 years after this date (i.e. ‘follow-up period’), as shown in Figure 1.
Study design and criteria used to define patient cohort selection. Within 1 year before the date of the first triptan prescription (i.e. index date), no eligible patient had an ICD-10 diagnosis of migraine; prescription for a disease-specific therapy (i.e. triptan or ergot alkaloid); or a prescription non-specific therapy linked to a diagnosis of migraine. Patient follow-up was for 2 years after the index date. In the UK, all patients had to be registered under the care of a general practitioner for ≥1 year before, and ≥2 years after, the index date. Dx: diagnosis; ICD-10: International Classification of Diseases and Related Health Problems, 10th edition.
Patients aged ≥18 years who received a prescription for a triptan from 1 January to 31 December 2006 were eligible. Within 1 year before the index date, the following categories of patients were eligible for the analysis: (i) individuals who did not have a previously documented International Classification of Diseases and Related Health Problems, 10th edition (ICD-10) diagnosis of migraine (G43); (ii) those who had no prescription of a triptan or ergot alkaloid; and (iii) those who also had no prescription of a non-specific therapy linked to a diagnosis of migraine. (Patients with prescriptions of non-specific therapies not written specifically for migraine 1 year before the index date were also excluded.) In the UK, patients were further required to be registered with their GPs for ≥1 year before, and ≥2 years after, the index date. Each patient was followed for 2 years from the index date to evaluate triptan persistency, switching or discontinuation.
Migraine-specific therapies included oral almotriptan, eletriptan, frovatriptan, naratriptan, rizatriptan, sumatriptan and zolmitriptan, as well as ergot alkaloids (e.g. ergotamine, dihydroergotamine [DHE]). To ascertain prescriptions of non-specific medications written specifically for migraine, we referred to relevant ICD-10 codes.
Definitions
Potential refill patterns and classifications are summarized in the supplementary figure in the Appendix. Patients were terminally classified at the time of each acute migraine medication prescription into the following categories: persistent included patients who continued to refill their index triptans (contiguous prescriptions of the index triptan); within-class switchers were individuals who switched to another triptan from the index triptan; between-class switchers were those who switched to another, non-triptan medication from the index triptan; and discontinuers were those who received no further specific or non-specific migraine prescriptions during the remaining follow-up period.
Measures and data analysis
Descriptive statistics for baseline characteristics were computed by country, including mean patient age and the number (%) of women in the cohort. Baseline comorbid conditions and concomitant medications were identified using appropriate ICD-10 or Anatomical Therapeutic Chemical (ATC) classification codes, respectively. At each refill, overall rates and percentages of persistency, switching and discontinuation were computed. The probability of persistency at the jth refill in each country was computed as the number of patients with j consecutive refills of the index triptan, divided by the total number of patients in the index population. The probability of persistency between refills was calculated by dividing the number of patients with j − 1 refills by the number of patients with j consecutive refills. Probabilities of within-class switches, between-class switches and discontinuations were computed in a similar manner. Numbers and percentages of each of these outcomes (or censored patients) were provided by each refill through a total of seven possible refills (eighth prescription; or 2 years) in each country.
Results
Baseline characteristics
In all, 3618 patients with migraine in the UK, 2051 in France and 954 in Germany were included in the cohort (N = 6623; Figure 2). More than 75% of patients in each country were women (Table 1).
Eligibility criteria and data flow to arrive at final cohort (N = 6623). Baseline demographic and clinical characteristics for all patients (N = 6623). Frovatriptan and rizatriptan were not marketed in France. Percentages do not add to 100 because of rounding. NA = not applicable.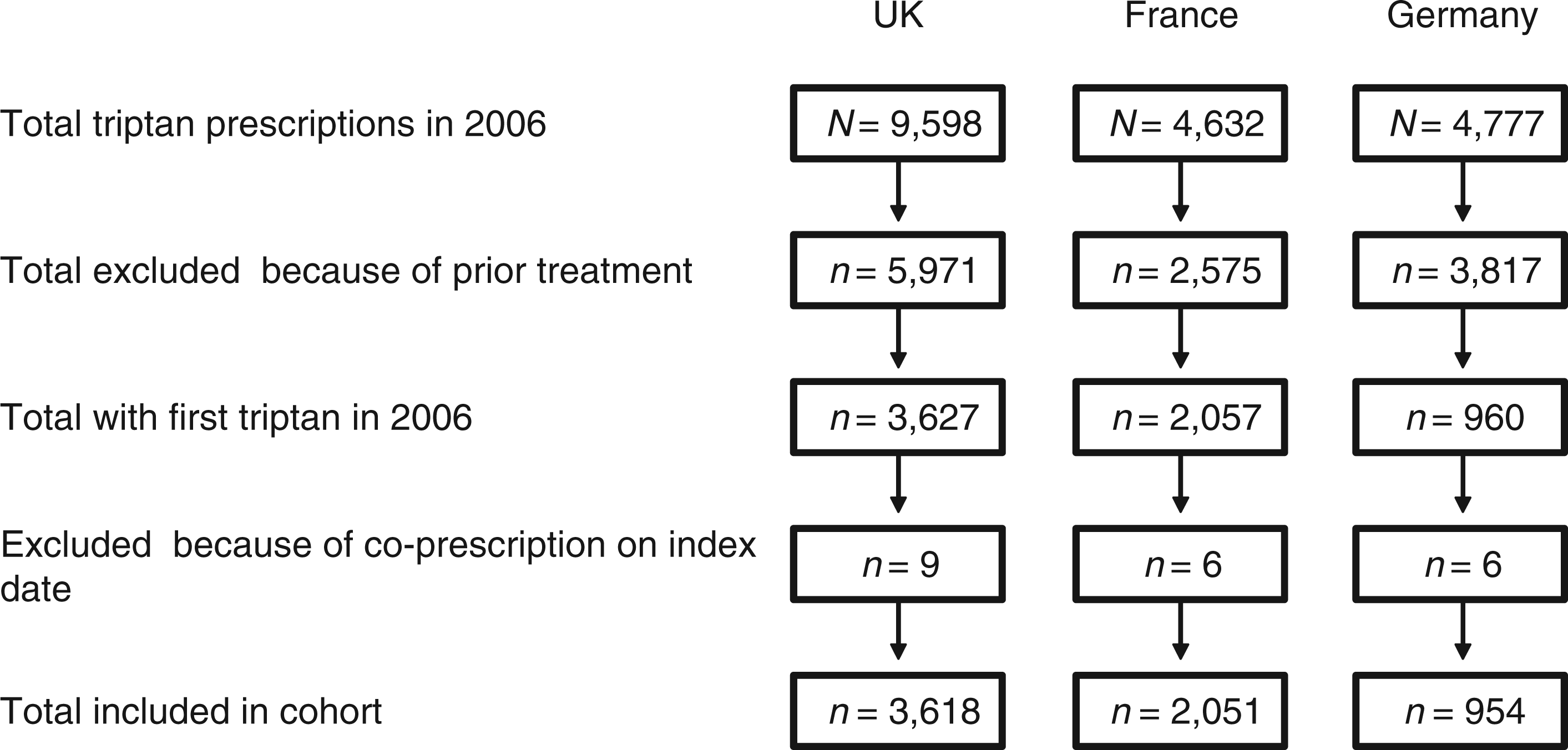

By country, leading index triptans (in descending order of frequency) were sumatriptan, rizatriptan and zolmitriptan in the UK; zolmitriptan, eletriptan and almotriptan in France; and rizatriptan, frovatriptan, sumatriptan and zolmitriptan in Germany (Table 1). Rizatriptan and frovatriptan were not marketed in France.
Follow-up data: findings across countries
Triptan prescriptions at the first refill
Most (>55%) patients never received a refill prescription of their index triptans (Figure 3). Triptan prescription refill rates declined over time, with the steepest decreases occurring between the index date and the projected date of the first refill. In the UK, 2016 (55.7%) of 3618 patients did not receive a consecutive refill of their index triptan, whereas 527 (14.6%) were persistent to their index triptan for only one additional fill. Corresponding data in France were 1349 (65.8%) of 2051 patients not receiving a consecutive refill of their index triptans and 302 (14.7%) being persistent for one additional fill. In Germany, 604 (63.3%) of 954 patients did not receive a consecutive refill of their index triptan and 131 (13.7%) were persistent to the index triptan for one additional fill.
Consecutive triptan refills, by proportion of patients (N = 6623) over a 2-year follow-up period, by country. In the UK, 2016 (55.7%) patients did not receive a consecutive refill of index triptans, whereas 527 (14.6%) were persistent to index triptans for only one additional fill. Corresponding data in France were 1349 (65.8%) patients not receiving a consecutive refill of index triptans and 302 (14.7%) being persistent to index triptans for only one additional fill. Corresponding data in Germany were 604 (63.3%) patients not receiving a consecutive refill of index triptans and 131 (13.7%) being persistent to index triptans for only one additional fill. Triptan refills declined across refill counts through the fifth as a percentage of the total sample population in each country.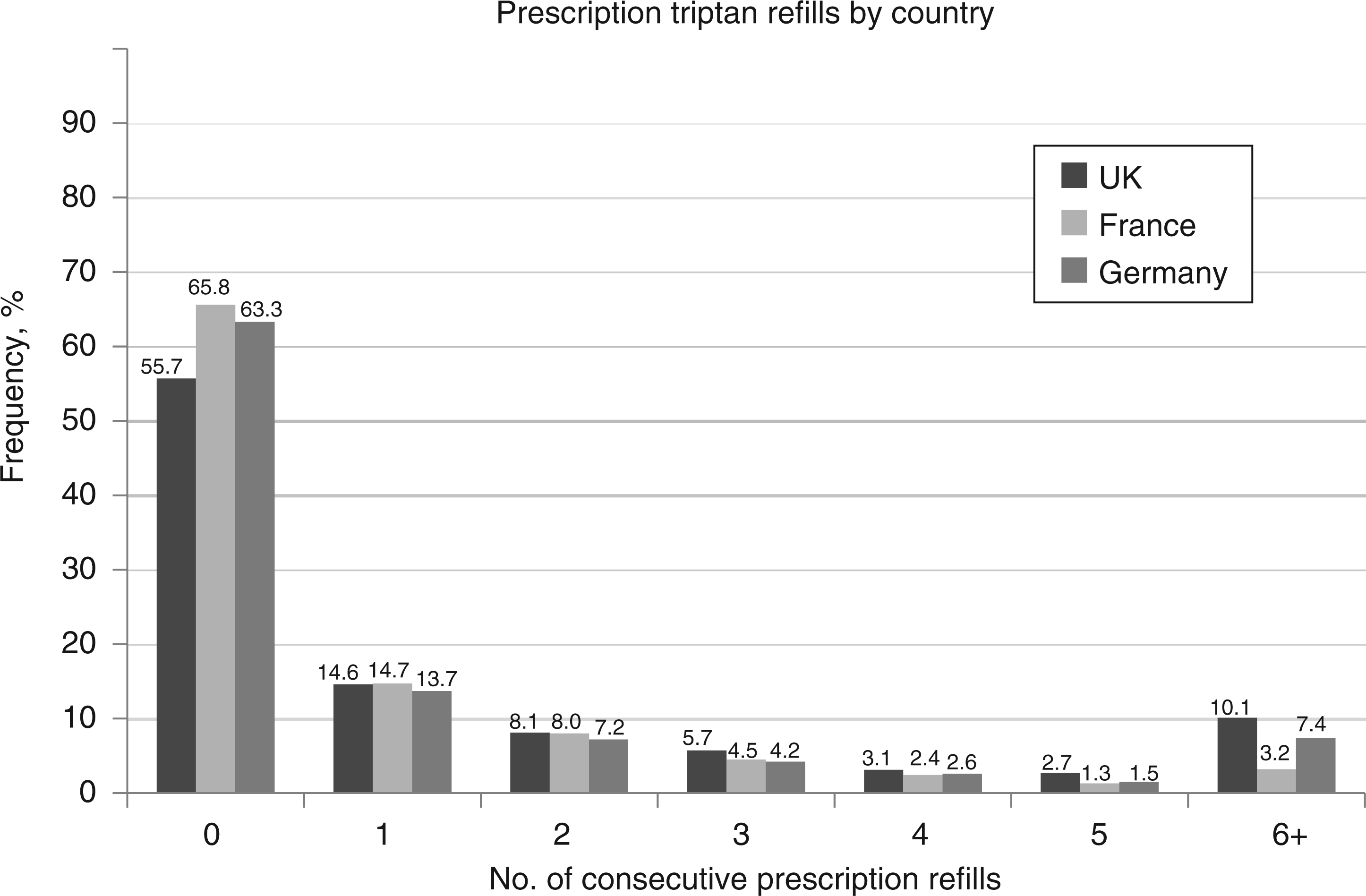
Only a small proportion of patients in each country persisted with triptan prescription fulfilment for six or more refills over the 2-year follow-up period (Figure 3).
A similar medication usage and switching pattern after the initial triptan prescription was observed across the UK, France and Germany (Figure 4). A total of 34.2–44.3% of newly prescribed triptan users persisted (for one or more consecutive triptan refills) with triptan prescriptions over the 2-year follow-up period. Smaller proportions of patients (<7.0%) switched to alternative triptans (i.e. within-class switches): 4.9% in the UK, 6.8% in France and 6.3% in Germany. Even fewer switched to different classes of prescription medication (i.e. between-class switches): 2.3% in the UK or Germany and 4.0% in France. However, large proportions of patients (>48%) received no further prescription for migraine after the index triptan prescription: 48.5% in the UK, 54.9% in France and 54.7% in Germany.
Triptan refill and other migraine medication patterns after the initial (index) triptan prescription in the UK, France and Germany, at the time of the first refill (left-hand columns) and at the end of the second year (right-hand columns). In each country <45% of patients were persistent with their index triptans at the time of the first refill. At the end of the second year, <14% of patients were persistent with their index triptan prescriptions, and >83% received no further prescriptions for migraine medications at all. Some percentages do not sum to 100 because of rounding.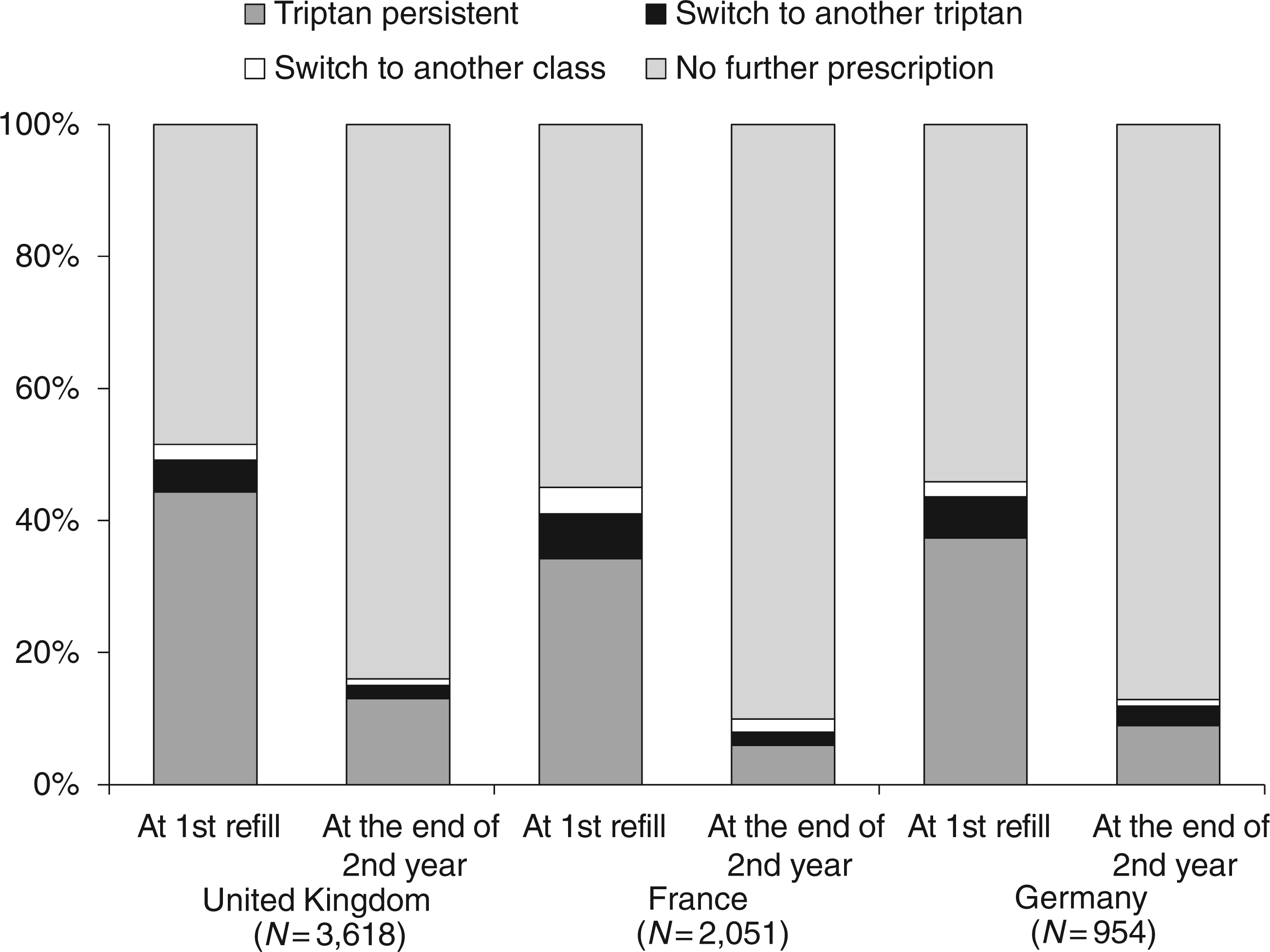
Triptan prescriptions at the end of 2-year follow-up
At the end of 2 years, >83% of patients in each country received no further migraine medication prescription, and <14% were persistent with their index triptans (Figure 4). In the UK, 84.0% of patients had no further prescription for migraine medications at the end of 2 years, 13.0% remained persistent with their index triptans, 2.0% switched to alternative triptans, and 1.0% switched to other classes of migraine medication. In France, 91.0% of patients received no further migraine prescription at the end of 2 years, only 6.0% remained persistent with their initial triptans, and 2.0% each switched to other triptans or alternative classes of medication (percentages do not sum to 100 because of rounding). In Germany, 88.0% of patients received no further migraine prescription at the end of 2 years, 9.0% remained persistent with their index triptans, 3.0% switched to other triptans, and 1.0% switched to other medication classes (percentages do not sum to 100 because of rounding).
Follow-up data: findings by country
UK
Within-class switching of prescription migraine medications, by country.

NA = not applicable (frovatriptan and rizatriptan were not marketed in France).
Between-class switching from index triptans to other prescription migraine medications, by prescription refill number and country.

Numbers of individual between-class prescription medication switches sum to values greater than the single-count totals because some individuals switched to prescription medications from more than one pharmacological class.
A/E = antiemetic; A/P = antipyretic; NNA = non-narcotic analgesic; NSAID = non-steroidal anti-inflammatory drug.
France
Of the 139 (6.8% of the entire French cohort) patients who switched to alternative triptans after their index prescriptions, frequent regimen alterations included changes from zolmitriptan to almotriptan (n = 30, 21.6% of within-class switchers) or to eletriptan (n = 20, 14.4%), and also from almotriptan to eletriptan (n = 18, 12.9%) (Table 2). Switches from or to sumatriptan were less frequent in France than the UK.
Among the 83 French patients (4.0% of the entire French cohort) who switched to alternative prescription medication classes after their index triptan prescription fills, 69 (83.1% of French between-class switchers) chose NNAs, antipyretics or analgesic/anti-emetic combinations (Table 3). A further 42 (50.6%) switched to prescription NSAIDs, as either monotherapy (n = 28, 33.7%) or combination therapy (n = 14, 16.9%); and 13 (15.7%) switched to ergot derivatives, either alone (n = 11, 13.3%) or as ergotamine combination regimens (n = 2, 2.4%). No patient switched to an opioid or barbiturate.
Germany
In Germany, 60 (6.3%) of 954 patients with migraine switched to other triptans after their initial triptan prescriptions. Among these regimen alterations, sumatriptan was the most common triptan that patients switched to, especially at refill 1. In particular, frequent within-class switches included rizatriptan to sumatriptan (n = 26, 43.3% of within-class switchers) or from either zolmitriptan or frovatriptan to sumatriptan (n = 12 [20% of within-class switchers] each) (Table 2).
Among the 22 German patients (2.3% of the entire German cohort) who switched to non-triptan medication classes, 12 (54.5% of German between-class switchers) switched to prescription NSAIDs; and 9 (40.9%) to prescription NNAs, antipyretics or analgesic/anti-emetic combinations (Table 3). One patient (4.5%) switched to an ergot derivative, and no patient switched to a prescription opioid or barbiturate.
Discussion
In our retrospective cohort analysis of an electronic medical database involving only prescription medications (i.e. no over-the-counter [OTC] remedies), <45% of European patients with initial triptan prescriptions for migraine refilled these prescriptions at the estimated time of the first refill or afterwards. Approximately 55−66% of patients did not receive triptan prescription refills after their index triptan prescriptions. Smaller proportions of patients in all three countries switched to alternative triptans (5−7%) or to other prescription medication classes (2−4%) after the initial triptan prescription fill. Large proportions of patients (>48%) received no further prescription for migraine after their index triptan prescription. At most, approximately 10% of European migraine patients continued to fill triptan prescriptions at the end of the 2-year follow-up period. The likelihood of refilling triptan prescriptions declined sharply after the initial fill, and most regimen alterations in general occurred around the projected time of the first triptan prescription refill. At the end of the second year, >83% of patients in each country received no further prescriptions for migraine medications, <14% remained persistent with their initial triptans, 2−3% switched to other triptans, and 1−2% switched to other classes of migraine medications.
These findings are consistent with the existence of a clinical challenge, mainly in patients with moderate-to-severe migraine who receive new triptan prescriptions from their existing primary care physicians. The challenge to increase triptan refill frequencies also represents a potential opportunity for primary care physicians, other clinicians and pharmacists to counsel patients about their disease and its management. Given that triptan prescription fill and refill frequencies decreased sharply after the index triptan prescription in our cohort, it may be important to focus on the early post-index-prescription window in order to sustain prescription-filling behaviours over time. This process might include eliciting patient expectations for, and experiences with, their medications; adjusting dosages to enhance patient toleration and acceptance; and otherwise maximizing treatment benefits. A prospective study would be needed to rigorously determine whether allocating additional time to such early counselling is effective (and cost-effective vs. usual care) in increasing triptan prescription refill frequency in particular and optimizing patient experiences with their medications in general.
Our observations extend data from a previous, similarly designed US retrospective cohort study of a pharmacy claims database by Katić et al. (36). In that study, approximately 54% of newly prescribed triptan users did not have consecutive index triptan refills after their initial prescriptions (36), compared with approximately 56−66% of European patients in our study (see further details below). US patients were least likely to persist with treatment from the time of the index triptan prescription to the first refill. Similar proportions of patients in each study were persistent with their index triptan prescriptions for one additional fill: 12.8% in the US claims database analysis (36) compared with 13.7−14.7% in the present study. A smaller proportion of the US (vs. our European) cohort discontinued prescription migraine therapies altogether at the time of the first medication refill: 25.5% compared with approximately 49−55% of European patients (36). It is somewhat disconcerting that approximately one of four US migraineurs in the study by Katić et al. (36), and one of two European migraineurs in the present study, did not receive adequate prescription migraine-specific treatment over a 2-year period. However, this conclusion may be mitigated by further OTC medication use or non-pharmacological therapies, which these studies did not assess and which may have conferred additional headache relief in a substantial proportion of these patient cohorts.
Other explanations for our low triptan-refill data are also plausible, including the possibility that some patients experienced exacerbations of migraines that resolved spontaneously. Approximately 7% of newly prescribed US triptan users switched to alternative triptans (36), a similar value to the 5−7% observed in our study.
In contrast, US patients were more likely (vs. our European cohort) to switch to prescription non-triptan therapies at their first prescription refills. Of 40,892 US patients with migraine receiving an initial triptan prescription in the study by Katić et al. (36), 22,031 (53.8%) did not receive a consecutive index triptan refill. Among this smaller patient subset, 14,770 (67.0%) switched to non-triptan prescription medications at the first refill (36) compared with only 2.3−4.0% in our European cohort. A total of 7455 US between-class switchers – 50.5% of all between-class switchers and 33.8% of all patients without a consecutive triptan refill – changed to prescription opioids at the first refill (36). Corresponding data for other prescription medications included 5122 patients (34.7% of between-class switchers; 23.3% of those without consecutive triptan refills) switching to NSAIDs; 1051 (7.1%; 4.8%) changing to barbiturates; and 1450 (9.8%; 6.6%) switching to other prescription non-migraine-specific therapies (36). Our study may have underestimated overall opioid use because it evaluated only refill frequencies for prescription, not potential OTC, opioids.
On the other hand, two major factors limit the degree to which actual health-seeking behaviours of our cohort can be compared with those of the US study (36): (i) the limited patient-level data inherent in our retrospective cohort study of electronic medical records; and (ii) potential transatlantic disparities in healthcare systems, including potential differences in co-pay costs, medication tiering, and other financial issues related to medication access. Future studies are needed to determine reasons why European patients do not refill their initial triptan prescriptions. Ideally, some of these studies should be conducted at the national level, because there may be country-specific differences in patient (and care-giver) attitudes, beliefs and expectations concerning the management of migraine with triptans and other medications.
Potential study limitations
Perhaps most importantly, our study population comprised a subset of all migraineurs: individuals with migraine treated by primary care physicians with whom they had established clinical relationships in the UK, France and Germany. Despite considerable disability and reduced quality of life, most British and Western European patients with migraine either do not consult with physicians, do not receive a correct diagnosis of migraine, are inadequately treated, self-treat their condition, and/or do not use prophylactic medications (37–42). Given that many of our patients could have purchased widely accessible OTC triptans rather than fill and refill triptan prescriptions at the time of the study, or could have switched from prescription to OTC triptans, our analysis may have overestimated the problem of low triptan prescription refill frequency in these countries.
In fact, triptans were first approved (naratriptan [Formigran; GlaxoSmithKline (GSK)] 2.5 mg) for OTC use in Germany in 2006, and then, for behind-the-counter (BTC) dispensing by pharmacists in the UK (June 2006, as sumatriptan [Imigran Recovery] 50 mg; GSK]), as our study was being conducted (2006−2008). Particularly in patients with less severe (but still considerable) disease burden, these widely available agents can help to limit unnecessary office visits and repetitive prescriptions from physicians, and also can assist in filling potential gaps in prescription medications (although patients should be instructed not to take more than 10 triptan tablets in a month, in order to prevent iatrogenic increases in attack frequency) (43). In Germany, OTC triptan (naratriptan) sales in 2008 were approximately €2 million and, in the UK in 2010, total BTC triptan sales were approximately £5 million (44,45). By one estimate, only 15% of British patients with migraine received triptan prescriptions around the time of our study (43). More than 4 million OTC naratriptan tablets (approximate current cost = €5 − 10 per 2 tablets) were dispensed from 2006 to 2010, without any reported safety or tolerability issues (46). Potential low-cost OTC triptan options are also widely available via the Internet.
Use of OTC triptans has now been introduced into German national headache treatment guidelines; rather than prescribing triptans, many German physicians are proactively requesting that patients use these OTC agents (46). On the other hand, use of non-prescription triptans (including also Migraleve Ultra [Pfizer]) in the UK has been more limited, in part because pharmacists are required to complete a specific patient adequacy questionnaire before dispensing BTC triptans.
Taken together, these facts concerning the triptan treatment milieu during our study might help to explain why higher proportions of German (54.7%) than British (48.5%) patients in our study never received further triptan prescriptions for migraine after their index prescriptions (and also had lower frequencies of refills 2−6+; Figure 3); higher proportions of the German patients may have been meeting their therapeutic needs via OTC (vs. prescription) triptan use. It might be of interest in the future to conduct a naturalistic observational study of triptan prescription fill and refill frequencies after (vs. before) a patent expiration.
Our retrospective analysis also involved patients’ electronic medical records (continuous prescriptions written) rather than their pharmacy claims or actual medication-taking behaviours. According to study protocol, patients who switched from triptans to opioids and then back to triptans were considered to be triptan-persistent. We also did not impose any minimum duration of adherence or gap in medication prescribing to define persistency.
Another limitation of the present study is that it assessed only the use of oral triptans, not nasal sprays (NS), subcutaneous (SC) injections, or other, non-oral formulations. Consequently, our study may have underestimated the degree of within-class triptan switches compared to real-world settings. Our study also did not account for potential switches from prescription to OTC triptans or from prescription to OTC analgesics with or without subsequent refills.
As mentioned previously, the degree of patient-level data in our study, including patients’ reasons for filling or discontinuing triptan prescriptions over time, was limited. This issue and others are being addressed in an ongoing observational study. In theory, other plausible explanations of our findings of reduced triptan persistency also include potentially incorrect migraine diagnosis (47).
Other viable explanations of our findings of reduced triptan fills and refills include the prospects that: (i) patients may have had relatively low frequencies of migraines, which did not require additional triptan prescriptions and refills; or (ii) the prescribed doses may have been inadequate to abort triptan attacks, with worse outcomes resulting in switches to non-triptans. It is also possible that reduced triptan prescription fills and refills represented improved migraine outcomes, with reduced attack frequency, duration or severity after effective abortive treatment.
Given the ‘gatekeeper’ role of primary care physicians in the UK, it is feasible that British patients received (and refilled) their triptan prescriptions from specialists upon referral. On the other hand, French and German patients may have been more likely to receive initial triptan prescriptions from office-based specialists rather than primary care physicians. The possibility that patients with more severe migraine consulted with specialists rather than primary care physicians may have introduced selection bias toward a cohort with overall milder disease than might otherwise have been expected. Patients with milder disease may have had relatively infrequent (and less severe or disabling) attacks and hence also experienced reduced requirements for triptan fills and refills compared to those with more severe disease.
The relatively advanced age of our cohort – migraine prevalence peaks at approximately 25−39 years in Europe (9) – increases the likelihood of comorbid conditions (47), which can complicate migraine diagnosis and treatment (or even contraindicate it). These factors could also help to explain reduced fills and refills of triptan prescriptions. However, we infer that a clinical electronic record of a triptan prescription is a reasonable surrogate for the presence of migraine, because triptans are considered to be a sound treatment option for patients with moderate-to-severe disease (23) and, to our knowledge, there are no off-label uses of these medications.
By definition in our study protocol, patients with migraine diagnosed within 1 year were not eligible; thus, most patients were probably receiving triptan prescriptions for newly diagnosed migraines. By recently receiving a diagnosis and disease-specific treatment, such patients might be expected to have been ‘sensitized’ to their susceptibilities to migraines (and to anti-migraine drug efficacy). This possibility, together with our finding that triptan prescription refill frequencies declined sharply over time, suggests that, overall, patients with newly diagnosed migraine might be expected to be more persistent with therapy compared to those with longer intervals since migraine diagnosis.
To generate a more homogeneous patient population, we excluded individuals whose index triptan prescriptions were accompanied by other migraine medications. Because a higher degree of such ‘rescue’ and other forms of migraine co-medication might be expected in patients with more severe migraine, this criterion may have biased our patient sample towards a less severely ill or disabled population. Prescription triptan fill and refill frequencies might have been higher if patients receiving migraine prophylaxis had been included. On the other hand, triptans are considered to be sound initial treatments for patients with moderate-to-severe migraine (23), and, according to our study design, any triptan refill during the 2-year follow-up period was captured. We are therefore confident that the observed triptan persistency or non-persistency patterns were adequately quantified and characterized in our study.
Finally, our study involved different physician practices within distinct healthcare systems across three European countries; such methodological heterogeneity is inevitable in a study of this nature but must be recognized as a potential impediment to generalizing our findings to wider patient segments and healthcare settings. The IMSDA database was designed to be representative of the many types of possible practice settings in each country. The extent to which our database was representative of all patients seen by primary care physicians in each country was largely dependent on each country’s healthcare system and a patient’s interactions with it.
These caveats notwithstanding, our data raise some important research questions concerning patients’ (and/or their physicians’) reasons for refilling, discontinuing or switching prescription migraine regimens over time and potential baseline or on-treatment predictors of these decisions. A prospective observational study in the USA has been conducted to better understand reasons for triptan usage and discontinuation among newly prescribed triptan users.
Conclusions
Our study findings suggest potential clinical challenges in the management of acute migraine by primary care physicians in Europe who are concerned about optimizing patients’ experiences with prescription triptans. The findings are largely consistent with those reported previously in the USA. Most patients starting triptan therapy in the UK, France and Germany did not persist with this treatment beyond the initial prescription fill. Many patients discontinued all prescription therapies, while smaller proportions switched to alternative (non-index) triptans or other classes of medications. Most regimen alterations, including discontinuations, occurred at the estimated time of the first refill. However, many migraine sufferers probably did not seek physician care for their migraines, and others might have used available non-prescription (e.g. OTC, BTC) forms of triptans. Our findings are most generalizable to relatively older patients with moderate-to-severe migraine. A prospective, longitudinal study, including more detailed patient data, has been performed to better understand reasons for filling/refilling or discontinuing prescription migraine therapies.
Footnotes
Funding
This study and the present communication were supported by Merck & Co., Inc. (Whitehouse Station, NJ, USA).
Acknowledgements
Assistance in research and manuscript preparation was provided by Stephen W. Gutkin, Rete Biomedical Communications Corp. (Wyckoff, NJ, USA), with support from Merck & Co., Inc.
Conflict of interest
When this study was conducted and the manuscript prepared, Drs Ng-Mak and Ho were employees of, and minor shareholders in, Merck & Co., Inc. Dr Ng-Mak is now an employee of, and minor shareholder in, Allergan, Inc.; while Dr Ho is an employee of, and minor shareholder in, AstraZeneca. Dr Chen is an employee of, and minor shareholder in, Merck & Co., Inc. Drs Stanford and Roset are employees of IMS Health, a paid consultancy to Merck & Co., Inc.