
Abstract
Objectives: Apart from the characteristic chronic head pain in a coin-shaped circumscribed area, superimposed exacerbations have been described from early reports of nummular headache (NH). In a prospective series, we aim to compare the demographic and clinical characteristics between cases of exacerbations (ENH) and non-exacerbations (NENH) in NH.
Methods and results: Seventy-two NH patients (44 female, 28 male) attending a headache outpatient office. As eight patients presented with bifocal NH we analysed 80 painful areas; 47 (58.8%) presented in situ exacerbations. Mean intensity of exacerbations was 7.5 ± 1.6 and they lasted 5.7 ± 11.6 minutes. Exacerbation quality was mostly stabbing. We found no differences between ENH and NEHN groups in age at onset, baseline pain intensity, size of painful area, allodynia or other sensory symptoms, or baseline pain quality. There were no differences between populations with respect to relief with symptomatic therapy, requirement of preventative therapy and its response to preventatives.
Conclusion: In situ exacerbations superimposed on baseline pain are frequent in NH and might be included in diagnostic criteria. No statistically significant differences were found between ENH and NENH cases in demographic and nosological characteristics, or needing or response to therapy, but these sample sizes are small.
Objectives
Proposed diagnostic criteria for nummular headache (ICDH-II, International Classification of Headache Disorders, 2nd edition).

Apart from the mild-to-moderate intensity baseline pain, many patients usually experience superimposed exacerbations, lasting from several seconds to hours. Although exacerbations are mentioned in diagnostic criteria and some series of patients, we hereby firstly analyse comparative characteristics between exacerbations (ENH) and non-exacerbations (NENH) nummular headache cases.
Methods
We prospectively evaluated consecutive new patients with NH diagnosed accordingly to ICHD-II research criteria, attending a headache outpatient office located in a tertiary hospital from January 2008 to October 2011. Seventy-two patients (44 female, 28 male) out of 1560 (4.6%) attending were diagnosed with NH. As eight patients presented with bifocal NH we analysed the clinical characteristics of 80 painful areas.
We obtained a complete history for each patient, including precipitant events or coexistence of other types of headache. We considered age at onset and sex, and evaluated characteristics of baseline pain (quality, intensity, temporal pattern, location, size, shape) and exacerbations (quality, intensity and duration). Regarding temporal pattern, we considered chronic NH when there were no significant remission periods, episodic NH when remission periods longer than 3 months were noticed, and recent when time from onset was less than 12 months. The presence of triggers of exacerbations was also considered. Subsequently, we performed a complete physical and neurological examination including inspection, palpation and sensory examination of the painful area. We considered in each patient relief provided with symptomatic treatment and requirement and efficacy of preventative therapies. Neuroimaging study (magnetic resonance or computerized tomography of the head when first was not possible) and routine blood work-up, always including erythrocyte sedimentation rate and antinuclear antibodies, were carried out, with no abnormalities in all cases.
We finally compared demographic, clinical and therapeutic characteristics between ENH and NENH groups using conveniently unpaired t-test and chi-square test. Statistical analysis was performed with SPSS 15.0 software. Significance level was established at 0.05 (two-tailed).
Our first 30 NH cases (3), including four bifocal (4), have already been published.
Results
Mean age at onset of NH in 72 patients was 47.3 ± 18.5 years (range 12–82). As eight patients presented with bifocal NH we analysed 80 painful areas. Temporal pattern was chronic in 30 areas (37.6%), episodic in 31 (38.7%) and recent in 19 (23.7%). Forty-two (52.5%) were right-sided, 32 (40%) left-sided, and six (7.5%) sagittal. Most frequent locations were occipital (26.3%), parietal (23.8%) and frontal (18.8%). The shape of the painful area was mainly rounded (80%). Qualities of baseline pain were mostly pressing (33.8%), stabbing (31.3%) or burning (23.8%). Intensity (0–10 on a visual analogical scale (VAS)) was 5.7 ± 2.6 (range 1–9). In 35 areas (43.8%) numbness was spontaneously disclosed by the patients, associating paraesthesia in 16 (20%). Tenderness to palpation was found in 29 areas (36.3%).
There were in situ exacerbations in 47 areas (58.8%). Intensity of exacerbations was 7.5 ± 1.6 (range 4–10) and they lasted 5.7 ± 11.6 minutes. Exacerbation quality was mostly stabbing (59.6%). In three patients in our series, exacerbations were triggered by head movements and in one of them also by coughing or sneezing.
Among the 72 patients, 20 (27.7%) did not respond to analgesics (defined as less than 50% pain relief), and in 42 (58.3%) a preventative was required, achieving at least 50% pain relief in 34 (80.9%) patients. The most widely used drug was gabapentin (37 patients, 51.4%) titrated between 800 and 1800 mg/day. In six patients gabapentin was not helpful and lamotrigine dosed between 100 and 200 mg/day was used instead.
Main features of exacerbation and non-exacerbation groups.

ENH: exacerbations nummular headache; NENH: non-exacerbations nummular headache; SD: standard deviation; F/M: female/male; Ch/Epis/Rec: chronic/episodic/recent; VAS: visual analogue scale (0: no pain, 10: the worst imaginable pain); Occ/Par/Fr: occipital/parietal/frontal; R/E: rounded/elliptical.
When considering patients instead of painful areas n is respectively 43 and 29.
In response to preventatives N is 26 and 16, respectively.
t-test; 2chi-squared test.
Discussion
Since the first description of nummular headache (1), more than 200 cases have been described worldwide (3). As we show in this series, NH is not an uncommon diagnosis in an outpatient headache office. In one hospital series, its incidence was 6.4/100,000/year (5) and in a study in a general neurology outpatient office it represented 1.25% of all patients attending due to a headache (6). Originally, NH was described as a persistent, dull, mild to moderate head pain, felt exclusively in a circumscribed round or elliptical-shaped area typically 2–6 cm in diameter (1,5,7,8).
NH has a female predominance and mean age of onset is around 40 years, as we have observed in our patients. Pain is usually located in the parietal scalp, although in our series there is a slight occipital predominance (7).
Although not included in diagnostic ICHD-II criteria, superimposed exacerbations have been described from early reports of NH. They may last for several seconds or gradually increase up to hours (1,5). Exacerbations are noticed as being more intense than basal pain, and mainly with a throbbing, electric or stabbing quality; in our series most of them were stabbing. They may be precipitated by touching the symptomatic area (5,8–12) and, as we have observed in our series, by head movements or Valsalva manoeuvres. The existence of pain attacks with no baseline pain (9,13) has also been described; nevertheless, we think that differentiation with primary stabbing headache is particularly difficult in such cases (5).
Demographic and clinical features of NH cases including exacerbations in larger published series.
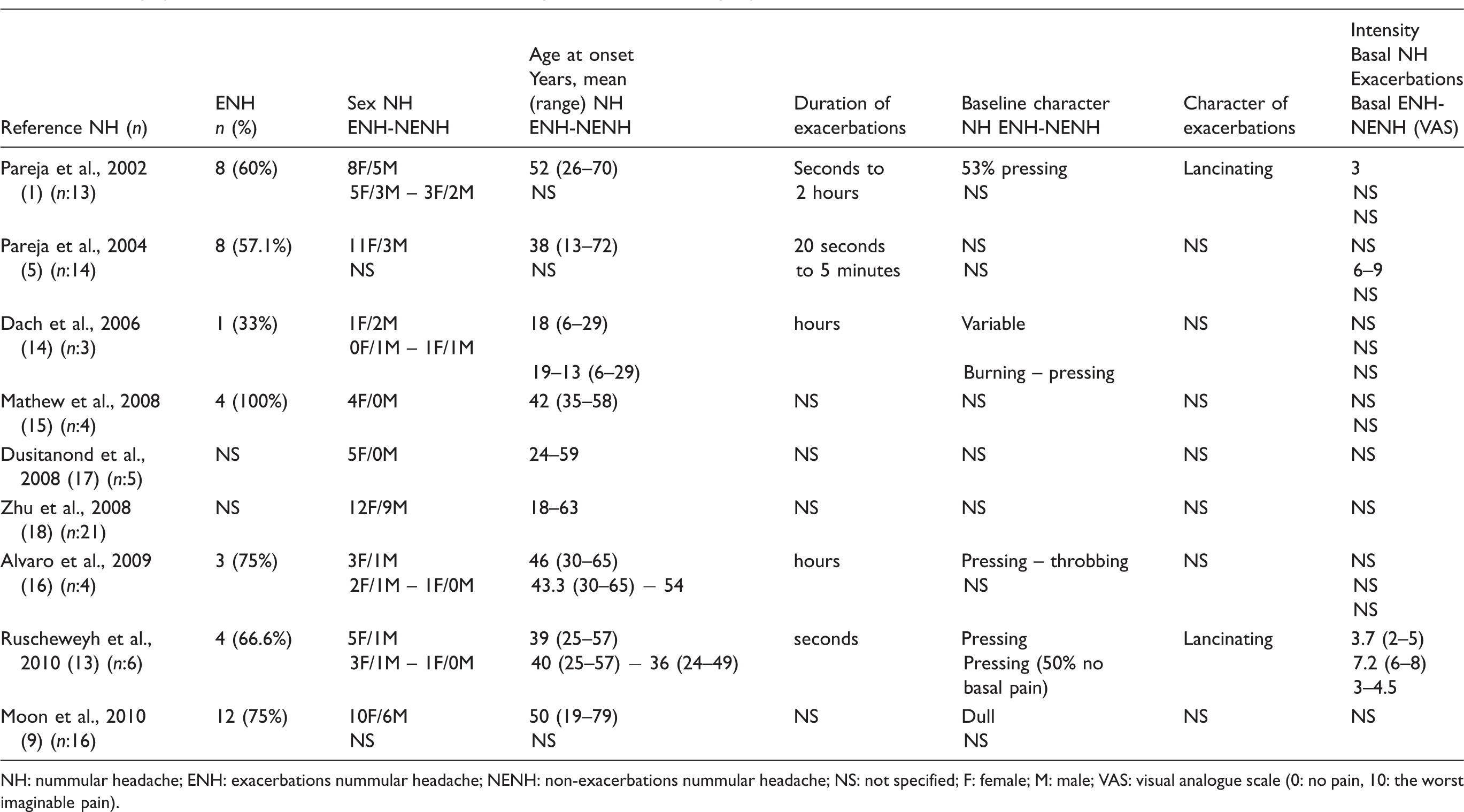
NH: nummular headache; ENH: exacerbations nummular headache; NENH: non-exacerbations nummular headache; NS: not specified; F: female; M: male; VAS: visual analogue scale (0: no pain, 10: the worst imaginable pain).
The exact aetiology of NH is not clear, although it appears to be a local pain disorder with sensitization restricted to the symptomatic area, probably stemming from epicranial tissues, such as the terminal branches of sensory nerves (9,13,19–22). In the same way as neuropathies of peripheral nerves, in NH there is a variable combination of either continuous or paroxysmal spontaneous pain, stimulus-evoked pain, trophic changes (23) and sensory signs. Pain paroxysms may be consistent with the terminal branch neuropathy hypothesis of NH (13).
Regarding treatment, our first series affirmed that treatment was generally not necessary and it was enough for patients to be informed about the benign nature of their pain; when needed, standard doses of paracetamol usually sufficed (1,5). However, patients with NH often have an inadequate response not only to analgesics, but also to non-steroidal anti-inflammatory drugs (NSAIDs), opiates, oral steroids, or local infiltration with anaesthetics (7,14,15,24). Such patients should be assessed for the use of preventative therapy, considered necessary in 58% of our cases. There are no clear guidelines, as all we know about the management of these patients is based on small series or isolated cases. Gabapentin has been the most prescribed drug and has been suggested to be partially or completely effective in some case reports (7,14,19), although results are inconsistent (8–10,16,17,25). Botulinum toxin type A (BoNTA) has been used in a small number of patients with encouraging results, and appears to be effective in NH with inadequate response to other therapies (15,17). It has been recently supported with a Grade C recommendation (26). Other preventatives such as tricyclic antidepressants (15,24,25), topiramate (9,13), carbamazepine (9), indomethacin (8) or neurotropin (27) have been helpful in some patients.
In our series more than 80% of patients achieved at last partial response with preventatives. We commonly used gabapentin at a dose of 600–2400 mg daily; BoNTA was not attempted on any of our patients. In our patients the presence of exacerbations was not related to relief with symptomatic therapy, or needing or response to preventatives.
In conclusion, in situ exacerbations are common in NH, a not infrequent diagnosis in a headache outpatient office. The presence and characteristics of exacerbations might be included in future diagnostic criteria. According to our comparative analysis of exacerbations and non-exacerbations cases in the larger series of NH published up to now, there are no demographic or clinical differences, including needing or response to therapy, between both populations. Nevertheless, sample size was probably still too small to show statistically significant differences.
Footnotes
*
Partially presented as a poster at the 2nd European Headache and Migraine Trust International Congress, Nice, October 2010.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.