
Abstract
Ten patients (one man and nine women, mean age 48.8 ± 20.1) presented with a stereotypical and undescribed type of head pain. They complained of strictly unilateral, shooting pain paroxysms starting in a focal area of the posterior parietal or temporal region and rapidly spreading forward to the ipsilateral eye (n = 7) or nose (n = 3) along a lineal or zigzag trajectory, the complete sequence lasting 1-10 s. Two patients had ipsilateral lacrimation, and one had rhinorrhoea at the end of the attacks. The attacks could be either spontaneous or triggered by touch on the stemming area (n = 2), which could otherwise remain tender or slightly painful between the paroxysms (n = 5). The frequency ranged from two attacks per month to countless attacks per day, and the temporal pattern was either remitting (n = 5) or chronic (n = 5). This clinical picture might be a variant of an established headache or represent a novel syndrome.
Keywords
Introduction
Head pain may have an intracranial or extracranial origin. We have previously proposed the term epicrania to group all headache syndromes that apparently stem from superficial or extracranial structures, including the scalp and all the layers of the skull (1). Epicranias would comprise both epicranial headaches, e.g. nummular headache (NH), and epicranial neuralgias, e.g. supraorbital and occipital neuralgias. Superficial head pain may be continuous or brief, and either localized in a small area or within the territory of a pericranial nerve. In addition, there may be symptoms and signs of sensory dysfunction in the symptomatic zone, or tenderness over the emergence or the course of a pericranial nerve. Otherwise, epicranial pain tends to be confined within a restricted area, and so far substantial spread or march to other regions has not been reported.
Our aim was to report an undescribed type of headache, apparently originating in the scalp, but with particular traits that deviate from all known headaches and neuralgias. Ten patients presented with a paroxysmal head pain starting in a focal area of the posterior parietal or temporal region and rapidly spreading forward to the ipsilateral eye or nose along a linear or zigzag trajectory, the complete sequence lasting one to a few seconds. The features are so consistent and distinctive that we are probably facing a novel syndrome, which we have named epicrania fugax (EF).
Patients and methods
Through a 2-year period we identified 10 patients with stereotypical head pain. All of them complained of shooting painful paroxysms starting at a particular point of the scalp and quickly radiating forward to the ipsilateral eye or nose. A detailed history was obtained in all cases. A complete physical and neurological examination was also performed. This always included inspection, palpation and sensory examination of the stemming area, as well as palpation of the supraorbital, infraorbital, supratrochlear, infratrochlear, minor occipital and greater occipital nerves. X-ray of the skull, computed tomography or magnetic resonance imaging of the head, and routine blood work-up with erythrocyte sedimentation rate and immunological screening were carried out in all cases in order to exclude any underlying disease.
Pharmacological treatment was prescribed in only two patients: one of them received indomethacin (75 mg/day), and the other took carbamazepine (600 mg/day). Another patient underwent anaesthetic blockades with 0.25% bupivacaine at three points of the symptomatic side: first, the supraorbital nerve (SON); second, the greater occipital nerve (GON); and third, the stemming area.
Results
Among the 10 reported patients, one was male and nine female (see Table 1). They were aged 24–78 years (mean 48.8 ± 20.1 years), and the age at onset of the pain paroxysms ranged from 23 to 70 (mean 45.8 ± 18.7 years). Two patients had a history of migraine, and one patient had tension-type headache. However, there was no temporal connection with these headaches, and the new pain was described as different from any previously experienced pain. Apart from that, past medical history was always unremarkable, and the onset of head pain could never be related to any particular event.
Demographic and clinical features of patients with epicrania fugax

Visual Analogical Scale (0 = no pain; 10 = the worst pain imaginable).
Touch could be a precipitating mechanism when applied to the site of origin of the pain.
Between paroxysms mild pain or other sensory disturbances could be present at the stemming area (i.e. the site of origin of the pain).
The clinical features are shown in Table 1. Pain paroxysms were strictly unilateral and usually recurred on the same side of the head. Seven patients had symptoms on the right and one patient on the left, while the attacks shifted sides in only two patients. Pain always started in a focal area of the posterior parietal or posterior temporal region, which remained the same for all the attacks in each patient. With each attack an electric or stabbing pain stemmed from that particular point and rapidly spread forward to the ipsilateral eye (n = 7), or even the nose (n = 3), along a linear or zigzag trajectory (Fig. 1). The complete sequence could last up to 10 s, but typically lasted 1–3 s. Once the pain reached the eye, two cases had ipsilateral lacrimation without conjunctival injection. One of the patients with pain reaching the nose had rhinorrhoea at the end of the attacks (Fig. 2). The paroxysms were usually spontaneous, but two patients had attacks triggered by touch on the stemming point. Between attacks five patients had no symptoms at all, whereas the other five had mild pain or tenderness in the stemming area. The frequency of attacks was variable, ranging from two attacks per month to ‘countless’ attacks per day. The temporal pattern was chronic in five patients, who had been having attacks for 1–10 years without a break. The remaining five patients had a remission after a symptomatic period of 2 weeks to 1 year, and none of them has relapsed to date.

Trajectory of pain paroxysms in epicrania fugax. Pain always stems from a particular cranial area and reaches the ipsilateral eye or the ipsilateral nose.

Eczema due to numerous attacks with rhinorrhoea in patient 5.
Upon examination, neither skin changes nor sensory loss were noted in the painful zones, but there was hyperaesthesia to pinprick and light touch in the trigger area of patient 1. Palpation of the supraorbital, infraorbital, supratrochlear, infratrochlear, minor occipital and greater occipital nerves did not evoke any abnormal sensation, and neurological examination was otherwise normal. Blood tests and imaging studies were also normal in all cases.
While patient 1 was having a bout of pain paroxysms, anaesthesia of the SON inhibited the radiation, but the trigger zone remained tender. In contrast, blocking of either the GON or the trigger zone in the same patient abolished all the symptoms. Patient 6 took indomethacin (75 mg/day) for 3 months and did not find any relief. On the other hand, patient 8, who had the most frequent attacks, got a complete response with carbamazepine (600 mg/day).
Discussion
Here we present 10 patients with a previously undescribed head pain that shows consistent features both intra- and interindividually. This clear-cut set of symptoms apparently constitutes a new headache, and we have named it EF. The clinical picture is a combination of two components: dynamic, i.e. spontaneous or triggered paroxysmal pain that suddenly starts in a posterior cranial area and rapidly spreads forward to the ipsilateral eye or nose; and static, i.e. the fixed source of the shooting pain, which may be just a trigger zone or remain slightly painful between the paroxysms. This superficial and monodirectional pain probably originates in a terminal branch of a pericranial nerve. However, the precise nature of EF is unknown. It might be regarded as a variant of other headaches, or might represent a new syndrome.
There are obvious similarities between EF and primary stabbing headache (PSH). Both disorders are characterized by ultrashort paroxysms of head pain. Unlike EF, PSH paroxysms tend to be multilocalized, but the stabs may be strictly confined to one area in a minority of patients (2–4). PSH is hardly ever provoked and has no interictal symptoms. Nevertheless, the jabs occasionally emerge on top of a unilateral headache with local allodynia (5). In PSH the vast majority of stabs are singlets starting and ending at the same point (6). However, it may rarely manifest in volleys (4, 6), and consecutive stabs may sporadically move through a long distance. Theoretically, a series of stabs could follow the trajectory of EF, although a spread from the posterior cranium to the eye or nose has never been described. Despite all these considerations, the clinical picture of EF is not typical for PSH for a number of reasons (Table 2). PSH is typically characterized by multifocal and motionless stabs. In contrast, all the patients in this series showed a focal and fixed source, motion, and a characteristic trajectory of their head pain, and these consistent features are probably linked by a specific pathogenic mechanism. Moreover, carbamazepine, but not indomethacin, had a therapeutic effect in EF. Although this observation is based on only two patients, it does not support the presence of PSH. EF might be a rare variant of PSH and thus enlarge the clinical spectrum of headache stabs. However, EF and PSH are more likely to be independent disorders.
Differences between primary stabbing headache and epicrania fugax

Sjaastad et al. 2002: The Vågå study (4).
Current series.
There are also some similarities between EF and NH. EF resembles NH in the presence of a focal painful area. Nevertheless, NH remains circumscribed in a small cranial area, and pain overshooting such a fixed area has never been observed (2, 7–9). In addition, NH is typically continuous, although there may be occasional exacerbations. Superimposed paroxysms do exist in NH, but they always conclude in situ (9).
Epicrania fugax may also remind us of occipital or supraorbital neuralgias, but there are important differences. Occipital neuralgia is characterized by paroxysmal pain in the distribution of the greater occipital, minor occipital or third occipital nerve that is relieved by anaesthesia of the affected nerve (2, 10). Blocking of the GON provided absolute relief in one of our patients. However, the effect of anaesthesia was not assessed in the others, and none of the patients with EF felt pain or tenderness in the territory supplied by the occipital nerves. Moreover, the beneficial effect of GON blockade is actually a non-specific phenomenon common to many headaches, including migraine and cluster headache (11–13). Supraorbital neuralgia produces pain in the forehead, and is associated with tenderness at the supraorbital notch, on the emergence of the SON (14, 15). Otherwise pain in supraorbital neuralgia is usually continuous, and is relieved by local anaesthesia of the SON. Our patients with EF had pain in the area supplied by the SON, but it always stemmed from a posterior cranial area, just at the borderline between the territories of the GON and the SON. Besides, EF pain was not persistent but paroxysmal, and was not associated with tenderness of the SON. The SON was blocked in a single patient, and this caused transient anaesthesia in the frontal region. Conversely, the trigger area in the parietal region remained tender, although unable to radiate the pain towards the eye.
Epicrania fugax could be a variant of first division (V1) trigeminal neuralgia, since the paroxysms of pain are felt in the territory of V1 (2, 16). Besides, one of the patients with EF was treated with carbamazepine with complete success. However, EF differs clearly from genuine V1 trigeminal neuralgia as regards to several clinical variables, such as the usual age of onset, the site and nature of precipitating agents, and the duration, intensity and frequency of attacks (16, 17) (Table 3). The two syndromes also differ regarding the localization of the pain: in our published series of V1 trigeminal neuralgia (16, 17) the pain was usually felt in the orbit or forehead and hardly ever reached the hairy scalp. Furthermore, the suffering of patients with trigeminal neuralgia is much greater than that reported by the patients with EF. In fact, only one of our EF patients required drug therapy. All in all, these differences seem sufficient to discriminate between EF and genuine trigeminal neuralgia.
Differences between V1-neuralgia and epicrania fugax
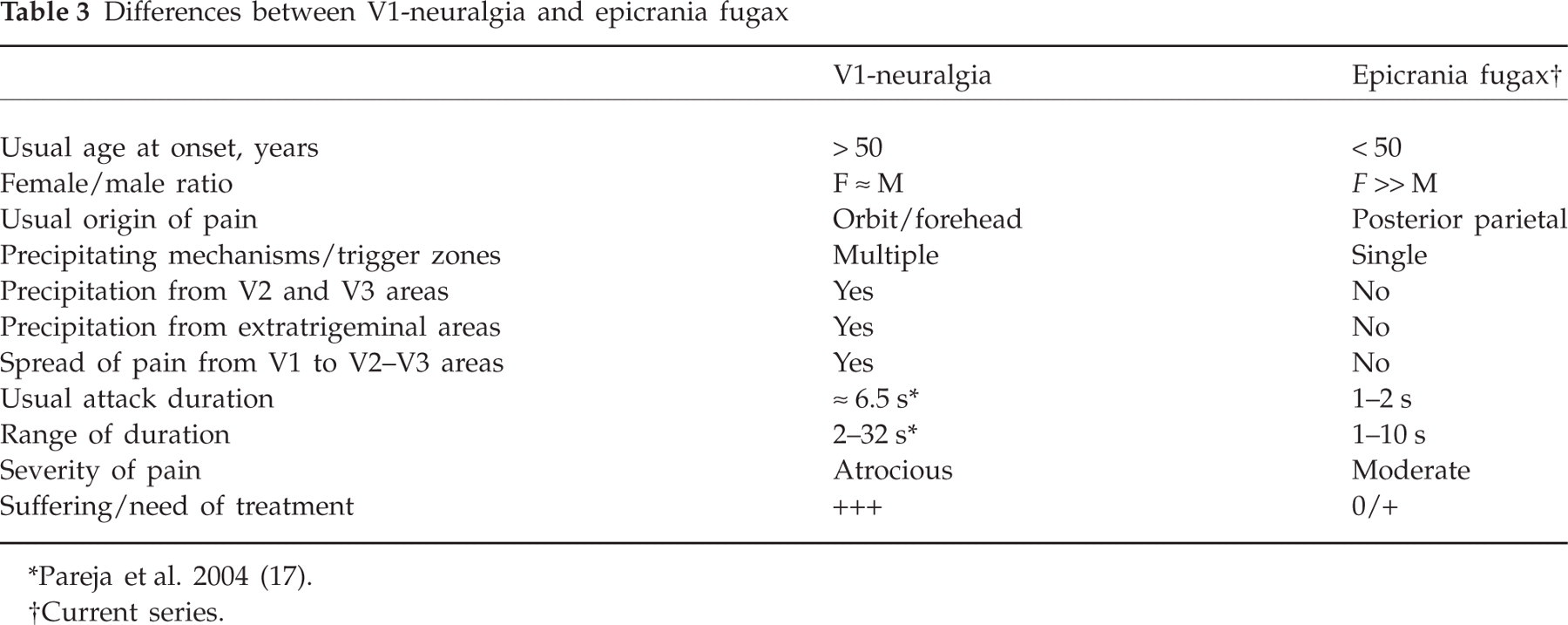
Pareja et al. 2004 (17).
Current series.
The presence of autonomic accompaniments in three patients may pose some difficulties in the differentiation of EF from shortlasting, unilateral, neuralgiform headache attacks with conjunctival injection and tearing (SUNCT). In contrast to SUNCT, EF seems to be a female-predominant disorder, with pain attacks usually lacking accompaniments. On the other hand, EF attacks last up to a few seconds, whereas only a minority of SUNCT attacks last < 10 s (18). What is more, no conjunctival injection at all was observed in those three patients with lacrimation or rhinorrhoea, and that is a characteristic symptom in patients with SUNCT (2, 19, 20). The discrimination between EF and shortlasting, unilateral, neuralgiform headache attacks with cranial autonomic features (SUNA) is not so straightforward. Unlike SUNCT, SUNA can be diagnosed with the presence of just one cranial autonomic feature and the attacks have a wider range of duration (2, 20). Consequently, the minority of EF patients that displayed lacrimation or rhinorrhoea could meet criteria for SUNA. However, overlap concerning a particular feature is a common situation among different headaches. Otherwise, the attacks of the three such patients were identical to those of the remaining patients and, admittedly, they could be grouped in the same category.
The pathogenesis of EF is uncertain. The existence of a stemming or trigger zone in a focal area, the electric or stabbing character, and the narrow pattern of radiation are features that suggest a peripheral origin of this sort of pain. The discharges might originate in a terminal twig of the SON and eventually extend to other fibres of the nerve trunk. The apposition of distinct axons might favour the transfer of nerve impulses from one set of fibres to another, either by ephaptic (electric) transmission or by paracrine diffusion of chemical mediators (21). Alternatively, they might stem from terminal branches of the GON, and spread to the SON by cross-talk between fibres of both nerves. Indeed, pain in all our patients started at the edge of both territories, where the terminal sensitive fibres of the GON and SON can be interwoven (22, 23). Expansion of pain from one region to another could also be due to the confluence of separate afferences at the central nervous system (24). In fact, pain of neuropathies may sometimes extend outside the affected territories. Finally, we cannot exclude transdiploic transmission, which might explain the particular traits of EF. A rich innervation has indeed been recently found in the skulls of mice, with pain fibres that cross the bones and pain fibres that run longitudinally within the endosteum (25). In any case, the inputs generating EF would have to follow a central loop in order to recruit a trigeminofacial reflex in those patients presenting with autonomic features.
The fact that EF has been bilateral in two patients may be atypical, but is not a surprise. Other unilateral headaches and neuralgias may also come out on both sides of the head in some patients. For example, trigeminal autonomic cephalalgias, which are strictly unilateral, may display unilateral symptoms on either side in different attacks. Even in genuine neuralgias, which are conceptually unilateral, the process may duplicate on both sides. We have recently observed that the focal head pain of NH may also be present in two separate areas located on opposite sides in the same patient (26).
In conclusion, EF presents a clear-cut clinical picture that may be distinguished from other headaches and neuralgias. It is basically characterized by unilateral pain paroxysms that run back to front from a focal cranial area towards the eye or nose. EF might be a variant of other headaches, but might also represent a novel syndrome. At this stage, no definite explanation can be provided, but the clinical features point to a peripheral origin or trigger for this disorder.