
Abstract
Nummular headache (NH) has been defined as a focal head pain that is exclusively felt in a small area of the head surface. Here we describe three patients who presented with focal head pain in two separate areas. This finding seems to be consistent with bifocal NH and further enlarges the clinical diversity of this headache disorder. The pathogenic mechanisms of NH may be active in multiple cranial areas in some particular patients.
Introduction
Nummular headache (NH) was first defined as a primary headache disorder characterized by focal pain in a single round or elliptical area of the head surface, typically 2–6 cm in diameter (1, 2). The pain remained confined in such coin-shaped area, had mild-to-moderate intensity, and could be either continuous or intermittent. Furthermore, there could be a variable combination of sensory disturbances within the symptomatic area, including hypoaesthesia, paraesthesia, dysaesthesia and tenderness. However, since the first description of 13 patients in 2002, > 100 additional cases have been reported (3–27), some of which have shown different features, thus expanding the clinical spectrum of NH. Here we describe a new clinical feature in three patients, each presenting with focal head pain in two separate areas. This finding seems to be consistent with bifocal NH and further broadens the diversity of the clinical manifestations. This latest observation also suggests that the pathogenic mechanisms of NH may be active in multiple areas in some particular patients.
Case reports
Patient 1
A 28-year-old man presented with a 6-month history of focal and well-circumscribed head pain in the right parietal region, just over the right tuber parietale. The painful area was perfectly circular, measuring 5 cm in diameter (Fig. 1A). The pain was pressing and continuous, with mild-to-moderate intensity fluctuating around 3 out of 10. The affected area was hypersensitive, but there were no other associated features. Inspection and palpation of the scalp did not reveal any trophic changes. Hyperaesthesia, allodynia and trichodynia could be demonstrated within the painful area. Otherwise the neurological examination was normal. Blood tests, x-ray examination of the cranium and magnetic resonance imaging (MRI) of the brain were also normal. He did not take any symptomatic or preventive medications to alleviate the pain. During follow-up, the pain gradually decreased and finally disappeared 10 months after onset.
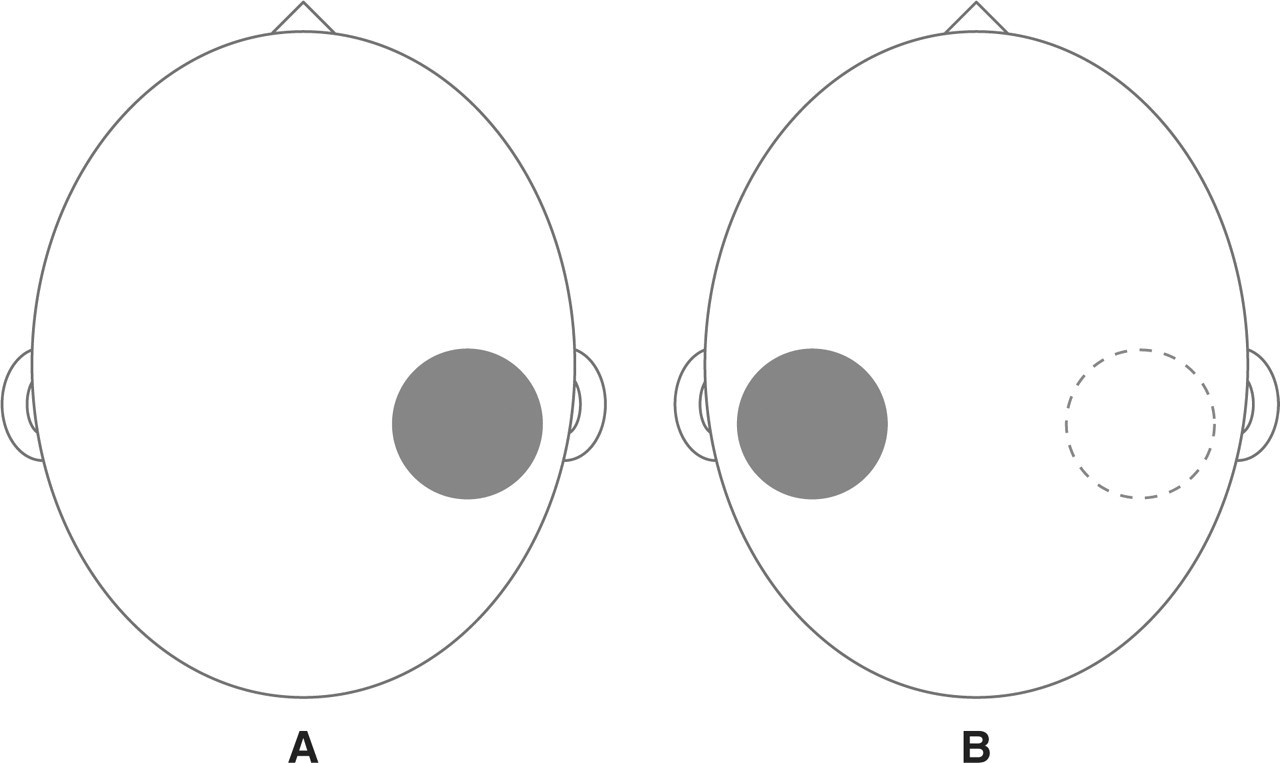
(A) Patient 1 had pain circumscribed to a circular area (5 × 5 cm) in the right parietal region for 10 months. (B) After 6 months' remission, pain emerged in a new rounded area (5 × 5 cm) over the contralateral parietal region.
After a 6-month remission period, a second focal head pain appeared in the left parietal region. The new painful area was roughly symmetrical to the former one, and was of similar shape and size (Fig. 1B). The pain was again pressing and continuous, and had an intensity of 3–4 on a 10-point scale. This time hyperaesthesia, allodynia and trichodynia were present in the new symptomatic area, but not in the previously affected area. In addition, pressure algometry demonstrated a lower pressure pain threshold in the new painful area (0.5 kg/cm2 in the left tuber parietale vs. 1.3 kg/cm2 in the right tuber parietale). The procedure was the same as that used in another study (28). In summary, an assessor blinded to the side of head pain performed three consecutive measurements on each marked point, and the mean value was taken as the pressure pain threshold. Pressure algometry was also applied over other cranial areas on both sides, and did not disclose any other significant asymmetries (left frontal 1.0 kg/cm2; right frontal 1.1 kg/cm2; left temporal 1.2 kg/cm2; right temporal 1.2 kg/cm2; left occipital 0.5 kg/cm2; right occipital 0.5 kg/cm2). The scores on the State Trait Anxiety Inventory (STAI) and the Beck Depression Inventory (BDI) were within normal ranges. This first case was discussed at the 59th Annual Meeting of the Spanish Neurological Society (21).
Patient 2
A 67-year-old woman started suffering from focal head pain in a circular area of 1.5 × 1.5 cm over the right frontal region (Fig. 2A). The pain was stabbing and continuous, with low-grade baseline intensity around 2 out of 10. Superimposed on the background pain, there were six to seven daily exacerbations with more intense pain (3–4 on a 10-point scale) lasting about 30 min. Neither trophic changes nor sensory abnormalities could be demonstrated in the symptomatic area, and no deficits were detected on neurological examination. Blood tests and cranial computed tomography were normal. A therapeutic trial with amitriptyline (10 mg/day) was not well tolerated and had no beneficial effect. Treatment with indomethacin (50 mg t.i.d.) provided partial relief.
(A) Patient 2 started having focal pain in a circular area (1.5 × 1.5 cm) at the right frontal region. (B) After 2 years with continuous pain, a new painful area (1.5 × 1.5 cm) appeared in the right occipital region.
Two years later, a second focal pain appeared in the right occipital region. This new pain was also felt in a round area of 1.5 × 1.5 cm (Fig. 2B). It was described as a pressing ache, with intensity around 3 out of 10 and no exacerbations. At the same time, the previous frontal pain persisted with its original features. Pressure algometry showed only slight differences between the pain thresholds on the symptomatic areas and the contralateral symmetrical points (right frontal 1.2 kg/cm2, vs. left frontal 1.3 kg/cm2; right occipital 2.0 kg/cm2, vs. left occipital 2.3 kg/cm2), but the pressure pain thresholds in other cranial regions were equal on both sides (right temporal 1.5 kg/cm2; left temporal 1.5 kg/cm2; right parietal 1.8 kg/cm2; left parietal 1.8 kg/cm2). Anxiety and depression tests (STAI and BDI) did not reveal any psychological disturbance.
Patient 3
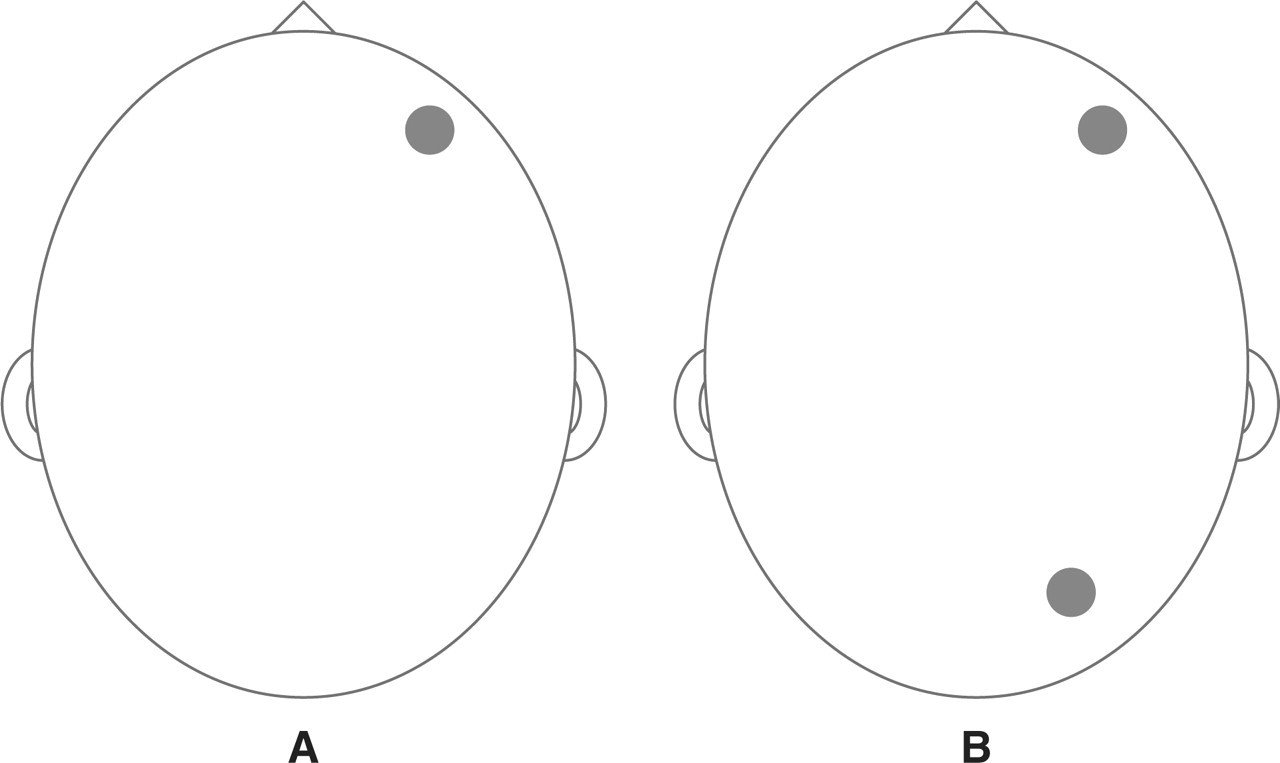
A 51-year-old man started feeling continuous pain in two circumscribed head areas simultaneously. The painful areas were located on each side of the head, in symmetrical temporal regions. Both were round and had a diameter of 2.5 cm (Fig. 3A). The pain had a pressing quality on both sides, but was more intense on the right (3–4/10) than on the left (1–2/10). The right area also showed cutaneous allodynia to touch stimuli. At this site there could be occasional exacerbations with severe pain reaching 9 out of 10. The exacerbations were either spontaneous or triggered by touch on the painful area and usually lasted just a few seconds. Other than hyperaesthesia on the right symptomatic area, there were no abnormalities in the physical examination. Ancillary studies including blood tests and MRI of the brain were normal. The pain was partially responsive to ibuprofen.

(A) Patient 3 presented with simultaneous pain in two symmetrical round areas (2.5 × 2.5 cm) at both temporal regions. The pain was more intense on the right. (B) After 2 weeks with continuous pain, the symptoms became intermittent in both affected areas.
Two weeks after onset, the pain became intermittent, with attacks lasting from 30 min to a few hours and occurring < 15 days per month (Fig. 3B). While the patient was pain free, pressure pain thresholds were measured at symmetrical points within both symptomatic areas. The measured values were lower in the right symptomatic area, which was the more severely affected (right temporal 1.0 kg/cm2, vs. left temporal 1.5 kg/cm2). In contrast, other cranial regions showed equivalent pain thresholds on both sides of the head (right frontal 1.6 kg/cm2; left frontal 1.6 kg/cm2; right parietal 2.3 kg/cm2; left parietal 2.3 kg/cm2; right occipital 2.5 kg/cm2; left occipital 2.5 kg/cm2). Psychological evaluation (STAI and BDI) found no evidence of anxiety or depression.
Discussion
Since the original description in 2002 (1), reports of multiple cases have increased our clinical knowledge on NH (3–27). For example, we now know that the pain may be severe (3, 5, 13, 14, 17, 20, 24, 25), although it is usually mild or moderate. In addition, some patients have shown trophic changes within the painful area (24). We have also learned that there can be two different temporal profiles, one chronic and one episodic (3, 5, 14, 20), with pain being either continuous or intermittent during the symptomatic periods. Furthermore, some headaches with a nummular pattern have been related to local lesions of the scalp (29), skull (22) or adjacent intracranial structures (18, 19). These might be considered secondary or symptomatic forms of NH. Altogether, these observations may eventually lead experts to revise current diagnostic criteria for NH. Here we have described a new clinical expression, with the presence of two distinct symptomatic areas in each of the reported patients. The combination of two painful areas may be regarded as bifocal NH, or else as co-existence of two NH in the same patient.
The spatial relationship between the two symptomatic areas was not equal in all our patients. Interestingly, two patients had pain over symmetrical points. Patient 1 felt the pain in both parietal convexities (the most common location for NH), and patient 3 had symptoms in both temporal regions. Moreover, the shape and size were identical on both sides in each of these cases. Some cases of bilateral NH have been described before, but their pain was located in a single midline area extending across both sides (3, 6, 7, 8, 13). Patient 2 also described two painful areas with a similar shape and size. However, they were placed in distant regions (frontal and occipital) of the same side of the head.
The temporal connection between the symptoms in each area was also heterogeneous. The sequence in patient 1 started on one side of the head and, after a pain-free period, emerged on the opposite side. In this migratory pattern the pain was present in one single area at a time. Patient 2 felt pain in one area at first and, after a long symptomatic period, started feeling pain in a second area as well. This was an additive pattern, with head pain in a single area evolving to head pain in two separate areas. Finally, patient 3 showed a synchronous pattern, since the pain appeared and vanished in unison in both symptomatic areas.
The pathogenesis of NH is uncertain. The confinement of pain and other sensory symptoms to a small cranial area apparently reflects a non-generalized and rather limited disorder. Moreover, pressure algometry has demonstrated a local increase of pain sensitivity just within the symptomatic area (28). On the other hand, NH patients do not show increased pericranial tenderness when compared with healthy subjects (30). All this evidence suggests that NH probably has a peripheral source. It has been proposed that NH may stem from any of the epicranial tissues, including the scalp and all the layers of the skull (3, 31). The present report of three patients with separate painful areas may pose a challenge to this theory. Alternatively, the existence of bifocal or multifocal NH may indicate that the local processes of NH can be reproduced in multiple cranial areas. In fact, these patients—especially patients 1 and 3—showed enhanced pain sensitivity within the symptomatic areas, which is still consistent with a local disorder. Perhaps some particular patients are liable to develop the pathogenic process of NH in different regions of the head.
In conclusion, NH may appear in two distinct areas in the same patient. The symptomatic areas may be located on one side or both sides of the head. The pain may emerge at the same time or follow a different course in each of the affected areas. The existence of bifocal or double NH further enlarges the clinical spectrum of NH. Moreover, this finding suggests that the pathogenic mechanisms of NH may be active in multiple areas in particular patients.