
Abstract
Background: The ‘headache attributed to airplane travel’, also named ‘airplane headache’ (AH), is a recently described headache disorder that appears exclusively in relation to airplane flights, in particular during the landing phase. Based on the stereotypical nature of the attacks in all reported cases, we proposed provisional diagnostic criteria for AH in a previously published paper. Up to now 37 cases have been described in the literature.
Methods: After our paper was disseminated via the Internet, we received several email messages from subjects around the world who had experienced such a peculiar headache. Their cooperation, by completing a structured questionnaire and allowing the direct observation of three subjects, enabled us to carry out a study on a total of 75 patients suffering from AH.
Results: Our survey confirmed the stereotypical nature of the attacks, in particular with regard to the short duration of the pain (lasting less than 30 minutes in up to 95% of the cases), the clear relationship with the landing phase, the unilateral pain, the male preponderance, and the absence of accompanying signs and/or symptoms. It is conceivable to consider barotrauma as one of the main mechanisms involved in the pathophysiology of AH. The observation that the pain appears inconstantly in the majority of cases, without any evident disorder affecting the paranasal sinuses, could be consistent with a multimodal pathogenesis underlying this condition, possibly resulting in the interaction between anatomic, environmental and temporary concurrent factors.
Conclusions: This is by far the largest AH case series ever reported in the literature. The diagnostic criteria that we previously proposed proved to be valid when applied to a large number of patients suffering from this condition. We support its recognition as a new form of headache, to be included in the forthcoming update of the International Headache Society Classification, within ‘10. Headache attributed to disorder of homoeostasis’. Its formal validation would favour further studies aimed at improving the understanding of its pathophysiology and implementing preventative measures.
Introduction
The ‘headache attributed to airplane travel’, also named ‘airplane headache’ (AH) is a recently described headache disorder that appears exclusively in relation to airplane flights, in particular during the landing phase. In 2007 we described the first Italian case of AH and proposed provisional diagnostic criteria, based on the stereochemical characteristics of the attacks (1), which were clearly outlined by case series described up to then (1–4). These preliminary criteria have been used to describe further cases in subsequent case reports (5–8). Moreover, after our paper was disseminated via the Internet, we received a number of email messages from people who had experienced headaches with the same features as those described in our article. These patients, when asked to provide detailed information about their attacks in order to better define the clinical characteristics of this headache, agreed to fill in a specific questionnaire. The preliminary results of our investigation were presented at the 15th International Headache Congress, held in Berlin in June 2011 (9).
Materials and methods
When replying to the subjects who sought our advice by email regarding their headaches, we attached the aforementioned structured questionnaire, aimed at obtaining all the relevant information that could clinically distinguish this peculiar disorder. Out of the 81 subjects suffering from AH, 78 had consulted us by email, whereas three presented in person to our centres. When clinically necessary, we further investigated other details of the headache, either by email or by telephone. The questionnaire was completed by 75 subjects.
Results
Age at onset
The initial observations (3) showing a male preponderance and an early age at onset of AH are confirmed in our current case series. In fact, the percentage of males was 61.3%. The patients’ mean age was found to be 36.5 ± 10.2 years (range: 8–62), with no significant gender difference. The mean ages on first flight and of headache onset were 17.7 ± 8.6 and 30.3 ± 9.9 years, respectively. In the majority of cases (88.0%) the onset of AH was not concomitant with the first flight.
Upper respiratory tract disorders
A positive history for allergy was reported by 32% of patients (13 males and 11 females); in particular two patients (a male and a female) suffered from bronchial asthma. A past history of sinus infections was found in 18.6% of cases (7 males and 7 females), whereas two male subjects had a recent episode of sinus infection. No patients had symptoms and/or signs related to inflammatory sinus disorders when they experienced the AH attacks. Almost a quarter of subjects (23%) were smokers, with no differences between males and females.
History of coexistent primary headaches
Concurrent primary headaches in ‘airplane headache’ patients (n = 41/75, 54.6%)

Clinical features of AH
The characteristics of AH appear to be quite peculiar.
Timing
Headache onset in respect to flight timing

First episode
The AH onset was concomitant with the first flight experience in nine patients, at the age of 20.3 ± 10.0 years, with their current mean age being 30.6 ± 12.3 years. In the remaining 66 cases, the first flight was experienced at the age of 17.3 ± 8.1 years, whereas AH onset occurred on average at the age of 31.7 ± 8.9 years (Table 2).
Duration
Clinical features of headache attributed to airplane travel (n = 75)

Intensity
The pain intensity was defined as severe by all the patients. More specifically, it was described as severe but tolerable in 11 cases, extremely severe in 29 and excruciating, unbearable in 35 (Table 3). On a mean visual severity scale (where 0 represents no pain at all and 10 represents pain as severe as possible) the mean score was measured as 8.8, with the score being more than 8 in 68 out of 75 cases (90.6%).
Quality of pain
Quality of the headache was most frequently defined as stabbing (44 cases, 59.5%). Other definitions were: pulsating in nine patients (12.1%), jabbing in eight (10.8%), pressing in seven (9.5%), electric shock in six (8.1%); in one case the quality was not specified (Table 3).
Emotional impact
Most patients (54, 72.0%) were concerned with the fear of suffering from a further attack and therefore were negatively predisposed for future flights. Among these subjects, 41 continued to fly with anxiety and/or worry; eight decided to fly only if strictly necessary, approaching the flight with anxiety; three gave up flying; and one avoided flights lasting for more than 2 hours.
Localization of headache
In the great majority of cases (64/74, 86.5%) the pain was strictly unilateral; one subject did not specify both the localization and the side of the pain, and a further subject reported the attacks to be unilateral, without describing their localization. In another 10 patients (13.5%) the headaches were bilateral or in the vertex. Out of the 64 patients with unilateral headaches, the pain constantly recurred on the same side throughout the different attacks in 52 cases (81.2%), while in seven cases (10.9%) the pain occurred on the opposite side in subsequent flights. The possible side shift of the pain was not assessable in five subjects who have suffered only from one unilateral attack up to now. The pain was more frequently localized to the fronto-orbital region (56/73, 76.7%), strictly side-locked unilateral in 44 cases (left n = 21; right n = 15; side not specified n = 8), unilateral with side shift in subsequent attacks in six cases and bilateral in six cases. In nine subjects (12.3%) the pain, constantly unilateral, was localized to the fronto-parietal region, (right n = 6, left n = 2, with side shift n = 1). Moreover, eight patients reported other pain locations, bilateral in four cases, affecting different areas, in particular the vertex and the occipital region (Table 3).
Accompanying symptoms
These were reported only by two patients (tearing, nasal congestion, and conjunctival injection, n = 1; only tearing, n = 1). No patients complained of nausea, vomiting, photophobia, phonophobia, osmophobia, ptosis or aura. All the patients felt anxious during the attacks.
Consistency of attacks
In 10 patients (13.5%) the same type of headache recurred consistently on separate flights, always on landing and, apart from in one case, irrespective of the flight’s duration. In only one of these cases did the pain also start during take-off. The attacks occurred in more than 50% of flights in 18/74 subjects (24.3%); for these subjects the pain started exclusively during the descent of the plane in 14, both during both take-off and landing in two, and during cruising in two. In contrast, the attacks occurred in less than 50% of flights in 10 patients (13.5%): exclusively during landing in nine and also during take-off in one. Three patients had attacks in about 50% of flights, the pain starting only during the descent, while nine other patients have had just one attack (eight on landing and one during take-off). For 22 cases (29.7%) the attacks were occasional and unpredictable. One patient reported the constant occurrence of attacks during landing only in the case of long-haul flights. Another patient had two attacks only during the last two flights, despite flying on average 6–8 times every year; when interviewed, he could not provide further details.
Self-administered manoeuvres
About half of the patients (n = 41/75; 54.7%) performed one or more spontaneous manoeuvres to try and decrease the intensity of the attacks and to obtain some relief, similar to the manoeuvres carried out by patients with migraine, tension-type headache and cluster headache, as previously reported (11). In descending order, the self-administered manoeuvres were: pressure on the pain site (n = 19, 46.3%), Valsalva manoeuvre (n = 11, 26.8%); relaxation methods (n = 3, 7.3%); chewing (n = 1, 2.4%); extension of the ear lobes (n = 1, 2.4%). Three patients performed both pressure and Valsalva manoeuvre and two associated pressure with relaxation. The overall efficacy of these manoeuvres seems to be unremarkable: only seven patients reported a reduction of pain intensity by 25%. Interestingly, one of these patients could achieve complete remission of AH using Valsalva manoeuvre.
Pharmacological treatment
Drugs, time of intake and efficacy (n = 25/75, 33.3%)
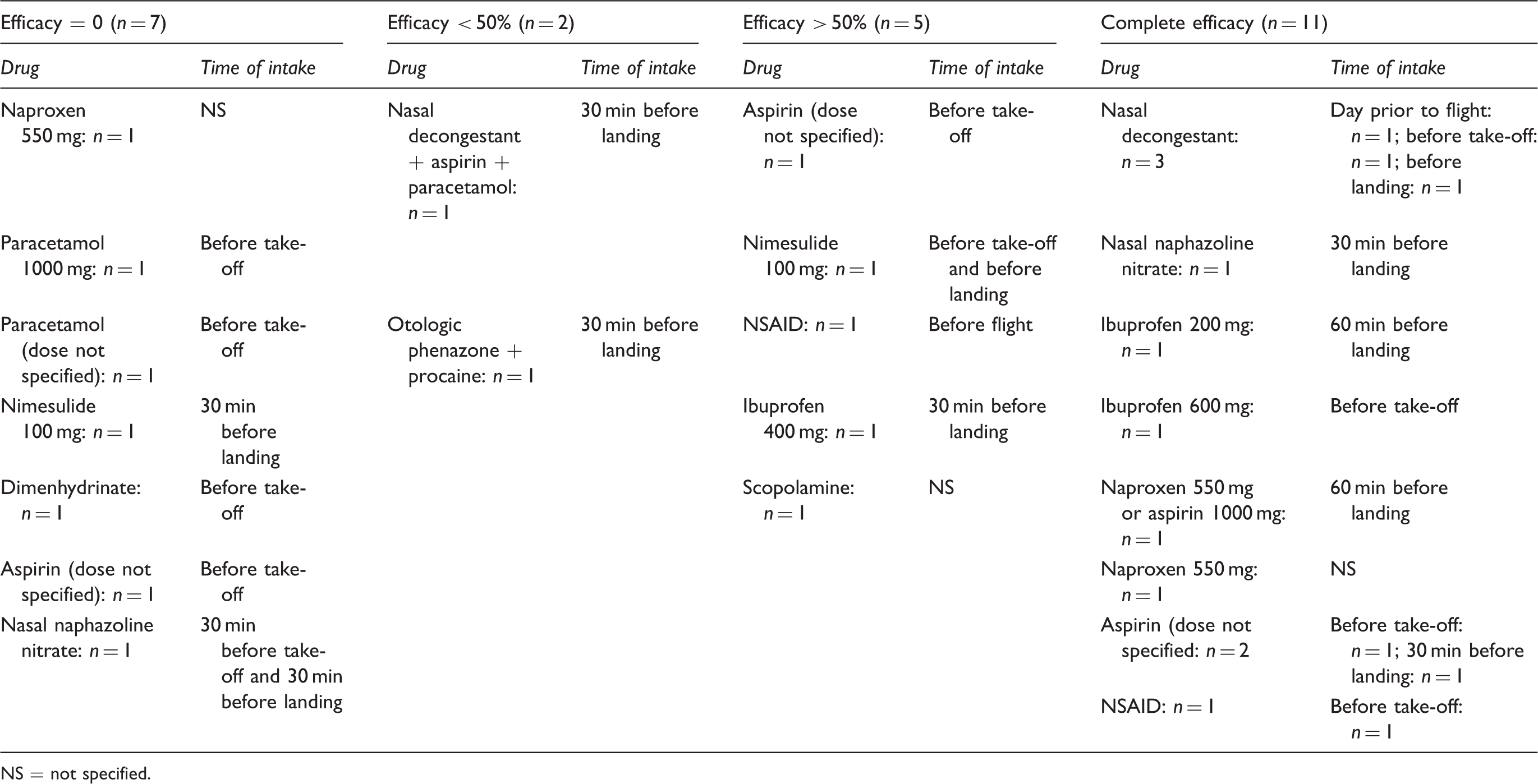
NS = not specified.
Discussion
This paper analyses the clinical features of 75 subjects who reported recurrent, peculiar headache attacks during airplane travel. The first case of AH was reported in 2004 (1) and a case series including six patients was published 2 years later (2). To date 37 extensively evaluated cases have been published in the literature (1–3,6–8,12–17). Because of the paucity of cases of such a peculiar headache, AH was deemed to be relatively rare. In fact, after we published our proposal for provisional diagnostic criteria in 2007 (3), based on the clearly stereotypical features of the attacks, we were contacted by many subjects complaining of a strictly flight-related headache that fulfilled our suggested criteria. The subjects who consulted us by email gave their consent to fill in a rigorously structured questionnaire, thus providing us with all the clinical information required to thoroughly describe the characteristics of this particular entity. A shortcoming of our survey is that, except for three patients who referred personally to our centres, it was not possible to perform a physical and neurological examination on most subjects. Moreover, only one-third of these subjects underwent extensive neuroimaging studies, aimed at ruling out secondary forms of headache, in particular headaches attributed to sinus disorders. For the remaining cases we based our diagnosis on the clearly described and well-characterized symptoms reported by the patients. We believe that the data we collected are conceivably reliable, due to the long-lasting clinical history, the stereotypical features of the attacks, already illustrated in the previously described cases, and the lack of symptoms attributable to sinus disorders (18).
The clinical features of AH are very typical. Males are more commonly affected (61%); the headache onset usually occurs in the fourth decade. Only in a little more than 10% of cases is the first attack concomitant with the first flight and in 13.5% AH occurs constantly during each flight. AH only occasionally starts during take-off or during cruising, but in some of these cases the attacks also occur during landing. In only three patients was AH not associated with landing at all. In the large preponderance of cases (87%) the attacks occurred exclusively during landing. In contrast with other observations, there is no evidence of a role related to different geographic locations of the airports; moreover, two patients reported having experienced the same type of headache also during rapid high mountain descent, six during immersion, four during free diving and two during scuba diving, respectively (3,17).
The headache is unilateral in more than 85% of patients, with side shift in different flights in 11%. It is mainly localized to the fronto-orbital area (77%), but also to the fronto-parietal (12%) region, with its quality being reported as jabbing or stabbing, and occasionally pulsating. The pain starts suddenly, reaching its peak in a few seconds, and subsides within 30 minutes in more than 95% of cases. Only a few patients after the acute phase have a persistent, moderate pain, occasionally lasting for some hours. The headache is reported as severe by all our 75 cases; it is defined as extremely severe/unbearable by more than 85%, the mean severity on the visual scale scoring being 8.8/10. Accompanying symptoms (tearing, conjunctival injection, nasal congestion), strictly ipsilateral to the pain side, were observed in only two patients. Associated nausea, vomiting, photophobia, phonophobia, osmophobia, ptosis or auras (8) have never been reported.
In about 20% of patients there was a past history of sinus infections, but in no case was there any clinical evidence of an active sinus disorder during AH attacks. More than 50% of patients suffer from at least one other form of primary headache. This finding is consistent with the hypothesis of a possible facilitating role of a pre-existing periodical activation of headache pain pathways on AH. Apart from the disability due to the pain severity, the attacks exert a significant emotional impact in about 75% of patients, negatively influencing the possibility of flying again in the future.
The pathophysiology of AH remains speculative. The occurrence of an extremely severe pain during take-off or landing in subjects already affected before the flight by upper respiratory tract or sinus infections has been known for a long time and has been taken into consideration particularly in aerospace medicine (19). In fact, according to the Aerospace Medical Association guidelines, active conditions such as middle ear and sinus infections are contraindications to flight until released by an otolaryngologist. In the same guidelines the use of nasal oxymetazoline is suggested to treat pain occurring during landing in cases where passengers are flying despite such an infection (20). However, a direct aetiological role of acute sinus inflammatory disorders underlying AH is reasonably excluded for our patients complaining of AH. The sudden onset and the quick resolution of AH pain without subsequent signs or symptoms attributable to sinus disorders, the absence of abnormal findings on radiological and physical evaluations, when performed, make an inflammatory process as a possible cause of AH unlikely in the majority of cases. The physical changes in the paranasal sinuses due to the modification of external ambient pressure according to Boyle’s Law are well known. Boyle’s Law maintains that at a given temperature, the volume of gas varies inversely with the pressure exerted on it. During airplane flights, on ascent the air in the paranasal sinuses will expand according to Boyle’s Law, contracting during descent. In normal conditions, the sinuses drain into the nasal cavity through small ostia, which permit mucociliary clearance and ventilation that equilibrates pressure. Under normal circumstances, the intranasal–intrasinus pressure differential is zero, as pressure changes are freely equilibrated through patent sinus ostia. However, when the opening is obstructed or narrowed, pressure equilibration becomes impaired, causing abnormal pressure differences. During take-off, in case of reduced patency of sinus ostia the decrease of barometric pressure is followed by an expansion of intrasinus gas volume, affecting the walls of the sinus and producing pain. During landing the situation is reversed, in relation to the rapid increase of barometric pressure. If ostial patency is marginal, increasing atmospheric pressure cannot be equilibrated within the sinus and a relative negative pressure environment develops inside the sinus. The pressure in the obstructed sinus remains relatively low, resulting in a vacuum effect, sometimes referred to in the literature as ‘the squeeze’. This vacuum effect may be stressful to the sinus mucosal lining and may cause mucosal oedema, transudation, and submucosal haematoma. This phenomenon is called sinus barotrauma, which is a disorder with acute mucosal inflammation of the sinuses caused by an inability to equilibrate the pressure in the sinuses during changes in ambient pressure. In most cases of sinus barotrauma, localized pain in the frontal area, which can be severe and sharp, is the predominant symptom (21–25).
The physiological intrasinus changes due to ambient pressure modifications during airplane travel cannot explain why only a few subjects suffer from AH. On equal terms of external conditions, it could be speculated that all the passengers during a particular flight should experience a headache. Nor can individual theoretical abnormalities of paranasal sinus ostia completely elucidate AH physiopathology, because in an individual subject AH can start after several normal flight experiences and does not recur consistently in following flights (only 10/75 patients report the constant occurrence of AH during each flight). Therefore, the most likely AH physiopathology seems to be related to a variety of multimodal contributing factors: anatomic factors, such as acquired or congenital abnormalities of sinus outlet, environmental factors (cabin pressure, aircraft speed, angle of ascent/descent, maximum altitude), concurrent factors that act by reducing the sinus ventilation, such as a temporary mucosal oedema, possibly worsened, in predisposed individuals, by the above-reported alterations. As recently reported (14), in our case series two subjects suffered from a headache with the same features during high mountain descent as that experienced. This observation confirms the role played by the rapid change of ambient pressure.
The exclusion of other possible diseases underlying AH is mandatory, given the existence of similar clinical pictures attributable to paranasal sinus disorders.
Interestingly, more than 30% of patients used medications in an attempt to treat their attacks. The subjects who could prevent the pain took heterogeneous drugs, usually analgesics and nasal decongestants. Based on the available data, it is not yet possible to draw definitive therapeutic indications (Table 4). However, the drugs that were demonstrated to be of benefit, in particular NSAIDs, are more likely to provide a significant efficacy when taken about 30–60 minutes before the expected trigger phase of the flight. Recently some authors reported a complete response of AH attacks to triptans, even if they do not specify whether other medications had been of benefit and, if so, to what extent (26). The efficacy of triptans was hypothesized to be related to the activation of the trigemino-vascular system, due to the stimulation of trigeminal nerve endings in nasal and paranasal mucosa (26). If the efficacy of triptans is confirmed in future studies, these drugs could be the first choice medications when NSAIDs and decongestants are ineffective, poorly tolerated or contraindicated.
Headache attributed to airplane travel (‘airplane headache’): proposed diagnostic criteria

Comments: Headache attributed to airplane travel occurs during landing in more than 85% of patients. The vast majority of them are concerned with the fear of suffering from further attacks, thus about 50% fly with anxiety, and 5% give up flying. In only 10% of cases does the first episode occur in association with the first flight experience. About half of sufferers also have other forms of primary headaches. The presence of sinus disorders should be excluded. Preventative strategies reported to be effective include NSAIDs, such as naproxen, taken 30–60 min before the flight phase, usually landing, that triggers the attack.
It seems advisable to recommend, given the large number of patients extensively studied, that AH be included in the third edition of the International Headache Society (IHS) classification. Other authors recently proposed (17) the following diagnostic criteria, based on the direct observation of a new series of 22 patients:
A. At least two severe headaches fulfilling criteria B–C. B. Exclusively during airplane travel, together with: • headache with a sudden and severe onset; • spontaneous decrease in the severe pain when the ascent and/or descent of the airplane are complete (<30 minutes). • C. Not attributed to another disorder.
In our opinion these criteria do not completely incorporate the peculiarities of this headache, leaving some potential differential diagnostic challenges with other forms of headaches, in particular in the group of trigeminal autonomic cephalalgias (TACs), still open. Therefore, we consider more appropriate the proposal of the diagnostic criteria for ‘headache attributed to airplane travel’ reported in Table 5, along with the attached comments.
Conclusions
The ‘headache attributed to airplane travel’ does not appear to be an infrequent disorder. Very typical and not to be confused with other forms of headache related to flight (27,28), it is characterized by severe pain, which provokes disability and anxiety, exerting negative influences on possible future flights. Each year approximately 1 billion people travel by air on domestic and international airlines and it has been predicted that in the coming two decades, the number of passengers will double. Therefore, AH will increasingly become a more common and relevant clinical condition. We support its recognition as a new form of headache, to be included in the forthcoming update of the IHS classification, within ‘10. Headache attributed to disorder of homoeostasis’. Its formal validation would favour further studies aimed at improving the understanding of its pathophysiology and implementing preventative measures.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.