
Abstract
Introduction
Airplane headache (AH) is a lesser-known headache disorder that occurs during and is caused by air travel. Although considered rare and current prevalence figures vary widely, it potentially affects millions annually. Risk factors for AH have not yet been adequately investigated, and so the present study aimed to identify risk factors associated with AH among a large cohort of frequent flyers.
Methods
We conducted a survey using an extensive questionnaire that highlighted 30 potential risk factors for AH. We compared individuals experiencing AH with those without headaches and those with other types of headaches. Two multivariate logistic regression models were developed from risk variables and assessed using the area under the curve (AUC) of their receiver operating characteristics, with 10-fold cross-validation applied for reliability.
Results
In total, 2237 questionnaires were analysed; 279 participants reported aircraft headache, while 1563 reported other forms of headache. Model selection resulted in two significant models: model 1, distinguishing AH from no headache, and model 2, differentiating AH from other headaches. Both models demonstrated promising accuracy, with AUC values of 0.794 and 0.595, respectively.
Conclusions
AH notably affects productivity and workdays lost. The identified risk factors align with risk factors for headache in general, as well as headache at high altitudes. Interestingly, folic acid supplementation could have a positive, protective effect. Further research is warranted to explore these relationships and potential preventive strategies.
This is a visual representation of the abstract.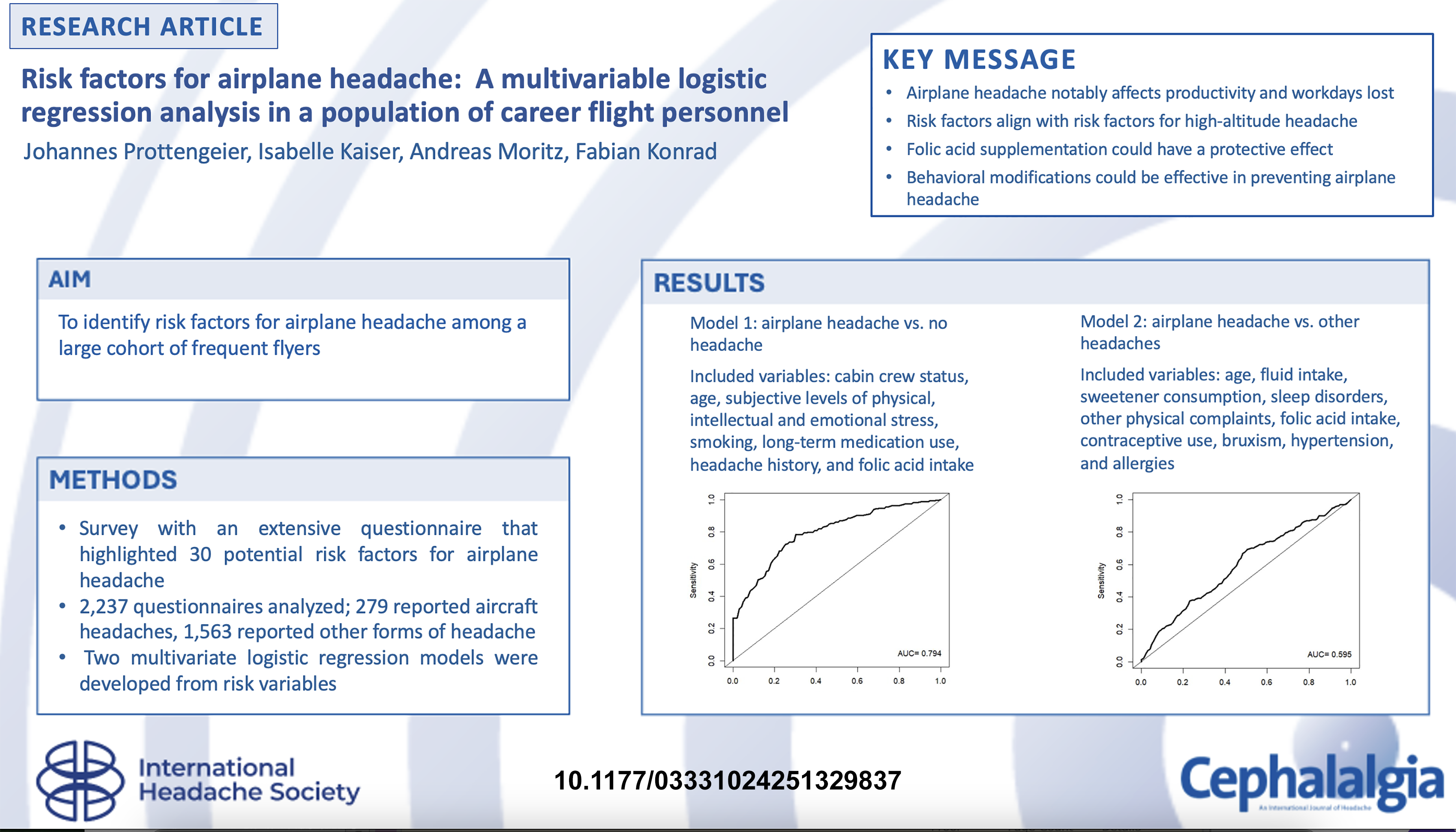
Keywords
Introduction
Airplane headache (AH) is a little-known headache disorder that was first identified in 2004 as “headache associated with air travel” (1). It gained recognition in pain research and was included in the International Classification of Headache Disorders (ICHD) of the International Headache Society (IHS) in 2013 (2).
AH is characterized as short-lasting, often severe, one-sided headache that occurs during and is caused by air travel. Its usual onset is during ascent or descent and subsides after landing (2,3).
Most early data on AH stemmed from small case series and reports, focusing on prevalence, clinical features, diagnostic criteria and treatment (1,4–6). Subsequent studies and experimental trials involving larger populations have refined our understanding of this condition (4,6–9). Despite this progress, the existing literature predominantly addresses prevalence and clinical manifestations rather than the triggers and risk factors associated with AH.
In the literature to date reported prevalence estimates vary widely, ranging from 0.5% to 40% (4,6,9,10). A recent large scale epidemiological study determined a point prevalence of 0.75% (8). Although this figure may seem low, with over 8.6 billion air travellers anticipated in 2023, it translates to nearly 65 million occurrences of AH annually (11).
The risk factors for AH remain underexplored. An experimental study by Bui et al. (7) suggested cerebral vasodilation due to mild hyperventilation and local inflammation in sinus barotrauma as a hypothesis for a pathomechanism. However, comprehensive population-based studies identifying specific risk factors during air travel are lacking.
By contrast, the risk factors for common headache types, such as migraine, chronic daily headache and tension headache, are well researched and documented. These include medication overuse, caffeine consumption, depression, stressful life events, obesity and low educational status (12–14).
Similarly, high altitude headache (HAH), which shares pathophysiological links with AH, and is described in the same subsection of the ICHD-3, is associated with risk factors such as a history of migraine, insomnia, low arterial oxygen saturation, high exertion levels and inadequate fluid intake (3,15,16).
The impact of headaches on productivity and lost workdays is well established, yet specific data for AH is scarce (17–20).
Previous studies have highlighted the emotional burden of AH, with some sufferers reporting stress, flight anxiety and developing avoidance behaviors, with up to 12% of individuals possibly attempting to avoid flying altogether due to the disorder (21,22). For aviation professionals, the implications of AH could lead to substantial productivity losses, increased economic costs and, in severe cases, career changes or incapacitation.
Given this context, our study aimed to identify risk factors for AH through multivariable logistic regression analysis, utilizing data from a large cohort of occupational flyers. This research seeks to inform future preventive strategies and enhance our understanding of AH, leveraging the unique collaboration with two major professional associations for flight personnel.
Methods
Study objectives, design and population
This study aimed to identify risk factors for AH within a large cohort of professional aviation personnel by creating a prediction model. The survey was approved by the ethics committee of the Friedrich-Alexander University of Nuremberg (vote no. 72_14 Bc), ensuring voluntary participation and anonymous data collection.
Recruitment occurred in cooperation with the pilots’ association Vereinigung Cockpit e.V. (VC) and the association Unabhängige Flugbegleiter Organization e.V. (UFO). Invitations to participate in the online survey were sent to all 20,000 members of these associations. Between March and June 2014, a total of 2,400 participants completed the questionnaire via the SoSci-Survey platform over a 92-day period. Inclusion criteria mandated that participants regularly engage in air travel as part of their professional duties. All participants who completed the questionnaire were included in the study without regard to age, gender, professional experience or training, with all respondents assumed to be of legal age due to their membership requirements of a completed aeronautical training.
Questionnaire
The structured questionnaire was developed through discussions among pain specialists in our department, integrating our pain center's headache questionnaire with physiological and logistical considerations pertinent to flights, alongside the diagnostic criteria for AH established by the IHS (2,3).
Participants were categorized into three groups based on their responses: those experiencing airplane headaches (AH), those with other types of headaches (OH) and those without headaches (NH). The NH group answered basic demographic and occupational questions but were not specifically queried about headaches. Participants reporting headaches in their professional practice provided detailed information about prevalence, symptomatology, prior illnesses and potential risk factors. Headache types were differentiated based on symptoms and classified according to the ICHD-3 criteria (2,3) (Figure 1). In detail, all participants answered questions on sociodemographics, as well as information on previous illnesses, nicotine and alcohol consumption, long-term medication, and subjective work related stress in the general section. Participants reporting headaches while flying also answered specific questions about symptoms, accompanying features and management strategies. Ultimately, three groups were established: (NH, AH and OH), so that, in addition to demographic parameters, risk factors from the headache-specific section of the questionnaire could also be depicted.

The definition of headache attributed to aeroplane travel in the International Classification of Headache Disorders, 3rd edition (ICHD-3).4
Statistical analysis
Statistical analyses were performed with R, version 4.4.0. (R Core Team, Vienna, Austria). p < 0.05 was considered statistically significant. Due to the exploratory nature of this analysis, the p-values were not corrected for multiple testing. Sociodemographic characteristics of study participants were reported as proportions or, in case of continuous variables, as mean. Univariate group comparisons of categorical variables such as gender and occupation were performed using a chi-squared test. For continuous variables such as age and body mass index, an unpaired t-test was used. Group comparisons of interest were AH vs. NH and AH vs. OH. Multivariate logistic regression was employed to analyse possible predictors for AH. Two models were developed to compare the AH group against the NH group (model 1) and the OH group (model 2). For model 1, all variables from the survey sections on sociodemographics, previous illnesses, nicotine and alcohol consumption, long-term medication and subjective work-related stress were considered. For model 2, additional headache-specific variables were considered. We tested the potential predictors for multicollinearity before using backward elimination for variable selection. Odds ratios (OR) and 95% confidence intervals were determined for variables included in the final model. Furthermore, overall p-values were calculated using likelihood-ratio tests. The area under the curve (AUC) of the receiver operating characteristic (ROC) curve was calculated as a measure of model performance. To enhance generalizability and mitigate overestimation of the AUC, a 10-fold cross-validation was conducted.
Results
In total, 2504 responses were recorded, with 2237 (89%) fully completed questionnaires included in the analysis.
Among these, 1842 participants (82.2%) reported experiencing headaches while flying; 279 (12.5%) were classified as airplane headache (AH), while 1563 (69.8%) were identified as other forms of headache (OH). Additionally, 395 participants (17.7%) reported no headache (NH) during flights.
Participant ages (mean ± SD) were 37.08 ± 8.44 years for AH, 38.81 ± 8.79 years for OH and 40.6 ± 11.25 years for NH (Figure 2). Notably, the proportion of women was significantly lower in the NH group compared to the AH group (58.5% vs. 29.1%, p ≤ 0.001). The prevalences of female participants were almost similar in the AH and OH groups (58.5% vs. 55.9%, p = 0.44) (Figure 3 and Table 1).

Proportions for age in the AH, NH and OH groups.
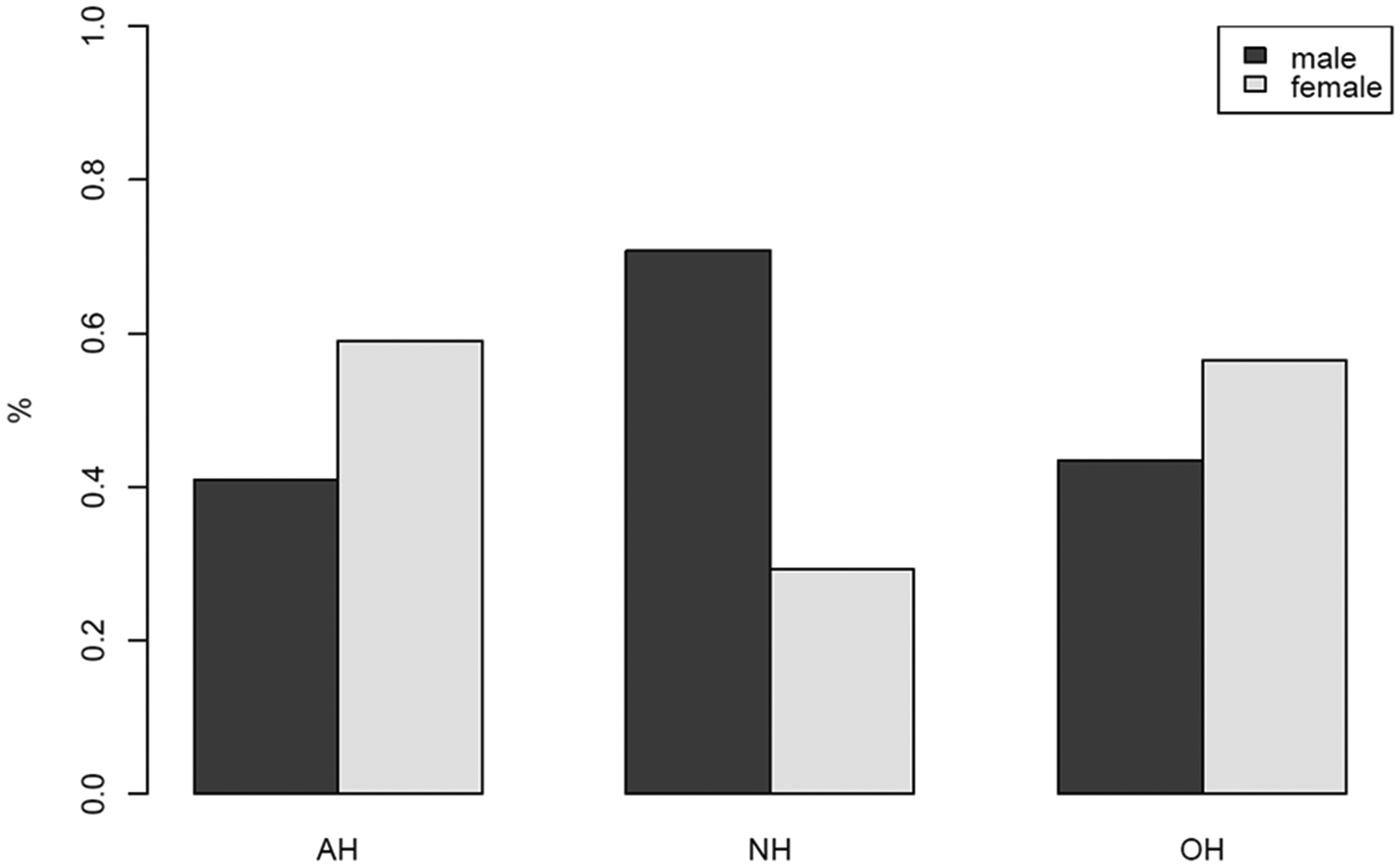
Proportions for sex in the AH, OH, and NH groups.
Gender distribution in passengers with airplane headache (n = 279), other headache (n = 1563) and no headache (n = 395).

AH, airplane headache; OH, other headache; NH, no headache
Occupational distribution showed a skewed representation of cabin crew among respondents, with 75% in the AH group compared to 67.1% in the OH group (p = 0.009) and 36.6% in the NH group (p < 0.001) (Figure 4). The body mass index values (mean ± SD) for the three groups were in a similar range: 22.79 ± 2.80 for AH, 22.96 ± 2.92 for OH and 23.80 ± 3.15 for NH (Figure 5).

Proportions for occupation in the AH, NH and OH groups.

Proportions for BMI in the AH, NH and OH groups.
Regarding productivity loss, 41.9% of AH respondents and 32.6% of OH respondents reported more than five days of reduced productivity per year, while 37% and 35.8% respectively reported two to five days. Additionally, 37 participants (13.9%) in the AH group reported total absence, resulting in 170 lost workdays (0.61 days per person), while 139 participants (11.1%) in the OH group reported 663 days of absence (0.42 days per person).
The one-year prevalence of headache episodes during flights was 96.8% for the AH group and 89.9% for the OH group. The overall one-year prevalence for the whole study population was 74.9%. In the AH group, 43.8% reported headache episodes during over 25% of flights, compared to 30.9% in the OH group (p < 0.001).
The logistic regression model comparing the AH group with the NH group (model 1) demonstrated good predictive power (AUC 0.794) following 10-fold cross-validation (Figure 6). The final model identified ten influential factors: cabin crew status, age, subjective levels of physical, intellectual and emotional stress, smoking, long-term medication use, headache history, and folic acid intake (the sole protective factor) (Table 2). All factors, except for subjective intellectual challenges and smoking, significantly influenced the occurrence of AH (p ≤ 0.05)

Model 1, AH vs, NH: receiver operating characteristic curve and area under the curve (AUC). AH, airplane headache; NH, no headache.
Influencing factors for airplane headache in model 1, comparing the AH group (n = 279) vs. the NH group (n = 395).

AH, airplane headache; NH, no headache. *p-values from likelihood-ratio tests
The presence of a pre-existing headache condition had the highest effect (OR = 1.59).
Medication use, higher stress levels, and working as cabin crew had similar effect sizes (OR = 1.09, 1.15 and 1.17, respectively). Higher age and folic acid intake exhibited a protective effect on the occurrence of AH (OR = 0.99 and 0.77).
In model 2, the predictive power for the comparison of the AH group with the OH group was low after 10-fold cross-validation (Figure 7).

Model 2, AH vs. OH: Receiver operating characteristic curve and area under the curve (AUC). AH, airplane headache; OH, other headache.
This model also included ten influential factors: age, fluid intake, sweetener consumption, sleep disorders, other physical complaints, folic acid intake, contraceptive use, bruxism, hypertension and allergies (Table 3). A significant influence (p ≤ 0.05) was only observed for four of the risk factors: age, sweetener use, sleep deprivation and hypertension.
Influencing factors for airplane headache in model 2, comparing the AH group (n = 279) vs. the OH group (n = 1563).
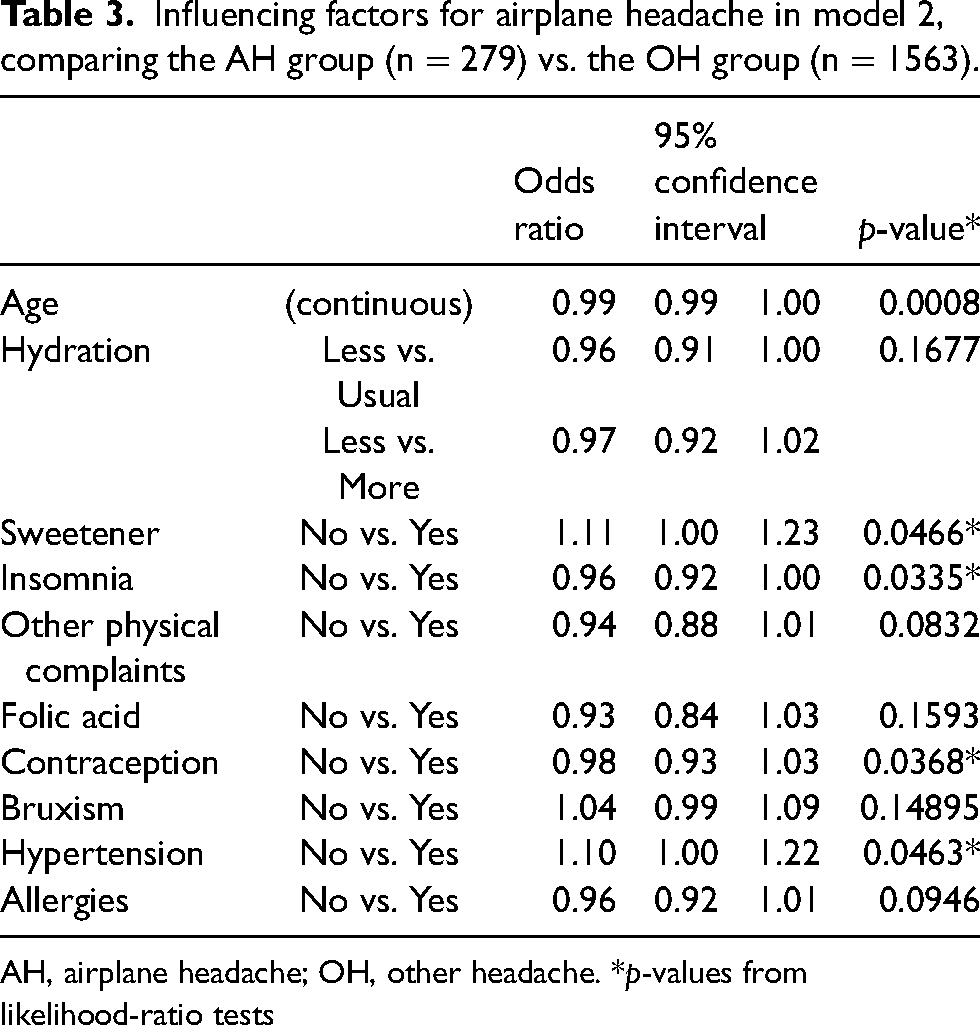
AH, airplane headache; OH, other headache. *p-values from likelihood-ratio tests
Non-significant risk factors included hydration, other physical complaints, folic acid intake, contraceptives, bruxism and allergic disposition, all of which displayed negligible effects on AH occurrence.
Discussion
Prevalence
AH may not pose a life-threatening risk due to its transient nature, but its prevalence among air travellers, particularly in the present study, which found a 12.5% period prevalence in professional flyers, highlights its significant impact. This contrasts with the lower point prevalence of 0.75% reported in a broader study of air travellers, underscoring the inconsistency of AH triggers despite the constant presence of air travel as the primarily trigger (4,8). This once again emphasizes the need for research into risk factors and triggers.
The one-year prevalence of 74.9% in our cohort indicates that many individuals are likely to experience recurrent episodes, with 30–44% reporting headaches in more than 25% of their flights.
Gender issues
Our findings align with previous research indicating a higher incidence of AH among women, consistent with studies by Bui et al. (4) However, other literature presents mixed results regarding gender distribution, with some studies finding no significant differences or a male predominance (10,21,23). Skewed gender distributions are also known for primary headaches, with more men tending to be affected by tension headaches, while migraine disproportionately affects women, with a three-fold higher risk (24,25).
Loss of productivity
The data reveal a lower productivity loss due to AH compared to other headache types with a sickness absence of 0.6 days in 12 months, compared to up to 9.7 working days in three months (17,20). This could be attributed to the short duration of AH and its predictable cessation after landing, which reduces the likelihood of sick leave. However, the performance impairment, during flights caused by AH, but does not lead to sick leave and total absence should also be addressed, because it was reported by almost 42% of those affected. Cockpit and cabin crew perform critical tasks and safety-relevant activities on board and this raises concerns about safety and operational effectiveness with respect to whether AH could have an influence on the process and result quality of these activities, especially in view of the fact that AH occurs more frequently in the particularly critical flight phases of climb and descent (2,3,5,6,10,21,26,27).
Risk modelling
In our first predictive model comparing AH with NH, several significant risk factors were identified, including cabin crew status, elevated levels of emotional and physical stress, younger age, and long-term medication use. While none had exceptionally high odds ratios, their clustering suggests that certain combinations of factors may significantly increase risk.
Mainardi et al. repeatedly described the emotional stress associated with AH in over 70% of those affected and can lead to avoidance behaviours in some individuals. This ranges from a fear of flying in over 50% of those affected to a strict avoidance of further air travel in as many as 4% of cases (21,22). With regard to the population of commercial airline pilots in the present study, one can speculate whether the emotional stress associated with AH could be a reason for a certain proportion of those affected to change their profession. This mechanism could explain the decreased prevalence of AH with age.
Stress, regular medication use and the presence of comorbidities presenting as risk factors for AH overlap with findings already observed in relation to other recurrent and chronic headaches (12,14). As the most potent risk factor, the presence of a headache diagnosis increases the risk by 60%, and so people with chronic headaches can be categorized as particularly vulnerable to AH.
In the second prediction model comparing AH vs. OH, few significant differences emerged, reflecting the shared risk factors between AH and other forms of headache. This is clearly reflected in the low AUC-ROC of the prediction model. Only the consumption of sweeteners and hypertension showed statistical significance, indicating a nuanced relationship between AH and other headache forms.
The overlap in risk factors between AH and HAH (i.e. migraine, low oxygen saturation, high level of exertion, reduced venous return, dehydration) suggests shared pathophysiological mechanisms, although the exact processes differ (2,3,15,16). Bui et al. (4) also described that patients with a history of HAH are more prone to AH.
Despite this overlap in risk factors and the large overlap in clinical impression, which is also reflected in the similar diagnostic criteria in the ICHD-3, there are two different explanations of the underlying pathophysiology for AH and HAH (2). For AH, mild hyperventilation and local inflammation due to sinus barotrauma are considered primary contributors (7,28). By contrast, HAH is linked to reduced barometric pressure and hypoxia (29–31). Both conditions may lead to acute intracranial vasodilation with cerebral edema and subsequent severe pulsatile headache with the distinctive sudden onset, although the mechanisms remain distinct.
The influence of aspartame and sucralose as triggers for other types of headaches, such as migraines or tension headaches, is already well described (32,33). Interestingly, in conjunction with other factors, as described in the model, sweeteners may trigger airplane headaches more strongly than other headache forms.
Protective factors
A notable finding from our analysis is the protective effect of folic acid intake, which appears to reduce the risk of AH by 5–37%. This is consistent with earlier findings highlighting the benefits of folic acid in migraine patients since the 1950s, especially in combination with pyridoxine (vitamin B6) (34–36). The underlying mechanism is not yet fully understood, but potentially is a result of its role in lowering homocysteine levels, which are associated with mitochondrial function and cerebral energy production (34,36).
In conclusion, the combination of working as cabin crew, experiencing a stressful work environment and having a history of headaches are associated with an increased risk of airplane headaches. Conversely, folic acid intake offers a protective effect, suggesting potential avenues for prevention and management in affected populations. Further research is needed to clarify these relationships and explore additional preventive measures.
Limitations
Our study has several important limitations that must be considered.
First, the “healthy worker effect” may influence our findings. This phenomenon suggests that, over time, healthier individuals are more likely to remain in the workforce, potentially leading to an underestimation of the prevalence of AH among professional flyers. As a result, those most affected by AH might be less represented in our sample.
Additionally, there is a potential for positive selection bias. Individuals experiencing symptoms of AH may be more inclined to participate in an online survey about headaches, leading to an overrepresentation of those affected and possibly skewing the prevalence estimates.
The study design, relying on email invitations for an online questionnaire, presents another limitation. Participants did not have the opportunity to seek clarification during the survey, which could have led to misunderstandings or incomplete responses. Furthermore, the variable time gap between headache episodes and survey completion may introduce recall bias because participants might struggle to accurately remember their experiences. Despite these drawbacks, the anonymity of the online format may have encouraged more candid responses compared to face-to-face interviews, where individuals might feel pressured to underreport health issues due to the high health standards in aviation.
We acknowledge the complexities introduced by these biases and recognize that their effects on our findings are difficult to quantify. Future research should aim to address these limitations, perhaps by incorporating more structured interviews or longitudinal designs to better capture the experiences of both affected and unaffected individuals.
Conclusions
The present study did not identify any exclusive risk factors for AH; rather, the risk factors identified are largely consistent with those known for chronic headaches. Notably, parallels were observed between the risk profiles for AH and HAH, likely due to the similar climatic conditions experienced during air travel.
Given that the identified risk factors for AH overlap with those for other headache types, future research should explore the applicability of established prevention strategies for chronic headaches in the context of AH. In particular, the protective effects of folic acid, which have been debated for decades, warrant further investigation.
Regarding the possible influence on the decreased prevalence with age through severe cases of AH leading to career changes in commercial flight crews, further investigations appear to be warranted.
Clinical implications
The risk factors for AH in this large population of air travellers align with generally established risk factors for other headache forms. Significant similarities exist between the risk factors for AH and HAH. Behavioural modifications, such as ensuring adequate hydration, reducing stress and avoiding sweeteners, should be explored for their potential effectiveness in preventing AH. The effectiveness and safety of folic acid supplementation as a preventive measure against AH should be examined in more detail.
Footnotes
Acknowledgements
We are grateful to all volunteers for their participation in our study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical statement
The Ethics Committee of the Friedrich-Alexander University Erlangen-Nuremberg approved this study on 14 March 2014 (Decision 72_14 Bc). The need for written informed consent was waived because of the voluntary, anonymous and observational nature of our study.