
Abstract
This study presents six cases of headache that appeared only during flights and was not associated with other headache forms. The cases had severe headache attacks during some flights, when the plane was landing and taking off, with a unilateral and generally orbital and/or supraorbital localization. The attacks lasted between 15 and 20 min on average and recovered spontaneously, without any accompanying sign. We think that barotrauma caused by pressure changes in the cabin during take-off and landing could affect ethmoidal nerves (branching from the ophthalmic branch of the trigeminal nerve) that carry the senses of the mucosa on the inner surface of the paranasal sinuses, and/or nociceptors in ethmoidal arteries, thereby activating the trigeminovascular system and leading to headache.
Introduction
A case report published recently introduced a new form of headache called ‘airplane headache’ that appeared during flights (1). There are no detailed clinical data about this new headache and the mechanism underlying this phenomenon is not clear. This study presents six cases of headaches that were not associated with other headache forms and that developed during flights. Detailed clinical data about the cases are presented and the possible underlying mechanisms responsible for this kind of headache are reviewed.
Case reports
Case 1
A 42-year-old man had had his first headache attack 2 years previously and it had since recurred four times. All attacks had the same clinical characteristics. When the plane started to descend a severe jabbing pain suddenly developed in the right eye. Throughout the attack the pain remained localized in the right eye. Only in the last attack did the pain affect the right forehead and temple also. The pain reamined severe until the plane landed (15, 20 min on average). After the landing, the pain alleviated spontaneously and recovered completely in 30–40 min. There were no accompanying symptoms of throbbing, lacrimation or conjunctival injection, blurry vision, nausea or vomiting. The patient, who had been traveling by air for 5 years, had had this headache during some, but not all flights. He said that the headache appeared particularly when the plane was landing at the airports of seaside towns. He has no abnormality in his personal and familial history. Additionally, he has no other history of headache. His neurological, ophthalmological and ear–nose–throat (ENT) examinations were normal. Routine blood analyses, cranial magnetic resonance (MR) and paranasal sinus tomography were normal.
Case 2
A 40-year-old man had had his first headache attack 1.5 years previously and the attacks had recurred three times since. All attacks had the same characteristics. About 5–10 min after the plane took off, when it was still gaining altitude, a severe jabbing pain would suddenly start in the left eye and supraorbital region. The pain remained severe for 15 min. It would then start to alleviate spontaneously and recover in 15–20 min. No other symptom (nausea, vomiting, throbbing, lacrimation or conjunctival injection) accompanied the pain. The patient preferred to stay immobile, holding his eye with one hand during the pain. He said that he had been flying for 8 years, but has not experienced similar pain in all his flights. Neither he nor his family had any history of disease or headache. Neurological, ophthalmological and ENT examinations were normal, as were routine blood analyses, cranial MR and paranasal sinus tomography.
Case 3
A 33-year-old man had had his first headache attack 7 months previously and it had recurred twice since. He had been traveling by air for 5 years. The attacks had the same clinical characteristics. When the plane started descending, the patient suddenly felt a very severe jabbing pain in his right eye. He described this as the most severe pain of his life. The pain continued that way for 15–20 min. After the plane had landed, severity of the pain declined sharply and disappeared in 10–15 min. The patient preferred not to move during the pain. There was no other accompanying symptom. One of the attacks came when landing at an airport by the sea. The migraine history of the patient was around 10 years. He had migraine headaches without aura once or twice a month. He has no other characteristic in his personal or family history. His neurological, ophthalmological and ENT examinations, as well as routine blood analyses, cranial MR and sinus tomography results, were normal.
Case 4
A 36-year-old man had had his first headache attack 3 years previously, the second 1.5 years and the last one 15 days previously. The clinical characteristics of all three attacks were the same. When the plane started descending, the patient suffered from a severe jabbing pain in a restricted area of the right supraorbital region, accompanied by a stuffy feeling on the same side of the face and nasal congestion. The pain lasted about 15 min, spontaneously diminished and resolved in 25–30 min. The patient stated that he had all three attacks when landing at airports of seaside towns and that he did not have headaches in other flights. He had been having exercise headache for 15 years. The patient did not have any other disease and his neurological, ophthalmological, ENT examinations and routine blood analyses, cranial MR and sinus tomography results were normal.
Case 5
A 37-year-old man had had his first headache attack 4 years previously and it had since recurred four times. He had been flying occasionally for 6 years (two or three times a year). He had noticed that three of these attacks happened when landing at airports by the sea. The pain had the same characteristics in all attacks. A severe pain started suddenly in the right eye and around a short time (3–5 min) after the plane started to descend. The pain remained severe for about 15–20 min until the plane landed, and diminished and disappeared within 20–30 min after landing. The patient had no specific characteristic in his history or in his family, and neurological, ophthalmological, ENT examinations as well as routine blood analyses, cranial MR and sinus tomography results were normal.
Case 6
A 36-year-old man had had his first headache attack 1 year previously, during the descent of the airplane to an airport near a seaside town. The patient described the pain as sudden, stabbing at the right periorbital area and right half of the face, resembling the blast of a bomb on the head; the attack lasted around 15 min. The pain diminished when the plane landed and ceased in 30 min. No other symptom, such as nausea, vomiting, lacrimation, nasal congestion or conjunctival injection, accompanied the pain. The attack had recurred three times since then. All three pain attacks happened during landing at the same airport and their features were the same. He also had a history of retinal migraine at the right eye, with two or four attacks per year in the last 4 years. There was no additional pathological condition. Ophthalmological, neurological and ENT examinations of the patient were normal, as were cranial MR and sinus tomography results.
Discussion
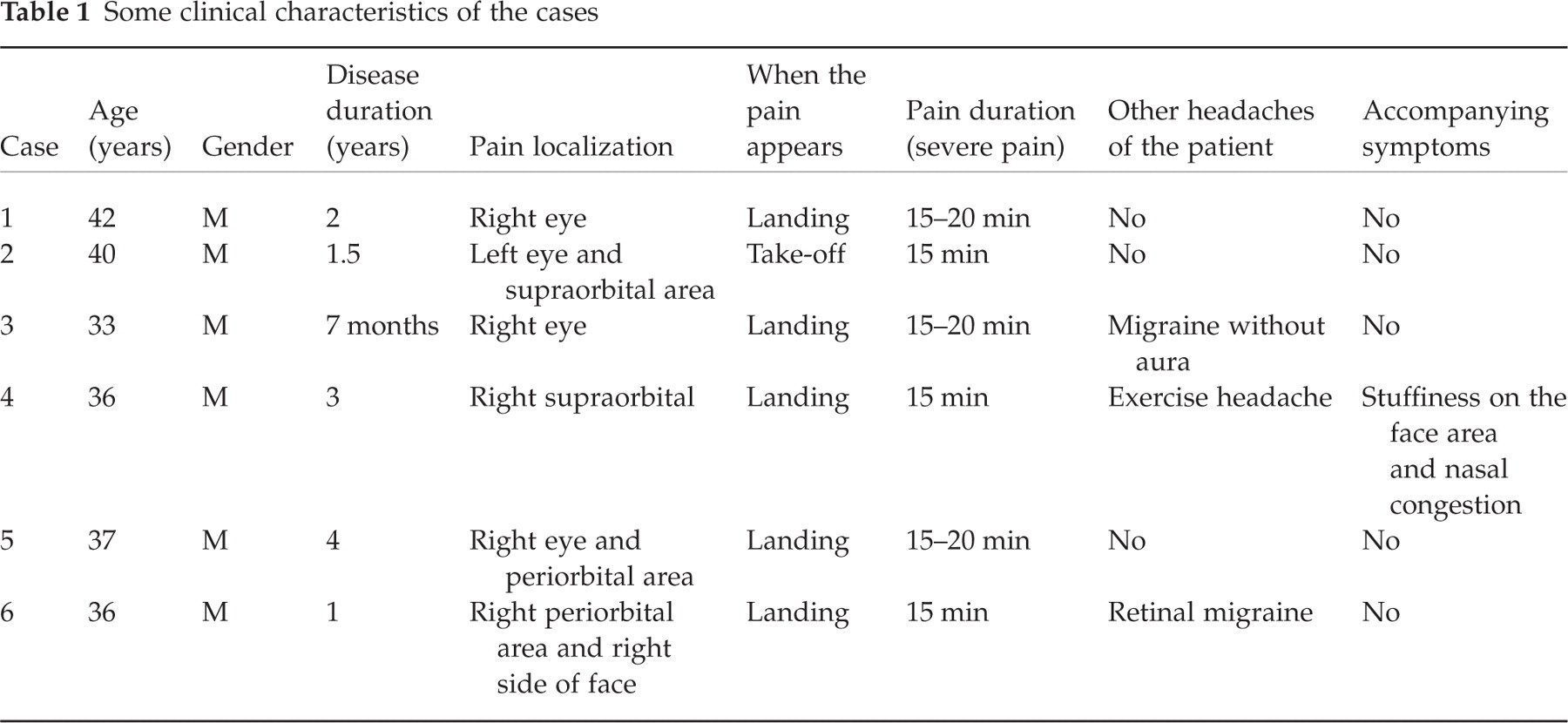
All the patients were male, with mean age 37.3 years (range 33–42 years). Mean age at onset was 35.4 years (32–40 years) and disease duration 2.1 years (7 months to 4 years). The headache had a unilateral localization on the head (especially in the right orbital region) in all cases. The pain was severe in all cases and the mean duration was 15 min (equating to the descent and ascent period of the plane). Only case 4 had accompanying symptoms. One patient (case 2) had headache during ascent of the plane, while the other five felt pain during descent.
The case reported by Atkinson and Lee was also male (1). In this case headache was on the forehead and midline (1). This case, on the other hand, had headaches twice in a single flight, one during take-off and the other during landing (1). Similarly, that case suffered headaches on all flights, whereas our cases had headaches in some flights and not in others. There are significant clinical differences between our cases and the case in the literature.
Some clinical characteristics of the patients are given in Table 1.
Some clinical characteristics of the cases
The fact that all patients were male and that their headaches were severe, short lasting, unilateral, with periocular localization suggests the characteristics of cluster headache. However, none of the patients had a history of cluster headache and the attacks were not exactly compatible with the characteristics of this type of headache. Nevertheless, we do not know whether all of the patients being male has any significance. Our patients have not been followed up for long enough to know the natural history.
The fact that headache attacks come during flight may suggest a similarity to high-altitude headache. However, duration, localization, severity of the headaches and lack of accompanying symptoms imply that these are of a different type. Besides, although high-altitude attack is relieved as the altitude decreases, most of our cases suffered from the headaches during the descent of the plane.
There are no data concerning the aetiology of this type of headache. In one case report, the authors discuss a patient who experienced symptoms of an acute right frontal, intraparenchymal pneumatocoele, which is a rare complication of an ethmoid sinus osteoma that eroded upward through the dura mater while on an aircraft descending to an airport. In this case, the change in cabin pressure probably destroyed the eroded cribriform plate and dura mater through an external effect and caused an intracranial pneumatocoele (2). In another report, Segev et al. has described a passenger who had acute and severe headache in the right frontal area during the descent of the plane (3). Examination of the case showed nasal septum deviation, inferior concha hypertrophy, as well as oedema and inflammation in nasal mucosa. In the MR examination performed a week later, they found a polypoid mass in the right frontal sinus, which they diagnosed as submucosal haematoma. They stated that the signs and symptoms were associated with sinus barotraumas resulting from an abrupt change in ambient pressure (3).
A rapid change in ambient pressure occurs during the descent of the plane or the diving of divers (3, 4). An interaction then takes place between the pressure gradient of the surfaces containing air in the body and rapidly changing ambient pressure. This condition, resulting from the direct effect of the ambient pressure and possibly leading to tissue injury, is defined as barotrauma (3–5). Rapidly changing ambient pressure compromises normal sinus outflow in divers and plane passengers who have inflammatory mucosal thickening in the sinus, polyp and/or structural nasal deviation (3). This leads to sinonasal barotrauma (3, 5). The pressure within the sinus where there is an obstruction will be lower relative to the ambient pressure during descent of an airplane and this causes a vacuum effect, sometimes referred to as ‘the squeeze’. The vacuum effect may cause tension in the mucosal lining of the sinus, thereby leading to mucosal oedema, serosanguineous exudate and submucosal haematoma (3). When the plane is ascending, the ambient pressure increases. This condition, sometimes referred to as ‘reversed squeeze’, leads to barotrauma to a lesser extent and by different mechanisms (3). Weissman et al. clinically graded sinus barotraumas according to severity (5). In Grade 1, there is a temporary discomfort in the sinus, which quickly recovers. Plain radiography examinations are normal and there may be only a slight mucosal oedema (5). In Grade 2 there is pain that diminishes in less than 24 h. Plain radiography may show mucosal thickening. These two are relatively mild phases and may arise in both the squeeze and reversed squeeze situations. Grade 3 is the most serious phase. The pain starts suddenly and severely, and rarely lasts more than 24 h. Plain radiography may show a polypoid mass due to liquid level and/or submucosal haemorrhage and free bloody exudates (5).
Headaches in our cases had supraorbital and orbital localization, were always unilateral, were relieved after the plane landed and disappeared in a short period of time. Headache characteristics of the cases reported by Mahabir and Segev et al. have similarities with those in our cases. Nonetheless, both of these cases had an organic pathology in the sinus that was identified clinically and radiologically and the headache attack occurred only once. Headache attacks of our patients, on the other hand, were recurrent and, most important, examinations and assays were normal. We think that the vacuum effect that appeared in our cases, particularly during the descent of the plane, may lead to a Grade 1 or Grade 2 barotrauma as defined by Weissman. We believe that this effect develops particularly in the ethmoid sinuses. Ethmoid sinuses consist of chambers called ethmoid cells, each with its own mucosa, innervations, ostium and pneumatization (6). The anterior ethmoid artery that supply these areas originates from the orbit, passes through the ethmoid cells, enters the cranium and re-enters the nasal cavity at the level of cribriform plate and septum (6). When passing through the ethmoid sinus, this artery is in close relationship with ethmoid cells, which vary according to the individual, and right and left localization. This relationship is determined by the genetic and/or random pneumatization pattern of the ethmoid cells. In addition,
It was interesting that not every boarding of an aircraft occasioned a headache. The flights in which the patients had headache probably had a subclinical condition which did not cause major discomfort for the patients, but affected the ethmoid sinuses. This subclinical condition caused congestion and inflammation in the ethmoid sinus and middle turbinate mucosa. Thus, the vacuum effect that appears especially during the descent of the plane may trigger a headache by causing barotrauma in the ethmoid cells, whose aeration is partly impaired. In addition, three patients had a long history of smoking. A change in the physiology of the concerned sinuses during flights during heavy smoking periods may lead to inflammation and oedema. As a result, sinus ventilation may be impaired, creating a disposition to barotrauma, and headache attacks. However, the cases presented at our clinic on average 3 weeks after the last headache attack. Their ENT examination findings were within the normal range and those changes had possibly resolved.
Additionally, the headaches were almost always unilateral, and mostly on the right side. We believe that unilateral headache may be explained by the wide variation in ethmoid cell ostia and pneumatizations, as stated above, and/or the ethmoid sinus mucosa on one side being affected more than that on the other side. Right-sided localization of the headache may be coincidental, as the number of our cases is very low.
It is worth noting that most of the attacks in a majority of our cases developed when the planes landed at airports at seaside towns. Meteorological conditions vary between seaside towns and those inland. Likewise, meteorological conditions may also change considerably between seasons, and even days. Atmospheric meteorological conditions can influence cabin pressure. These factors may explain why patients suffered headache attacks when landing at seaside airports and why they had headaches on some flights and not on others.
In conclusion, Atkinson and Lee named the headache form they described ‘airplane headache’ (1). We think that since the most probable cause of this type of headaches is barotrauma, it is appropriate to designate them as ‘barotrauma headache’ or ‘barotrauma-related headache’.