
Abstract
Background: Glutamate receptors are implicated in central nervous system (CNS) pain pathways, including trigeminovascular activation, central sensitization, and cortical spreading depression.
Methods: We investigated the influence of the N-methyl-
Results: Pretreatment with memantine significantly attenuated formalin-induced pain behavior (p < 0.01) and the sensory threshold for VFMF (p < 0.001). In the TCC, the increase in formalin-induced Fos immunoreactivity was significantly attenuated in the memantine group (p < 0.01).
Conclusion: The present study demonstrated that the NMDA receptor antagonist memantine inhibits the nociceptive process from trigemino-ophthalmic nerve endings to the TCC.
Introduction
Glutamate, a major excitatory neurotransmitter in the central nervous system, has a vital role in the mediation of synaptic transmissions (1,2). Electrophysiological and behavioral studies point to glutamate receptors as being essential for the spinal transmission of nociceptive information in physiological and pathological conditions (2–5). Administration of glutamate agonists can result in mechanical or thermal allodynia and hyperalgesia, known to be associated with the central sensitization of pain processes (6). Glutamate antagonists have repeatedly been shown to inhibit pain-related responses as well as to enhance opioid-induced analgesia (7–9).
Pain relay structures, including the trigeminal ganglion, trigeminocervical complex (TCC), and thalamus, contain glutamate-positive neurons (10,11). Glutamate activates neurons in the trigeminal nucleus caudalis (TNC) by acting on ionotropic glutamate receptors and is involved in signaling from the spinothalamic tract (12,13). Many experimental studies with glutamate have reported significant effects in pain pathways, but clinical studies in humans have not been conducted because of concern about various side effects that may obscure the therapeutic potential (14)
N-methyl-
The non-competitive NMDA receptor antagonist dizocilpine maleate inhibits neuronal firing in the trigeminocervical complex following electrical stimulation of the superior sagittal sinus (17). There have been two studies evaluating the effect of memantine on pain perception; both evaluated only behavioral aspects of memantine using neuropathic and orofacial pain models (18,19). Clinically, memantine demonstrated significant effects in reducing headache frequency and disability when given as a preventative treatment for refractory migraine in an open-label study; side effects are uncommon and generally mild (20). On the basis of these results, it is reasonable to hypothesize that memantine may have an inhibitory role in central pathway pain perception located in the TCC, but no study has yet directly demonstrated this relationship.
The current study used a formalin injection model, which has previously been shown to cause activation of a number of nuclei involved in the dorsal horn of the spinal cord in experimental animals (21,22). Subcutaneous formalin activates the Aδ and C nociceptors of sensory nerve endings and induces intense nociceptive input, with effects lasting 45–60 min, as assessed by behavioral observations (23) and electrophysiological recordings (21). This was shown to be a reliable method for assessing pain and has been used successfully in several recent studies. We used identification of the protein product of the immediate-early gene c-Fos as a marker of cellular activation; it is rapidly and transiently expressed in response to neuronal stimulation (24). Previous studies have reported consistently that neurons within the TNC express Fos in response to irritant stimuli to pain-producing structures. We investigated the effect of memantine on trigeminocervical nociceptive responses after formalin injection to the trigemino–ophthalmic-innervated dermatome from the point of view of morphological and functional aspects.
Methods
Animal preparation
Experiments were conducted after ethical review by the Institutional Animal Care and Use Committee at the Catholic University of Korea (approval number: UJA2011-02A). Male Sprague Dawley (SD) rats (200–250 g) were housed in standard plastic cages with sawdust bedding in a temperature-controlled room (23 ± 1°C) under a 12-h/12-h light/dark cycle. All procedures took place in the light phase, between 11:00 and 19:00 in a quiet room. Animals were randomized in a double-blind manner and were administered pretreatment with vehicle or memantine 30 min before the formalin injection.
Formalin was diluted in 0.9% saline to a concentration of 2.5%. A 50-μl bolus was then injected subcutaneously (s.c.) into the left side of the face over the upper eyelid, which corresponds to a trigemino–ophthalmic-innervated dermatome. To ensure calm, the injections were made under brief anesthesia, induced with enflurane through a nasal mask (Laboratoire Belamont). Anesthesia was discontinued when the first eye blink was observed. Under these conditions, the typical time for reawakening was less than 10 s. The animals were then placed in the 30 × 30 × 30-cm test box with three mirrored sides for a 60-min observation period. The rats did not have access to food or water during the test. Before formalin injection, the animals were usually placed in the same box for an acclimation period of 30 min. The observed responses involved two phases of rubbing. The first phase started 15–30 s after the test injection of formalin and lasted for 0–5 min. After a time of relative inactivity, a second phase of intense rubbing activity lasted 15–60 min after the injection. The recording time was divided into 12 blocks of 5 min, and a pain score was determined for each block by measuring the number of seconds that the animal spent rubbing the injected area with the ipsilateral forepaw. The data collected between 0 and 5 min post-formalin injection represented the early phase and the data collected between 15 and 60 min post-formalin injection represented the late phase. Behavioral analyses were performed by an investigator who was blinded to the animal's group assignment.
For the von Frey monofilament (VFMF) test, each rat was placed in an atraumatic plastic tube restraint, into which the animal entered uncoaxed. Animals were placed inside the testing apparatus for acclimation through the training period. Pressure thresholds were determined by applying the VFMF (Stoelting Co., Wood Dale, IL, USA) to the face over the periorbital region on both sides. The monofilaments were presented in a sequential ascending or descending order, to determine the threshold of response (25,26). A positive response to the VFMF was considered present when the rat showed recoil of the head away from the stimulus or vigorously stroked its face with the ipsilateral forepaw. The 66% probability thresholds of a positive response, defined as a positive response to two of three trials with the VFMF, were determined before and 1 h and 2 h after formalin injection.
The animals were then separated into three groups as follows:
Control group – animals received vehicle pretreatment (saline, 1 ml/kg intraperitoneally, i.p.) followed by vehicle injection in the left periorbital area (saline, 50 μl, s.c.; n = 6). Formalin group – animals received vehicle pretreatment (saline, 1 ml/kg i.p.) followed by formalin injection in the left periorbital area (2.5% formalin, 50 μl, s.c.; n = 6). Memantine group – animals received memantine pretreatment (10 mg/kg, i.p.) followed by formalin injection in the left periorbital area (2.5% formalin, 50 μl, s.c.; n = 6).
Tissue preparation and immunohistochemistry
Following the experiment, the animals were killed by perfusion via the ascending aorta with 0.9% saline (50 ml), followed by 4% paraformaldehyde (50 ml) in 0.1 M phosphate-buffered saline (PBS, pH 7.4). The brain and spinal cord were removed and stored overnight in the same fixative and then placed in a cryoprotectant solution (20% sucrose, 30% ethylene glycol in 0.1 M PBS) for 48 h before sectioning. The brain and upper cervical spinal cord was sectioned serially on a freezing cryostat. Sections (30 µm) that spanned the trigeminocervical complex (trigeminal nucleus caudalis, cervical spinal cord, levels C1, C2, and C3) were collected in PBS.
Tissue sections were processed as free-floating sections. Sections were placed into 24-well plate, rinsed with 0.1 M PBS, and then incubated in 3% H2O2 in 50% ethanol (Junsei Chemical, Tokyo, Japan) for 10 min. Sections were then rinsed in PBS and incubated in blocking solution (10% normal goat serum in 0.1 M PBS), followed by incubation overnight with the primary anti-Fos antibody, raised in rabbit (1:5000; pc38, Calbiochem, San Diego, CA, USA), diluted in 2% normal goat serum, 0.2% triton in PBS (Vector, Burlingame, CA, USA). The next morning, sections were again washed in PBS and then incubated in the secondary antibody (biotinylated anti-rabbit, raised in goat; Invitrogen, Camarillo, CA, USA) diluted at 1:500 in 2% normal goat serum in PBS for 20 min, followed by further washes in PBS. Sections were then incubated with an ExtrAvidin–peroxidase (Sigma, St Louis, MO, USA) for 2 h before a further series of washes in PBS. Finally, the sections were incubated with 3,3’-diaminobenzidine tetrahydrochloride dihydrate containing nickel (DAB; Vector) before being washed and mounted on slides, air-dried, dehydrated, and mounted in distyrene plasticizer xylene (DBX) medium under a cover slip (Thermo scientific, Cheshire, WA, UK).
Omission of the primary or secondary antibody abolished the immunocytochemical staining completely, indicating specificity. Fos immunoreactivity was distinguishable by cellular location: the nucleus was always labeled an intense dark brown-to-black, indicating the Fos protein.
All sections were examined under an Olympus Universal microscope equipped with a digital camera (Olympus, Shinjuku, Tokyo, Japan) by two investigators blinded to the animal groups being assessed. Methods for assessing Fos protein-stained nuclei have been described previously (27). Briefly, for cells to be considered Fos-positive they had to be dark brown-to-black and round or ovoid, and they had to be visible under a light microscope at magnifications of 4×, 10×, and 20× objective plus a 10× eyepiece. Cytoarchitecturally identified regions of the superficial lamina of the TNC and of the upper cervical dorsal horn levels (C1–C3) of hemi-sections were examined for Fos-positive cells. The TNC was referenced to the obex according to coordinates provided by Paxinos and Franklin, and the cervical levels were determined based on the morphological appearance of the section under bright field illumination (28). At each level, four randomly selected sections were assessed, and an average of all cells per hemi-section for each level was calculated to investigate the distribution pattern at each nucleus without prior knowledge of the treatment of each animal. All counts were made by the same experimenters to maintain consistency in the application of criteria used to select Fos-positive cells and to reduce the likelihood of subjective variability.
Data analysis
Normally distributed data are reported as means (standard deviation), and data with unequal variances are reported as medians (interquartile range). The ANOVA test was used to assess differences between groups. Because quantitative measurements were made on an ordinal scale, statistical analyses were conducted using non-parametric statistics (29). Comparisons between treatment groups were made using the Kruskal–Wallis analysis of variance, and the Mann–Whitney U test was used for differences between groups. For multiple comparisons, the Bonferroni correction was applied. For Fos counting, Cronbach’s coefficient α was used to assess intra- and intra-observer reproducibility for counts made by the two independent investigators. All observations from investigators had an α coefficient >0.9 and thus values were pooled together. A probability of p < 0.05 at the two-tailed level was considered to indicate statistical significance. Analyses were performed using the SPSS software (version 16.0; SPSS, Chicago, IL, USA).
Results
Formalin-induced pain behavior
The control group was used to determine standard values for the early and late phases. Injection of formalin induced long-lasting face rubbing behavior that was characterized by two phases, as described previously (Figure 1). Memantine pretreatment attenuated formalin-induced pain behavior, though this was significant only in the late phase (p < 0.01; Figure 2).
Time course of face rubbing activity observed after formalin injection in each group. The mean number of seconds that rats spent rubbing is plotted for each 5-min block over the 60-min post-injection observation period. Comparisons of the early and late phases of formalin-induced face rubbing activity in each group. *p < 0.05, compared with the control group. **p < 0.05, compared with the formalin group.

Von Frey filament test
The VFMF thresholds are presented as proportional values to those of the contralateral site of the injected area. In the control group, the periorbital VFMF threshold ipsilateral to vehicle injection was not significantly different from the threshold contralateral to vehicle injection (df(2) = 710.4; p = 0.13).
The periorbital VFMF thresholds ipsilateral to the formalin-injected site decreased significantly 1 h and 2 h after formalin injection (df(2) = 6598.1; p < 0.01). In the memantine group, the periorbital VFMF thresholds were unchanged after formalin injection (df(2) = 529.2; p = 0.45; Figure 3).
Comparison of von Frey response thresholds at pretreatment and at 1 h and 2 h after formalin injection in each experimental group. *p < 0.05, compared with baseline.
FOS immunoreactivity
In both groups, Fos-positive neurons were located primarily within the superficial laminae of the TNC and laminae I and II of the C1–C3 levels.
There was a significant difference in the number of Fos-positive cells across the three groups (H(2) = 9.17; p = 0.01). The number of Fos-positive cells increased significantly following formalin injection versus the control group (p = 0.01). Memantine pretreatment significantly decreased the number of Fos-positive cells as compared with the formalin group (p = 0.009), and the number of positive cells was similar to that of the control group (p = 0.59).
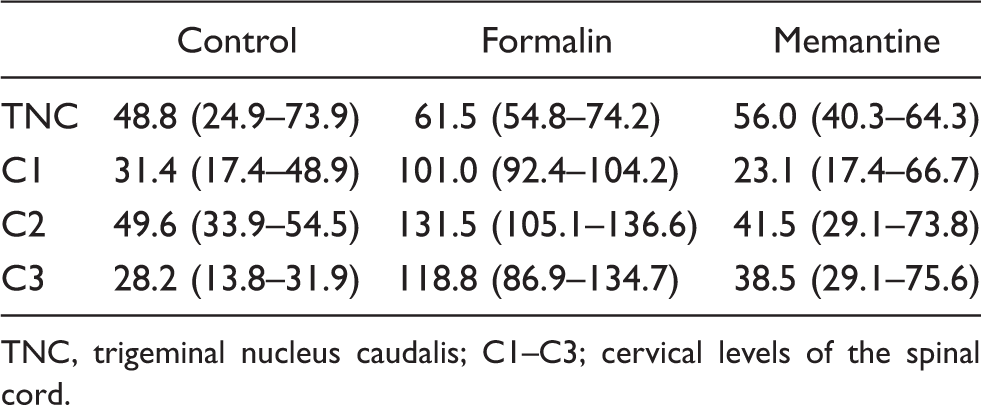
Data on the Fos-positive cells in each level of the TCC are presented in Table 1, and the distribution of Fos-positive cells in each experimental group is shown in Figure 4. The integrated counts of TCC for each group are presented in Figure 5.
Representative microphotographs of dorsal horn sections at the C2 level from each experimental group immunostained for Fos following formalin injection. Scale bars = 200 µm for all images. Comparisons of Fos-positive cells per animal in the trigeminocervical complex (TCC) in each treatment group. *p < 0.05, compared with the control. **p < 0.05, compared with the formalin group. The number of Fos-positive cells (25th – 75th percentile) per hemi-section per animal in each trigeminocervical region in each group TNC, trigeminal nucleus caudalis; C1–C3; cervical levels of the spinal cord.

Discussion
In contrast to most previous studies that injected formalin into the perioral area to induce orofacial pain, we used the periorbital area, which is a trigemino–ophthalmic-branch-innervated dermatome, to focus on headache pathophysiology. Unmyelinated C-fibers from the ophthalmic division of the trigeminal nerve are known to be important in the development of headaches (30,31). Electrophysiological studies showed that activated neurons of the trigeminocervical complex after stimulation of the superior sagittal sinus or the middle meningeal artery exactly corresponded to those of the TCC after cutaneous sensory stimulation to the periorbital area (32–34). In an experimental approach for evaluating migraine, the sensory threshold for pain/temperature at the ophthalmic dermatome was altered to assess trigeminovascular system sensitization (35,36). About two-thirds of migraine patients complain of hyperalgesia or allodynia at ophthalmic dermatomes, including in the forehead, which reflect central sensitization at the TCC (37). The presence of allodynia could be an important consideration for therapeutic limitations in migraine treatments (37,38). The distribution of Fos-positive neurons in the present study corresponded to the trigeminocervical complex proper, that is, the lower portion of TNC and C1-C3 cervical dorsal horn, and this was identical to the region that responds to stimulation of the perivascular nerve endings of the trigeminal nerve around the superior sagittal sinus or middle meningeal artery (32,39,40). The biphasic behavioral response to formalin injection is also comparable to those observed in orofacial formalin tests (18,41). Thus, the periorbital formalin injection model could be a useful tool for further experimental approaches to the pathogenesis of headaches.
We have demonstrated that the NMDA receptor antagonist memantine attenuated formalin-induced pain behavior, and the late phase seemed to be inhibited to a significant extent. After formalin injection, chemoreceptors are activated on the peripheral terminals of primary afferents to produce brief, phasic pain behavior in the early phase. During the late phase, which is the result of central sensitization of second-order neurons (19,42), glutamate is released, producing lasting, tonic nociceptive behavior (43,44). Interestingly, the temporal profiles of these biphasic responses approximately parallel those of peripheral nociceptors (45) and convergent neurons (3,46,47). Previous experimental approaches showed that NMDA receptors are involved in pain-related phenomena (18,48). Pain sensitization of dorsal horn neurons after peripheral inflammation-induced neuropathic pain is dependent on NMDA activity (49). Nociceptive behaviors are selectively enhanced by pretreatment with a NMDA agonist, but not with a 2-amino-3-(5-methyl-3-oxo-1,2- oxazol-4-yl)propanoic acid (AMPA) or a metabotropic receptor agonist (49). Development and expression of responses during the late phase are believed to be NMDA receptor-dependent (3), and NMDA agonists increase the nociceptive response only in the late phase following subcutaneous formalin injection into the hind paw (49). Memantine reduces nociceptive behavioral responses in chronic pain and neuropathic pain models, and this has been observed within therapeutically relevant dose ranges (16,19,25,50). In a study by Eisenberg et al., memantine blocked the formalin-induced late phase at dose levels substantially lower than those required for suppression of the early phase (19).
The results of the present study, which showed preferential inhibition of late phase formalin-induced pain behaviors by memantine, suggest that this drug might have useful effects for central sensitization of second order neurons in the pain transmission pathway rather than those involved in peripheral acceptance of pain signal inputs.
Because many NMDA receptor antagonists produce behavioral changes, such as hyperactivity and motor dysfunction, it is important to consider the possibility that the reduction in pain behavior may be due to a non-specific behavioral effect of memantine (51). Although the present study did not involve quantitative assessment of motor impairment, the exploratory and freezing behaviors displayed with memantine treatment were comparable to those in the vehicle-treated control group. Moreover, it has been consistently reported that the dose used in the present study (10 mg/kg) does not cause motor impairment (16,25,48). Indeed, memantine did not cause motor impairment at doses up to 20 mg/kg (48).
The present study showed that pretreatment with memantine attenuated formalin injection-induced c-Fos immunoreactivity in the TCC. Glutamate receptors are present in the superficial layer of the dorsal horn, especially in the C-fiber process and their central terminal (10) and lead to neuronal plasticity in the spinal cord, producing central pain sensitization (52,53). Glutamate antagonists reduce excitation in the spinal cord by primary afferent stimulation (53,54) and block wide dynamic neuronal firing in the spinal cord (53,55).
The NR2B subunits of NMDA receptors are localized predominantly in the superficial layer of the dorsal horn (56,57). These subunits are involved in central sensitization in the spinal cord (58). Several NR2B antagonists are currently being studied in different experimental models of nociception (59,60). Furthermore, a recent study has shown that selective knockdown of NR2B in the dorsal horn using short interfering RNA can suppress formalin-induced nociceptive behavior (61). The restricted distribution of NR2B receptors makes them promising candidates as targets for side-effect-free analgesics (62). Memantine has NMDA (NR2B) receptor-channel binding affinity (16). Memantine preferentially blocks excessive NMDA receptor activity without disrupting normal activity because it enters the receptor-associated ion channel preferentially when it is excessively open and, most importantly, its off rate is relatively fast, so it does not accumulate substantially in the channel to interfere with subsequent normal synaptic transmission (63).
Conclusion
After a formalin injection into a trigemino–ophthalmic-branch-innervated dermatome, the anti-nociceptive effect of memantine on pain behavior and Fos expression in the TCC had established. Similar to topiramate and divalproex sodium, which have negative modulatory effects on glutamate receptors, memantine could be a possible candidate for use in the preventative treatment of headaches (64).
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for profit sectors.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.