
Abstract
Background: Hemiplegic migraine (HM) is a rare subtype of migraine with aura that includes transient hemiparesis of different degrees. The dominantly inherited type, called familial hemiplegic migraine, along with the sporadic type, in which no family history of similar attacks exists, have been recently recognized by the revised International Classification of Headache Disorders (ICHD-2). Short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT) and short-lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms (SUNA) are also very rare conditions that are classified as trigeminal autonomic cephalalgias. This report provides the first description of an association between HM and SUNCT/SUNA.
Cases: Eight females and two males with both these disorders were identified between 2007 and 2010.
Conclusion: The coexistence of such rare primary headache disorders is probably due to a common underlining mechanism, with a sodium channelopathy being an attractive potential candidate.
Introduction
Hemiplegic migraine (HM) is a subtype of migraine with aura in which the characteristic aura component of the disorder consists of transient, unilateral motor weakness (1). It may occur sporadically (sporadic hemiplegic migraine, SHM) or be familial (familial hemiplegic migraine, FHM). Large families containing first degree relatives suffering from hemiplegic migraine have been characterized at a clinical and molecular level. Linkage studies have identified several mutations in three genes coding for neuronal trans-membrane ion channels. These include the alpha-1-A subunit of the voltage gated calcium channel in FMH1 (CACNA1A) (2), the 1-alpha-2 subunit of the Na+/K+ pump (ATP1A2) in FHM2 (3) and the 1-alpha subunit of the voltage gated sodium channel (SCN1A) in FHM3 (4). Although SHM was thought not to be associated with these mutations, a recent study reported a high proportion of de novo mutations of CACNA1A and ATP1A2, but not SCN1A, in early onset SHM (5).
SHM and FHM are rare conditions, with an estimated prevalence of 0.01% in the general population (6). However, the rate of hemiplegic symptoms in tertiary care centres seems to be higher and some of these motor symptoms do not always fit with the classical description of weakness in SHM (7). Young and colleagues described an entity of non-familial migraine with unilateral motor symptoms (MUMS) in a case-control study (8), differing in terms of character and duration of weakness and in its striking correlation with pain severity, from FHM and SHM. However, whether this represents a pathophysiologically distinct process from HM remains unclear, and the second edition of the International Classification of Headache Disorders (ICHD-2) does not recognize it as such (1).
The even rarer (9) primary headache syndromes of short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT) and short-lasting unilateral neuralgiform headache attacks with autonomic symptoms (SUNA) are trigeminal autonomic cephalalgias, characterized by repetitive short-lasting attacks of severe, unilateral, neuralgiform pain, usually experienced in the distribution of the ophthalmic and maxillary trigeminal divisions and associated with ipsilateral trigeminal autonomic phenomena (1).
This report presents the first description of a potential association between HM and SUNCT or SUNA by providing a case-series of ten individuals who have both conditions.
Methods
Following an initial observation that several patients attending our tertiary referral service suffered from both HM and SUNCT/SUNA, we reviewed the case notes of individuals assessed between 2007 and 2010, to identify patients diagnosed with both, according to ICHD-2 criteria. This search revealed that, out of a cohort of 117 SUNCT/SUNA and 107 HM patients currently under our care, ten patients met the ICHD-2 criteria for both HM and SUNCT, or alternatively the criteria for HM and those proposed for SUNA (ICHD-2, Appendix A3.3). These case notes were reviewed in detail and the demographics, clinical features and treatment histories of the patients were collected. Treatment response was considered significant when a reduction of 50% in severity or frequency was seen (either by reviewing patient diaries or by patient estimate of improvement at clinic).
Results
Demographics
Migraine characteristics of patients with co-existent hemiplegic migraine and SUNCT or SUNA

C, Contralateral; F, Female; FHM, Familial hemiplegic migraine; GBP, Gabapentin; I, Ipsilateral; LMG, Lamotrigine; Lt, Left; M, Male; Rt, Right; SHM, Sporadic hemiplegic migraine; SUNA, short-lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms; SUNCT, Short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing; TPM, Topiramate; VRS, Visual rating scale.
SUNCT/SUNA characteristics of patients with co-existent hemiplegic migraine and SUNCT or SUNA
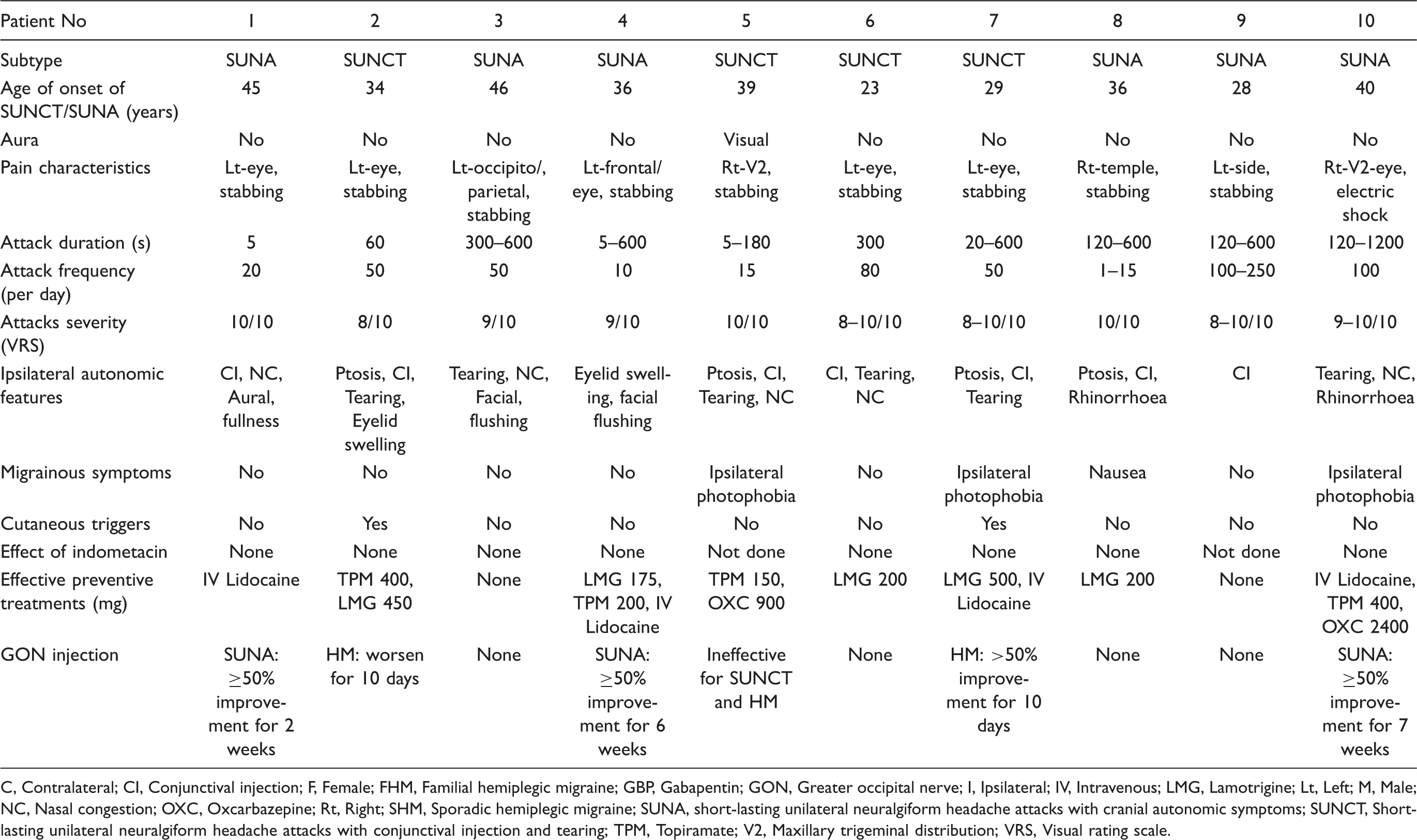
C, Contralateral; CI, Conjunctival injection; F, Female; FHM, Familial hemiplegic migraine; GBP, Gabapentin; GON, Greater occipital nerve; I, Ipsilateral; IV, Intravenous; LMG, Lamotrigine; Lt, Left; M, Male; NC, Nasal congestion; OXC, Oxcarbazepine; Rt, Right; SHM, Sporadic hemiplegic migraine; SUNA, short-lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms; SUNCT, Short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing; TPM, Topiramate; V2, Maxillary trigeminal distribution; VRS, Visual rating scale.
Migraine features
The HM was categorized as being sporadic (SHM) in all patients but one (patient 7), who fulfilled the ICHD-2 criteria for FHM. Six patients described the onset of at least two separate aura phenomena (visual, aphasic, sensory, motor or brainstem) prior to the onset of their headaches, while four patients described the aura phenomena developing during the headache exacerbations. Interestingly, half the patients had prolonged aura (especially motor) lasting longer than 24 hours. Four patients (patients 6–9) suffered from a constant daily background pain, described as a mild-moderate dull ache. In addition to this continuous pain, they experienced several exacerbations per month of more severe headaches, which fulfilled the diagnostic criteria for migraine attacks.
SUNCT/ SUNA features
Six patients fulfilled the diagnostic criteria for SUNA, while four fulfilled those for SUNCT. In four out of eight patients with unilateral migraine pain, the SUNCT/SUNA attacks were located on the same side. Attacks of both types of headaches occurred independently of each other in all cases. Three patients (5, 7 and 10) reported unilateral photophobia in the eye ipsilateral to the pain in association with their SUNCT/SUNA attacks and patient 8 described nausea accompanying most attacks.
Other co-morbid headache disorders
One patient also suffers from chronic cluster headache, with attacks occurring contralateral to the SUNA attacks, while two had a history of previous medication overuse headache, and had successfully undergone withdrawal.
Investigations
All patients underwent magnetic resonance imaging of the brain, which was normal except for patient 4, in whom it revealed a small cerebellar infarct, and patient 9, in whom it showed an area of right frontal cortical dysplasia. All but two patients were given a trial of indometacin to exclude paroxysmal hemicrania. One of the patients who were not given indometacin was profoundly allergic to non-steroidal anti-inflammatory drugs (NSAIDs). Indometacin did not have any effect on the short-lasting headaches.
Discussion
We describe the co-occurrence of HM and SUNCT or SUNA in a series of ten patients. Our current understanding suggests that these two conditions differ in terms of phenomenology, pathophysiology and the precise neuroanatomical pathways involved, but also that they share neurological pain mechanisms, namely the trigeminovascular system (10).
These disorders are rare. The estimated prevalence of sporadic HM is approximately 1 in 10,000 (6), while that of SUNCT/SUNA is 6.6 in 100,000 (9). Given the rarity of these headache syndromes, their co-existence in this series is unlikely to be a mere chance association. It seems likely that, in our tertiary practice, rare headache conditions and combinations of conditions will be over-represented. However, based on the available prevalence figures, the likelihood of coincidental occurrence of both disorders would be expected to be 6.6 per billion. Given that the population of UK is approximately 60 million, one might expect less than one case in the UK population. Referral bias therefore seems unlikely to be the sole explanation.
Alternative explanations include the possibility that the stated prevalence figures are underestimates. This is certainly possible: given that even common headache disorders are underdiagnosed, and the lack of large population-based data on the prevalence of rarer disorders, it is possible that SUNCT/SUNA or hemiplegic aura is commoner than has been appreciated.
It may also be the case that migraine, particularly chronic migraine with frequent or continuous pain, may amplify or even ‘unmask’ coexistent pain syndromes, leading the latter to be over-represented in the migraine population and vice versa (11). However, the salient feature of patients in this series was the presence of hemiplegic aura rather than merely chronic pain or central sensitization, raising the possibility that there is something more specific about aura in these patients that may be linked to a higher expression of the SUNCT/SUNA phenotype.
This association raises the possibility of a common denominator implicated in the pathogenesis of both conditions, with ion channel dysfunction being an attractive hypothesis. It is noteworthy that the most effective treatments of SUNCT/SUNA (lamotrigine, topiramate, as well as oxcarbazepine in our experience) modulate sodium channel function among others, and that sodium channel dysfunction is capable (at least in FHM series) of generating hemiplegic aura. Sequencing of sodium channel genes in these individuals may provide additional insight into the pathophysiology of SUNCT/SUNA as well as HM.
We recommend specifically asking patients presenting with either headache phenotype whether or not they suffer with different types of headaches, and particularly ask about unilateral stabbing headaches associated with cranial autonomic features in patients who present with hemiplegic migraine. These patients may represent an important subgroup worthy of further clinical and molecular characterization.
Footnotes
Funding
This work was undertaken at UCL/UCLH and was funded in part by the Department of Health NIHR Biomedical Research Centres funding scheme.
Competing interests
There are no competing interests. AN, GL and PS have no disclosures. MSM serves on the advisory board for Allergan and St Jude Medical, and has received payment for the development of educational presentations from Allergan, Merck Sharpe and Dohme Ltd and Medtronic.