
Abstract
Background
Hemiplegic migraine is a rare form of migraine with aura characterized by motor aura. Although auras in hemiplegic migraine are typically complex with two or more aura symptoms, neglect has been rarely described.
Case report
We report the case of a 20-year-old woman with sporadic hemiplegic migraine that was investigated for the presence of unilateral spatial neglect (USN) during aura in one of her migraine attacks. Transient hemispatial neglect was observed during a right-sided migraine attack with left sensory-motor hemisyndrome; after migraine resolution there was a total recovery.
Conclusions
Our case demonstrates that USN may be a symptom of aura. To our knowledge, this is the first report of USN during aura in an adult with sporadic hemiplegic migraine.
Keywords
Background
Hemiplegic migraine is a rare form of migraine with aura that is characterized by the presence of aura with motor symptoms (1). Although during aura in these patients could be present sensory, aphasic and basilar-type symptoms (2), associated with the motor involvement (1), the presence of unilateral neglect has been reported, to our knowledge, in only one case in childhood (3). We describe the first case in an adult woman with sporadic hemiplegic migraine.
Case report
The patient is a right-handed 20-year-old woman affected by migraine with typical visual aura since the age of 15 (two migraine attacks/month). In her familial history we found that her mother suffers from migraine without aura.
In May 2006 she experienced three migraine attacks with unilateral sensory and motor involvement that fulfilled the International Classification of Headache Disorders II (ICHD II) criteria for sporadic hemiplegic migraine (SHM). She was admitted to our neurological unit during the third episode.
In the first episode, nine days prior to her current presentation, she suffered from paresthesias involving the right hemisoma (begun from the right leg and ascending to the homolateral hemiface), associated with right hemiparesis and aphasia, followed after two hours by left-sided pulsatile headache. During the attack the patient presented drowsiness. Focal symptoms lasted for 12 hours, and after there was a complete recovery.
Two days after a similar episode occurred, characterized by right-sided sensory-motor hemisyndrome for 30 minutes, followed by pulsating headache that lasted for two hours.
Six days after, she was admitted to our neurological unit because she complained of scintillating scotoma for a few minutes in the right visual field, followed by tingling paresthesias at left hemisoma, mild left hemiparesis with hand pronation. Simultaneously she presented moderate right-sided pulsating headache. During the attack, basilar-type symptoms (except mild dysarthria) and campimetric deficits were absent. She had only mild difficulty in concentration, but was lucid and well oriented in time and space. Motor and sensitive symptoms lasted for four hours while headache persisted for 14 hours. Five hundred mg of paracetamol and seven drops of delorazepam were administered.
Brain computed tomography (CT), brain magnetic resonance imaging (MRI) and angio-MRI, electrocardiogram, cardiologic examination, supra-aortic trunks ecocolordoppler, thyroid hormones and other blood exams, performed the day of this migraine attack, were normal.
An electroencephalography (EEG) showed slow waves on the right side, without any epileptic discharge.
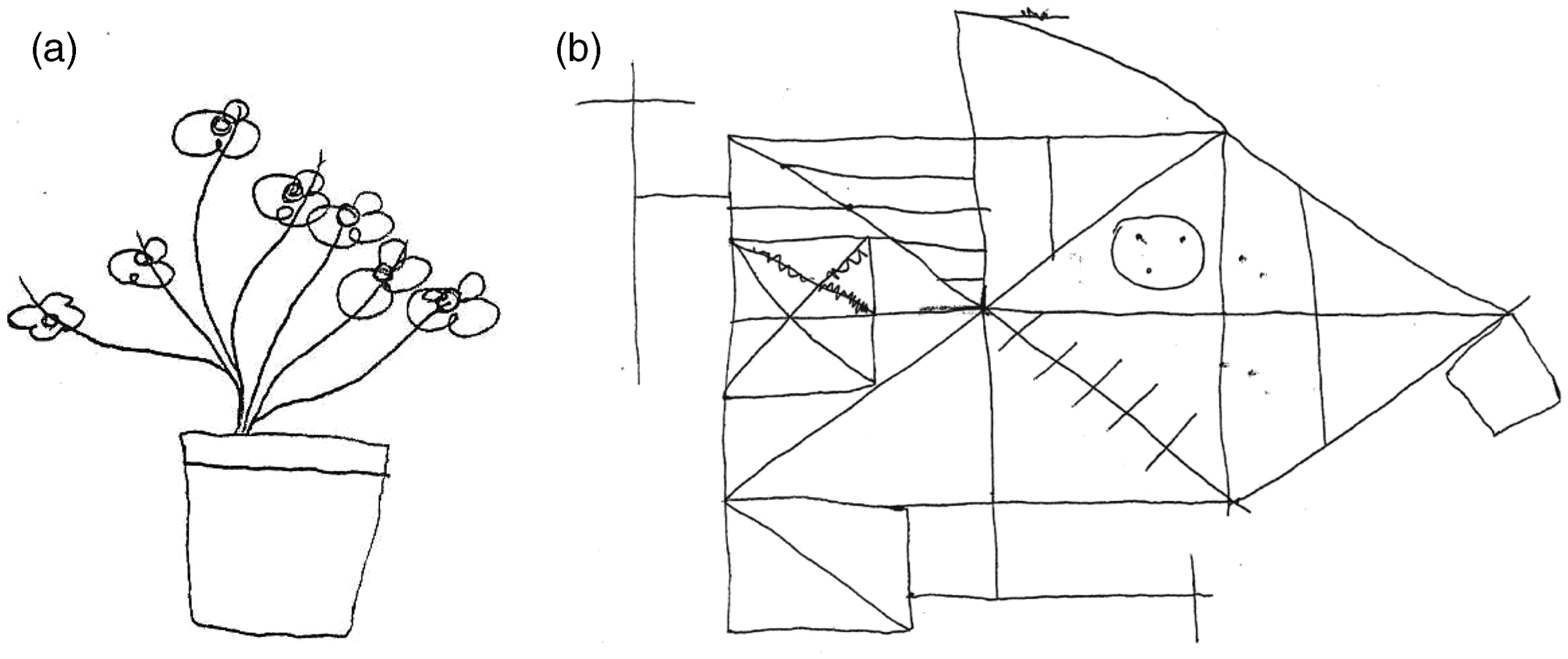
Although during aura there was no evidence of right hemisphere cognitive dysfunction, neglect tests were administered (Figure 1), and left unilateral spatial neglect (USN) was observed both in spontaneous drawing and copying of simple and complex figures (Figure 1(a–c)). Neuropsychological examination performed after the resolution of the neurological symptoms demonstrated the absence of neglect (Figure 2).
Drawing tests during migraine attack. Paper and copying models were put in the center of the patient’s middle sagittal plain. Figure 1(a) and 1(b) are spontaneous drawing tests; 1(c) is a direct copy from the template. Both in copying and spontaneous drawing tests, the left part of the figures are less detailed and defined than the right side. In (a) part of the numbers on the left side of the clock are drawn on the right side. Of note, the drawing was made on the right side of the paper. In (b) note the omission of petals on the left side. In (c) Rey complex figure copy, the left part is not defined. Spontaneous drawing (2(a)) and Rey complex figure copy (2(b)) after the remission of neurological symptoms. No neglect was observed.
Discussion
Our patient fulfills the ICHD II criteria for the diagnosis of SHM (4). In two migraine attacks, during aura, unilateral motor and sensory involvement on the right side were observed; in one of them, aphasia was present. During aura in the last episode, neurological focal signs and symptoms were left sided and transient extrapersonal neglect was observed. Personal motor and sensory neglect were not present at the clinical evaluation. Visual field deficit or other cognitive problems that could explain this neuropsychological disorder were excluded. Confrontational visual fields were full during the spatial neglect testing. Of note, a minor visual problem, not documented in the clinical examination, cannot explain the difficulties of the patient both in spontaneous drawing and copying from the template and the best definition of the right side of the figures.
Pharmacological therapies were administered after the tests.
Although neuropsychological abnormalities during migraine aura have been documented, as demonstrated by the frequent association with aphasia, right hemisphere dysfunction has been rarely described and USN is not described as a typical feature of aura.
In the familial hemiplegic migraine (FHM) literature, some authors analyzed retrospectively symptoms reported during migraine attacks by FHM patients (5–8); some of these would be consistent with neglect syndromes. In particular Rosenbaum (5) described an 18-year-old male with an episode characterized by left-right disorientation and denial of the entire right side. O’Hare et al. (7) reported the cases of two members of a family with FHM who experienced disturbances in the right visual field where objects appeared distorted in size and outline. Gardner et al. (8) reported during aura the presence of an alien hand syndrome in three women with FHM; in one of these was clearly described the presence of personal neglect.
Enoki et al. in 2006 described a 13-year-old girl showing USN during an attack of hemiplegic migraine (3); they hypothesize that left spatial neglect may be attributed to the cortical hypoperfusion that is developed transiently on the right hemisphere.
Also in our case, neglect was observed during right hemisphere dysfunction and was present during aura.
The reason why there are so few reports of neglect during aura could be different; it is possible that such a symptom is not clinically as evident as other neurological deficits and usually not recorded in headache patients’ diaries. Furthermore, neglect and in general right hemisphere deficits are more often associated with anosognosia (9); of note, our patient was not aware of her problem. Moreover, aura is usually reversible and of short duration, and neglect may be overlooked if the clinician doesn’t search for it during the acute stage. We don’t know if neglect is a rare symptom present only during long-lasting auras as occur in sporadic hemiplegic migraine or, if properly investigated, whether they could also be found during other forms of migraine with aura.
Conclusions
To our knowledge this is the first case of neglect during SHM in adulthood. We believe it’s interesting because it extends the semiology of aura in SHM and the possible causes of neglect. What we observed should be evaluated in a larger cohort of patients with SHM and other forms of migraine with aura, to better understand if this aura symptom is specific or not for SHM.
Clinical implications
First description of neglect during aura in an adult patient with sporadic hemiplegic migraine. Broadening aura’s phenotype and causes of transient neglect.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.