
Abstract
Background: Anecdotal reports and a single case-control epidemiological survey have suggested an association between the helminthic disease neurocysticercosis and primary headache. The present study was undertaken to determine whether neurocysticercosis is more common among patients with primary headaches than in other neurological disorders.
Methods: We determined the prevalence of neurocysticercosis in a cohort of patients with primary headache who were seen at our institution over a 20-year period. We used as controls all people from the same cohort with four major different categories of neurological disorders, including cerebrovascular disease, degenerative disorders of the CNS, head trauma, and primary brain tumors. We evaluated differences in the prevalence of neurocysticercosis between patients and controls.
Results: Forty-eight of 1017 patients with primary headache and 31 of 1687 controls had neurocysticercosis (4.7% vs 1.8%, p < 0.0001). Calcified parenchymal brain cysticerci were more frequent among patients with primary headache than in those with cerebrovascular disease (4.7% vs 1%, p < 0.001), degenerative disorders of the CNS (4.7% vs 2.4%, p < 0.05), and head trauma (4.7% vs 2.3%, p < 0.05). There were no significant differences, however, for the subset of controls with primary brain tumors (4.7% vs 3.5%), a condition that has also been associated with neurocysticercosis.
Conclusions: There is a relationship between calcified neurocysticercosis and primary headache disorders. It is possible that periodic remodeling of cysticercotic calcifications, with liberation of antigens to the brain parenchyma, contributes to the occurrence of headache in these patients.
Introduction
Neurocysticercosis is a pleomorphic helminthic disease affecting thousands of people all over the world (1). It is most often associated with seizures, although a number of patients present with focal neurological deficits, cognitive impairment, or headache. The latter usually occur in the setting of increased intracranial pressure in patients with multiple parenchymal brain cystic lesions, or in those with hydrocephalus or giant subarachnoid cysts (2).
The occurrence of neurocysticercosis among patients with primary headaches (migraine or tension-type headache) has been noted in anecdotal case reports (3) and in a single case-control epidemiological study (4). This association, however, has been considered as fortuitous by others, who did not find a pathophysiological rational basis to explain the development of chronic headache as the result of parenchymal brain calcifications or a single granuloma (5). We conducted a study in a large cohort of patients to determine whether neurocysticercosis is associated with the occurrence of ‘primary headache disorders’ and to discuss the possible explanations to this association.
Methods
From a cohort of 7519 consecutive adults attending the outpatient neurologic clinic of Hospital-Clinica Kennedy (Guayaquil, Ecuador) from January 1990 to December 2009, a total of 1820 patients met ICHD-II criteria for diagnosis of primary headache (6). For the purposes of the study, we only included the 1017 individuals with primary headache who were evaluated with computed tomography (CT) (case patients). We used as controls all people from the same cohort with four major different categories of neurological disorders who were studied with CT. They consisted of a total of 1687 patients with stroke, degenerative diseases of the CNS, head trauma, and primary brain tumors. Neuroimaging studies were analysed in both patients and controls, with attention to the presence of lesions characteristic of neurocysticercosis (7,8). Ethical aspects of the investigation and confidentiality of the names of the patients included in this cohort were assured by the institutional review board. The χ2 test was used to assess the significance of the difference in the prevalence of neurocysticercosis between patients and controls. Differences were considered significant if p < 0.05. Statistical analysis of data was carried out using EpiInfo-2000 software (Centers for Disease Control, Atlanta, GA).
Results
The 1017 patients with primary headache were 280 men and 737 women with a mean age of 38.8 ± 15 years (age range 18 to 94 years). Three-hundred-and-ninety-three patients (38.6%) had migraine, 311 (30.6%) had tension-type headache, 243 (23.9%) had a combination of migraine and tension-type headache, and the remaining 70 (6.9%) had other primary headaches (cluster headache, paroxysmal hemicrania, headache associated with exercise or sexual activity, thunderclap headache, hemicrania continua, and cough headache).
Characteristics of case patients and controls included in this study
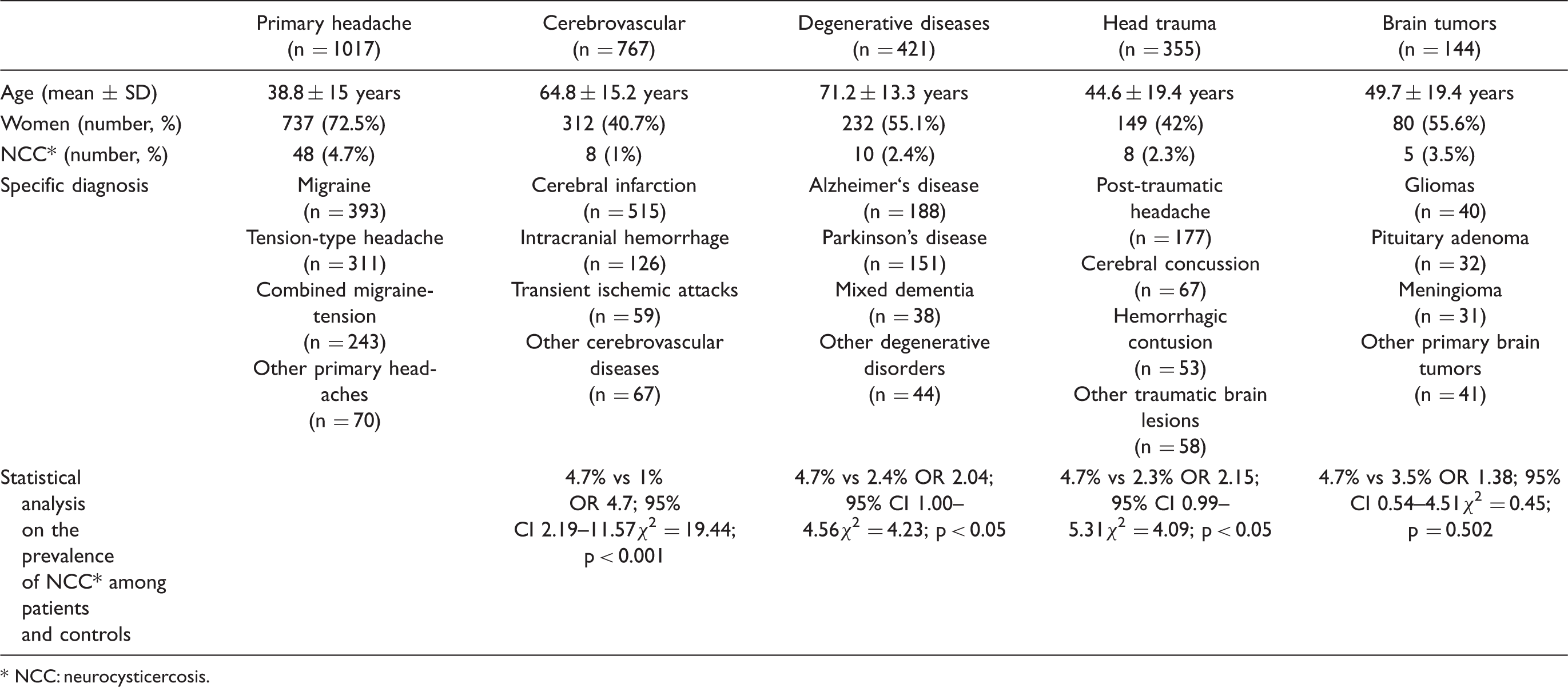
NCC: neurocysticercosis.
Forty-eight of the 1017 patients (4.7%) had parenchymal brain calcifications on CT scans of the head. Thirty-two patients had a single calcification, nine had 2–5 calcifications, and seven had multiple calcifications evenly distributed throughout the brain parenchyma. There were no significant differences in age, gender, or headache type among patients with and without neurocysticercosis. Eighteen of the 48 patients (37.5%) with headache and neurocysticercosis had migraine, 18 (37.5%) had tension-type headache, 11 (23%) had a combination of migraine and tension-type headache, and a single patient (2%) had hemicrania continua.
Thirty-one of the 1687 controls (1.8%) had neurocysticercosis, which appeared in the form of single or multiple parenchymal brain calcifications in all but one stroke patient who had a small cyst in the lateral ventricle. When analysed separately, we found neurocysticercosis in eight of 767 stroke patients (1%), in ten of 421 patients (2.4%) with degenerative diseases of the CNS, in eight of 355 patients (2.3%) with head trauma, and five of 144 patients (3.5%) with primary brain tumors.
As a whole, more case patients than controls had neurocysticercosis (4.7% vs 1.8%; OR 2.65, 95% CI 1.64–4.33; χ2 = 18.58, p < 0.0001). When the prevalence of neurocysticercosis was compared separately between patients and the different control groups (Table 1), we also found a significantly higher number of cases of neurocysticercosis among patients with primary headache than in controls with stroke (4.7% vs 1%; p < 0.001), with degenerative disorders of the CNS (4.7% vs 2.4%; p < 0.05), and with head trauma (4.7% vs 2.3%; p < 0.05). The only exception was a non-significant difference in the prevalence of neurocysticercosis among patients with primary headache and primary brain tumors (4.7% vs 3.5%).
Discussion
Despite the high prevalence of primary headaches and neurocysticercosis in the general population, it is surprising how scarce available information is about a possible association between these two conditions. Besides a handful of anecdotal case reports and small series showing a possible link between primary headache and neurocysticercosis (3,5,9,10), a case-control study from a small rural village in Ecuador suggested an association between neurocysticercosis and migraine (4). In that study, 57 migraine sufferers and 109 healthy controls underwent CT of the head, which showed neurocysticercosis in 19 of the 57 patients with migraine and in 14 of the 109 controls (33.3% vs 12.8%; p < 0.001). Fifteen of the 19 patients with migraine and neurocysticercosis had parenchymal brain calcifications as the sole evidence of the disease. This extremely high prevalence of neurocysticercosis among migraine sufferers could be due to selection bias. Using a field instrument, the authors detected 187 patients with migraine and all were then invited to have a CT scan. It could be argued that only those with more severe headache or with additional complaints accepted the inconvenience of transportation to a city that is more than 100 km away. Moreover, a positive case-control study is suggestive of association and not of causality. Despite these caveats, this is the only study stressing a relationship between primary headache and neurocysticercosis (4).
Differences in the demographic profile between our patients with primary headaches, that is, younger and with a higher percentage of women, were expected findings given the nature of neurological diseases of patients used as controls.
Our cohort strongly suggests an association between primary headache and calcified parenchymal brain cysticercosis. We found a statistically significant increased number of individuals with neurocysticercosis among case patients than in controls (p < 0.0001). The global odds ratio of 2.65 is our best estimate of this relationship, and the 95% confidence interval of 1.64–4.33 was consistent with the data suggesting that this parasitic disease may be associated with the occurrence of primary headache. The only exception was the similar prevalence of neurocysticercosis among case patients and the subset of controls with brain tumors. As previously noted, a link has also been found between neurocysticercosis and brain tumors, related to a combination of pathogenetic mechanisms that included a cell-mediated parasite-induced immunosuppression associated with an intense astrocytic proliferation that may surround some calcified cysticerci (11,12).
In our patients, it is clear that headaches were not the consequence of increased intracranial pressure. So, if we assume that our results were more than merely a chance association, we need to hypothesize a possible rational pathogenetic mechanism to explain the occurrence of headache in patients with parenchymal brain calcifications. Recent evidence has changed previous ideas regarding calcified parenchymal brain cysticerci as totally inert lesions. Calcifications, once considered inactive, may experience periodic morphological changes related to a mechanism of remodeling. This may expose parasitic antigenic material to the host, causing transient inflammatory changes in the brain parenchyma that may be the cause of seizures or focal neurological deficits in some patients (13,14). That such exposure may also cause transient and recurrent headache episodes mimicking a primary headache disorder is a plausible explanation, providing a rationale for the occurrence of headache in patients with calcified neurocysticercosis. In countries endemic for neurocysticercosis, routine practice of CT in people with headache may allow the detection of parenchymal brain calcifications that may be responsible for the occurrence of headache. This recommendation is also valid for immigrants moving from disease-endemic to non-endemic areas. Indeed, there are some recent reports of immigrants, living in Western European countries, who have presented with a ‘primary headache’ disorder, and in whom neuroimaging studies have revealed neurocysticercosis (15–18).
Footnotes
Author contributions
OHDB designed the study and drafted the manuscript; VJDB designed the study and analysed the data.
Conflict of interest
Nothing to disclose.