
Abstract
Introduction
In this report we describe a series of patients with a previously undescribed headache.
Methods
Over a 4-year period, we recruited 14 patients with a distinctive type of head pain of unknown cause that did not meet diagnostic criteria for other primary headaches.
Results
Nine women and five men with a mean age of 49.6 years (standard deviation, 17.8) presented with spontaneous headache attacks lasting 2–15 minutes. In each attack, the pain was localized to a region of one side of the head. Pain location varied between episodes in 12 patients. Pain quality was pressing, and pain intensity was mild to severe. There were no accompanying symptoms. Physical examination and all ancillary tests were unremarkable. Among seven patients who tried pharmacological treatments, one responded to antidepressants, another to indomethacin and three to other nonsteroidal anti-inflammatory drugs or simple analgesics.
Conclusions
Paroxysmal pressing headache may be a new headache syndrome marked by short duration of the pain and shifting location.
Introduction
Primary headaches are descriptive syndromes that have arisen from observations made by physicians in their patients (1). Among a myriad of patients diagnosed with already known headaches, at times one encounters patients with unexpected clinical features, and wonders whether such an observation is a variant of an acknowledged condition or if one is facing a new syndrome. Nevertheless, if more patients with the same novel clinical picture are observed, consistency is added to the initial observations and a hypothetical new syndrome begins to be considered (2).
In the last 4 years, we have seen some patients with a distinct headache whose clinical features did not fit any of the conditions currently classified in the International Classification of Headache Disorders, 3rd edition (ICHD-3) (1). Essentially, our patients suffered from spontaneous attacks of pressing headache lasting minutes that affected one region of either side of the head and could have shifting locations between episodes. This clinical picture was reminiscent of tension-type headache (TTH) regarding both the quality of the pain and the lack of accompaniments. However, its spatial and temporal features were not consistent with TTH or any other headache syndrome described to date.
Initially, we adopted a conservative position and considered that our patients had an atypical or unclassifiable headache. However, when dealing with successive patients with very similar complaints, we began to develop the feeling that their clinical picture was not only consistent but that it was to be distinguished from other headaches. Once a considerable number of patients were collected, we aimed to describe a distinctive type of headache with possible nosological boundaries. We propose that it is likely to be a new syndrome that we have termed paroxysmal pressing headache (PPH). Alternatively, this clinical picture could eventually be considered as a particular variant of TTH or other primary headache.
Methods
Over a 4-year period, we prospectively identified 14 patients who experienced a paroxysmal unilateral headache of pressing quality that did not meet current diagnostic criteria for migraine, TTH, trigeminal autonomic cephalalgias (TACs) or other primary headaches. All of them were recruited as outpatients at the Neurology Departments of three University hospitals (Hospital Universitario Fundación Alcorcón, Hospital Universitario Quironsalud Madrid, and Hospital Clínico San Carlos, Madrid, Spain) by three of the authors (JAP, TL, MLC).
Baseline demographic data, personal and family medical history, and a detailed description of the symptoms were obtained in a systematic way. The patients were asked about the location, quality, intensity – mild, moderate or severe – and temporal pattern of the pain, as well as potential triggers and aggravating or alleviating factors. In addition, all patients were specifically asked about the presence of nausea, photo- and phonophobia, trigeminal autonomic symptoms, restlessness or agitation, or any pain accompaniments. Previous treatments tested by the patients were recorded, together with their effects. Other past or concomitant headaches were also assessed, and their diagnoses were based on the ICHD-3 criteria (1).
A comprehensive physical and neurological exam was performed in all patients, including palpation of the temporal arteries, the pericranial nerves and the cranio-cervical muscles. The temporomandibular joints and the cervical spine were also tested for active and passive mobility and localized tenderness. Their psychological status was assessed using the Beck Depression Inventory, 2nd edition (BDI-II) (3), and the State-Trait Anxiety Inventory (STAI) (4). Underlying diseases were consistently excluded by routine blood work-up, including erythrocyte sedimentation rate, C-reactive protein and immunological screening, and neuroimaging studies, including magnetic resonance imaging of the head and magnetic resonance angiography.
The follow-up period ranged from 4 months to 2 years and 7 months. Throughout this time, the evolution of the headache and the treatments used were documented at intervals of 1 to 6 months. All clinical data were recorded in the hospital charts and were eventually confirmed through personal contact with the patients by one of the authors (JAP, AC, MA or MLC). All patients gave informed consent to be included in this report.
Results
Demographic and clinical features of this series of patients with paroxysmal pressing headache.

Intensity: + , mild; + +, moderate; + ++, severe.
F: female; Fr: frontal; GON: greater occipital nerve; L: left; M: male; NSAIDs: nonsteroidal anti-inflammatory drugs; O: occipital; P: parietal; R: right; T: temporal.
All 14 patients reported episodes of pressing pain of sudden onset lasting a few minutes (range, 2–15 minutes; see Table 1). The localization of the pain was variable but was typically focused in one region of one hemicranium, with ill-defined borders. Any region of the head (frontal, temporal, parietal, or occipital) could be affected. Two patients had fixed locations, but 12 patients had locations that changed from one episode to another. Three patients had side-locked headaches (right, n = 2; left, n = 1), while the remaining 11 patients had shifting sides (right or left). Pain quality was consistently pressing, but pain intensity could be mild (n = 3), moderate (n = 4) or severe (n = 7). The pain was not increased by physical activity, and there were no other accompanying symptoms. Between the episodes, all patients remained asymptomatic. The frequency varied between the different patients, and also within the same patient, ranging from one attack per month to 30 attacks per day. Headache attacks occurred spontaneously, without specific precipitating mechanisms. Nevertheless, four patients recognized that psychological stress could aggravate the symptoms, and one patient related some of her attacks to menstruation. This last patient got rid of the symptoms when she became pregnant. Four patients reported a past history of migraine and one patient had a history of TTH, but their new pain was not temporally related to the other headaches. Otherwise, seven patients reported a family history of headaches among first-degree relatives.
Upon examination, neither skin changes nor sensory abnormalities were noted in the painful zones. Moreover, palpation of the temporal arteries, the pericranial nerves and the cranio-cervical muscles did not evoke any abnormal sensation. General and neurological exams, BDI-II and STAI scores, and the results of all ancillary studies were otherwise normal in all patients.
Seven patients tested pharmacological treatments, and a therapeutic response was obtained in five (Table 1). One of them had pain relief with simple analgesics (metamizole), and three obtained symptomatic relief with nonsteroidal anti-inflammatory drugs (NSAIDs); one of these patients did not respond to ibuprofen but became asymptomatic on indomethacin 25 mg t.i.d. Another patient responded completely to amitriptyline 10 mg daily; this last patient had to stop amitriptyline due to an adverse reaction (i.e. micturition disturbance) but ended up responding to duloxetine 60 mg daily. On the other hand, some therapeutic failures were registered with paracetamol, NSAIDs, amitriptyline, pregabalin and occipital nerve blocks.
In the long term, five patients eventually experienced spontaneous remissions after a symptomatic period of between 8 months and 3 years and 8 months. Three patients had a remitting and relapsing course, with symptomatic periods lasting 1 to 4 months alternating with remissions lasting several months. The remaining six patients continued to have headache attacks throughout the follow-up (Table 1).
Discussion
Proposed diagnostic criteria for paroxysmal pressing headache.
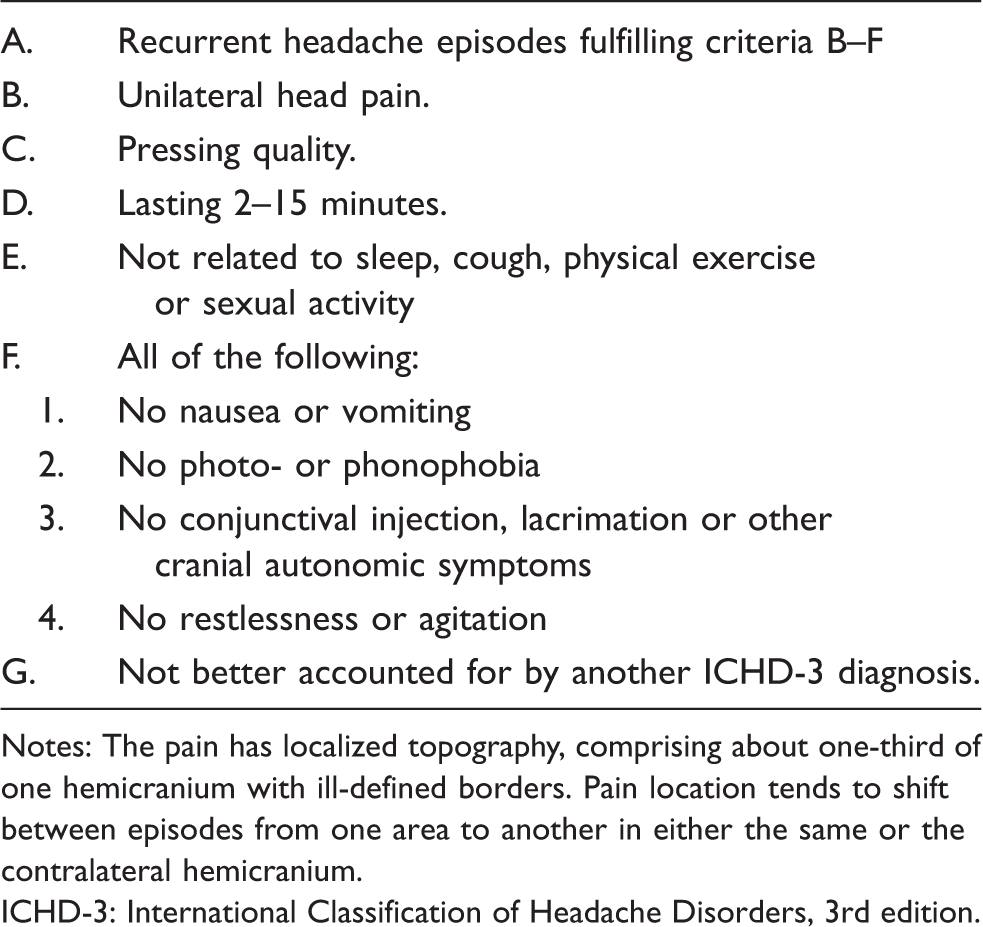
Notes: The pain has localized topography, comprising about one-third of one hemicranium with ill-defined borders. Pain location tends to shift between episodes from one area to another in either the same or the contralateral hemicranium.
ICHD-3: International Classification of Headache Disorders, 3rd edition.
The clinical picture of PPH should be distinguished from other well-recognized headaches (1). Specifically, it must be distinguished from short-lasting headache syndromes such as primary stabbing headache, SUNCT and SUNA, paroxysmal hemicrania, cluster headache, hypnic headache, and primary headaches induced by cough, physical exercise or sex (5).
Like PPH, primary stabbing headache is characterized by localized paroxysms of pain occurring spontaneously that may also change locations. However, the pain in primary stabbing headache is felt like a stab in a point-sized area, and each stab lasts for up to a few seconds (1,6). TACs are characterized by unilateral, orbital/periorbital headache attacks that are typically accompanied by a variable combination of autonomic features including conjunctival injection, lacrimation, nasal stuffiness, and rhinorrhoea (1,7). Both the lack of autonomic features and the multifocal localization clearly differentiate PPH from the TACs. Hypnic headache is characterized by recurring headache attacks lasting from 15 minutes up to 4 hours without characteristic associated symptoms (1,8). The main difference with PPH is that the attacks develop only during sleep, causing awakening. Primary cough, exercise and sexual headaches have sudden onset and may also have short duration. Nevertheless, these headaches are strictly dependent on the provocative factor and do not exist if the precipitating mechanisms are avoided (1,9).
In addition to the above-mentioned syndromes, PPH must be differentiated from other primary headaches including migraine, TTH and nummular headache.
PPH attacks may resemble those of migraine in terms of their hemicranial location. However, migraine attacks are normally more diffuse and often acquire a pulsatile quality. Moreover, migraine headaches commonly have a gradual onset and, if untreated, they last 4–72 hours. Otherwise, migraine headache is typically accompanied by photophobia and phonophobia, nausea and/or vomiting (1,10). Those migrainous features are not met in PPH.
PPH may also resemble TTH due to the pressing quality of the pain and the lack of accompanying symptoms. Unlike PPH, TTH typically acquires a diffuse and bilateral distribution. On the other hand, TTH usually develops gradually during or after recognizable stress, lasting from 30 minutes to 7 days (1,10). Upon examination, most patients with TTH exhibit both tender points and trigger points in the cranio-cervical muscles (11). It is true that our patients could be diagnosed with “probable TTH” according to the ICHD3 criteria, particularly those having mild or moderate pain. However, two of the essential features of the pain in our patients (i.e. the location of the pain and its duration) differed from those characteristic of TTH.
Finally, the differential diagnosis of PPH should include nummular headache. Indeed, the focal distribution of the pain is a common feature to both types of headache. Although nummular headache pain is mostly continuous, some patients have intermittent pain. There are also bifocal and multifocal cases in which the pain occurs in different areas of the head. Nevertheless, the pain of nummular headache is felt in a round or oval sharply-contoured area, generally 1–6 cm in diameter (1,12).
Presently, we do not have much data regarding the therapeutic options for PPH. Simple analgesics and NSAIDs were effective in some patients, but some other patients who tried them did not find any effect. A patient with multiple therapeutic failures had an absolute response to indomethacin; if this type of response is confirmed in other patients, PPH might eventually be included among the indomethacin-sensitive headaches. Finally, a patient responded to antidepressants; even though they are non-specific drugs, this could be a common feature with TTH or migraine.
In conclusion, our preliminary data indicate that PPH is a clear-cut clinical picture that may be distinguished from other similar headaches. PPH might be a variant of other headaches but might also represent a new syndrome. Since no underlying etiology has been found, PPH may be considered a primary headache. Further descriptions are needed to validate our observations.
Footnotes
Clinical implications
Fourteen cases of a previously undescribed headache are reported.
Paroxysmal pressing headache is characterized by sudden paroxysms of pain occurring spontaneously and lasting up to a few minutes.
The pain is typically pressing and is localized to a limited area of the head.
Pain location tends to shift between episodes from one area to another in either the same or the contralateral hemicranium.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.