
Abstract
Morning headache is accepted as part of clinical findings of obstructive sleep apnoea syndrome (OSAS). The prevalence of morning headache is at variable levels from 18% to 74% in patients with OSAS. However, there is controversy over the association of morning headache and OSAS. We studied morning headache prevalance and characteristics in 101 controls with apnoea-hypnoea index (AHI) < 5 and 462 OSAS patients with AHI ≥ 5. Morning headache was reported by only nine (8.9%) subjects in a control group compared with 156 (33.6%) of OSAS patients (P < 0.01). Morning headache prevalance was significantly higher in severe and moderate OSAS groups. AHI was significantly higher in OSAS patients with morning headache compared with patients without morning headaches. Oxygen saturation nadir during rapid eye movement and non-rapid eye movement sleep as well as mean oxygen saturation value during total sleep time were also found to be significantly lower in morning headache group. However, none of the sleep parameters was found to be determinants of morning headache. Morning headache was more frequently reported by patients of female gender and with primary headache history. Morning headache was totally resolved in 90% of patients treated with nasal continuous positive airway pressure. The history of OSAS should be considered in the differential diagnosis of morning headache.
Introduction
Obstructive sleep apnoea syndrome (OSAS) has been recognized as an important health problem with high morbidity, with approximately one in every five adults having at least mild OSAS and one of every 15 at least moderate OSAS (1). OSAS is characterized by repetitive episodes of upper airway obstruction that occur during sleep, usually associated with reduction in blood oxygen saturation. In patients with OSAS, various symptoms including snoring, nocturia, nocturnal sweating, daytime sleepiness and/or fatigue, intellectual deficiency, sexual impotence and even insomnia are reported. Recently, headache, especially morning headache, has been suggested as part of the clinical findings of OSAS. Furthermore, morning headache in relation to OSAS was included in the International Classification of Headache Disorders under the heading of sleep apnoea headache (2).
The prevalence of morning headache has been shown to be 5–7% in the general population (3, 4), whereas it has been reported at variable levels from 18% to 74% in patients with OSAS (3, 5). On the other hand, 12–41.7% of patients with nocturnal or morning headache have been shown to have OSAS by polysomnographic (PSG) evaluation (6, 7). Disappearence of headache when OSAS was treated supports the causal role of OSAS in morning headache. However, other studies have denied this relationship (8, 9).
The mechanisms by which OSAS causes morning headache have not been definitively identified. Hypoxia, hypercapnia, disturbance of cerebral blood flow autoregulation, transient increases in intracranial pressure and sleep fragmentation have been postulated (10, 11). In addition, the characteristics of morning headache have not been very clearly described. There are only scant data evaluating the characteristics of morning headache in OSAS that reported non-specific features (12, 13).
As there is controversy regarding the association of morning headache and OSAS as well as the prevalance and characteristics of headache, we aimed to investigate morning headache prevalance and characteristics in consecutive PSG-confirmed OSAS patients. We also analysed the improvement of headache in response to nasal continuous positive airway pressure (n-CPAP) treatment in order to prove that morning headache is caused by OSAS.
Patients and methods
Subjects referred to the Cerrahpasa Medical School, Department of Neurology, Sleep Disorders Centre between December 2005 and May 2007 with the complaint of snoring and/or respiratory problems during sleep were included in the study. All subjects had undergone clinical and PSG evaluation.
Clinical evaluation
Headache diagnosis was based on the criteria of International Classification of Headache Disorders. The primary criterion was the presence of headache upon awakening and improvement of headache within hours after awakening. We use the term morning headache instead of sleep apnoea headache because the criterion ‘disappearance of headache within 72 h after n-CPAP treatment’ was not always met. Subjects were interviewed regarding sleep-related complaints, depression, subjective daytime sleepiness and morning headache.
Morning headache was assessed using a headache questionnaire. The questions included presence of morning headache and primary headache history. If morning headache existed, localization (frontal, bilateral, occipital, generalized, half-sided), quality (pressing, throbbing, stabbing), duration (< 1 h, 1–4 h, > 4 h), frequency (≤ 1/month, 1–2/week, 2/week to 15/month, > 15/month), severity (mild, moderate, severe), accompanying features (nausea, vomiting, photophobia, phonophobia), analgesic use and effect on daily living activities were determined. The headache questionnaire also included the presence and characteristics of primary headache syndromes classified according to the International Headache Society (IHS) criteria. All patients also underwent an interview by two neurologists (B.G. and A.G.), and questionnaires were controlled in order to exclude incomplete or invalid data. Patients with OSAS who described morning headache and were treated with n-CPAP underwent second, third and forth interviews for the presence of headache at 1 day, 1 week and 1 month of treatment.
The Hamilton Depression Scale (HDS) was used in order to evaluate the presence of depression that may cause morning headache. Subjects with HDS scores of > 8 were excluded from the study to prevent bias originating from morning headache and depression. As we aimed to evaluate morning headache in OSAS, we excluded all the other primary sleep disorders in subjects. Only subjects who were referred to the sleep laboratory and did not fullfil the diagnostic criteria of any other sleep disorder according to the International Classification of Sleep Disorders (ICSD) were included in control group.
Polysomnographic evaluation
Polysomnographic evaluation of a minimum of 8 h was performed on Embla A 10 (Flaga, Reyjavick, Iceland) and Somnostar Alpha (Sensormedics, Yorba Linda, CA, USA) sleep systems. The following variables were monitored: 2 EEG (C3/A2-C4/A1 according to the 10–20 international electrode placement system), right and left electro-oculogram, chin electromyogram and electrocardiogram. Airflow was monitored by nasal pressure cannula. Respiratory movements were assessed by thoracic and abdominal strain gauges. Snoring was evaluated with neck microphone. Oxygen saturation during sleep was measured continuously using pulse oxymetry. Leg movements were recorded by left and right tibial electromyograms. PSG recordings were scored according to the standard criteria of Rechtschaffen and Kales (14) as an epoch of 30 s. Sleep-related respiratory disorders were diagnosed according to the criteria of the ICSD (15). Apnoea is defined as the cessation of airflow for 10 s, hypnoea as a decrease in the amplitude of a validated measure of breathing > 50% of normal and associated oxygen desaturation ≥ 4%. Obstructive apnoeas and hypnoeas are typically distinguished from central events by the detection of inspiratory efforts during the event. The apnoea–hypnoea index (AHI) was calculated as the number of apnoeas and hypnoeas per hour of sleep. Sleep apnoea syndrome was determined by using four AHI cut-points (AHI < 5, AHI 5 to < 15, AHI 15 to < 30 and AHI ≥ 30) and subjects were divided into four groups based on the PSG evaluation. Subjects with AHI < 5 were accepted as the control group. Remaining patients were classified as mild (AHI 5 to < 15), moderate (AHI 15 to < 30) and severe OSAS (AHI ≥ 30) according to AHI.
The other evaluated PSG parameters were total sleep time, sleep efficiency index, duration of non-rapid eye movement (NREM) 1, NREM 2, NREM 3+4 and rapid eye movement (REM) sleep stages [as % of total sleep time (TST)], oxygen saturation (sO2) nadir in REM and NREM sleep, mean oxygen saturation (sO2) during TST. Polysomnographic evaluation was performed by four neurologists who were blinded for the subjects.
This study was approved by the local ethics committee.
Statistical analysis
Data analysis was performed using the
Results
Of 810 patients, 563 consecutive subjects without any other sleep disorder other than snoring or OSAS or psychiatric disease who were investigated with PSG for reasons of sleep disorders such as OSAS and periodic limb movements were included in the study. Ages ranged between 22 and 84 years. PSG evaluation revealed that there were 101 subjects with AHI < 5 who enrolled in the control group. The mean age of the control group was 47.2 ± 11.9 years, with M/F ratio of 69/32. Four hundred and sixty-two patients were diagnosed as OSAS with an AHI ≥ 5. The mean age of the whole OSAS group was 50.9 ± 11.4 years and M/F ratio was 347/115. Morning headache was reported by only nine (8.9%) subjects in the control group compared with 156 (33.6%) of OSAS patients (P = 0.000) (Table 1).
Percentage of morning headache in control and obstructive sleep apnoea syndrome (OSAS) groups

P significance
∗< 0.005;
∗∗< 0.001.
The demographic characteristics and the presence of morning headache of all groups of OSAS patients and control subjects are shown in Table 2. Nearly half of the patients (n = 223, 48.5%) were diagnosed as severe OSAS with AHI ≥ 30. Morning headache was reported significantly more frequently in severe and moderate OSAS groups (38.4% and 36.8%, respectively), whereas 22% of patients with mild OSAS and only 8.9% of control subjects had morning headache (P = 0.000). χ2 test revealed that all groups differed significantly as regards the presence of morning headache, in which severe and moderate OSAS groups had significantly higher morning headache compared with mild OSAS patients and control subjects.
Distribution of morning headache, age and sex according to severity of obstructive sleep apnoea syndrome

P significance
∗< 0.001;
∗∗< 0.05.
AHI, apnoea–hypnoea index.
There were 347 male and 115 female patients among the total OSAS patients. The mean AHI was higher in male patients. One hundred and seventy-eight male patients were diagnosed as severe OSAS, whereas only 45 female patients had severe OSAS (P = 0.034). The male : female ratio was lower in OSAS patients with headache (P < 0.001). Primary headache history, both migraine and tension-type headaches, were more frequent in OSAS patients with morning headache (P = 0.000) (Table 3).
Comparison of gender and primary headache history in obstructive sleep apnoea syndrome (OSAS) groups with and without morning headache
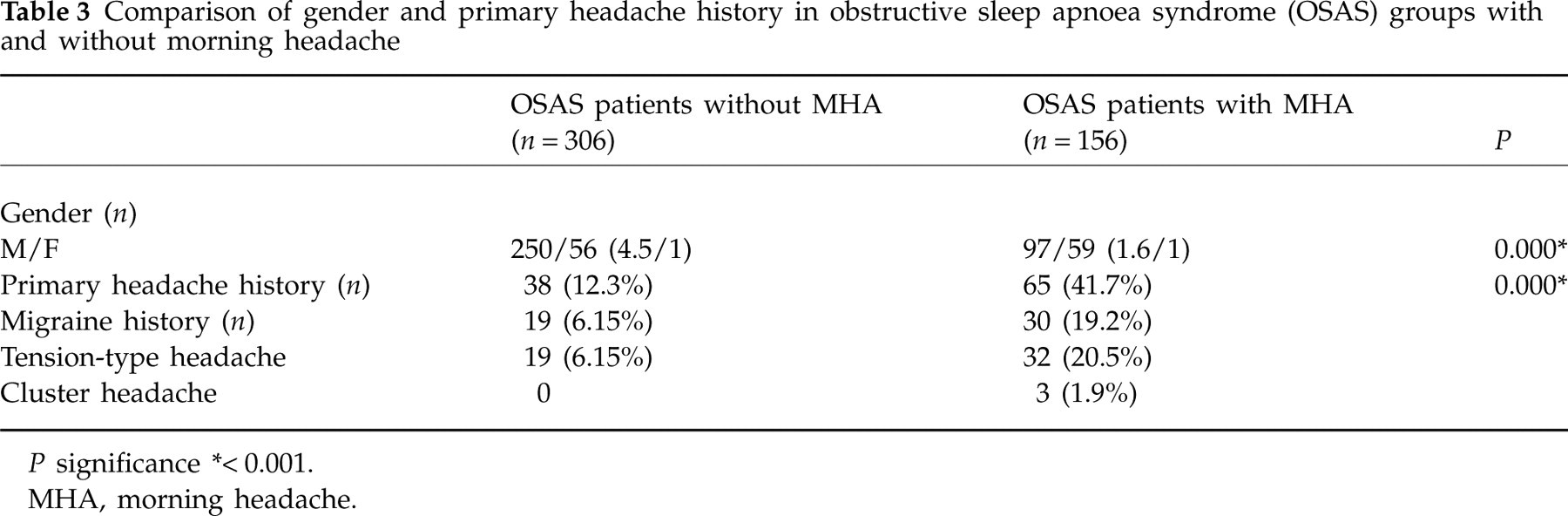
P significance
∗< 0.001.
MHA, morning headache.
Comparison of OSAS patients with and without morning headaches revealed that AHI was significantly higher in patients with morning headaches compared with those without morning headaches (38.7 ± 25.7 vs. 34.1 ± 24.6, P = 0.030). Oxygen saturation nadir during REM and NREM sleep as well as mean oxygen saturation value during total sleep time were also found to be significantly lower in the morning headache group (Table 4). The other PSG variables did not show significant differences between patients with and without morning headache.
Respiratory parameters of obstructive sleep apnoea syndrome (OSAS) patients with and without morning headache
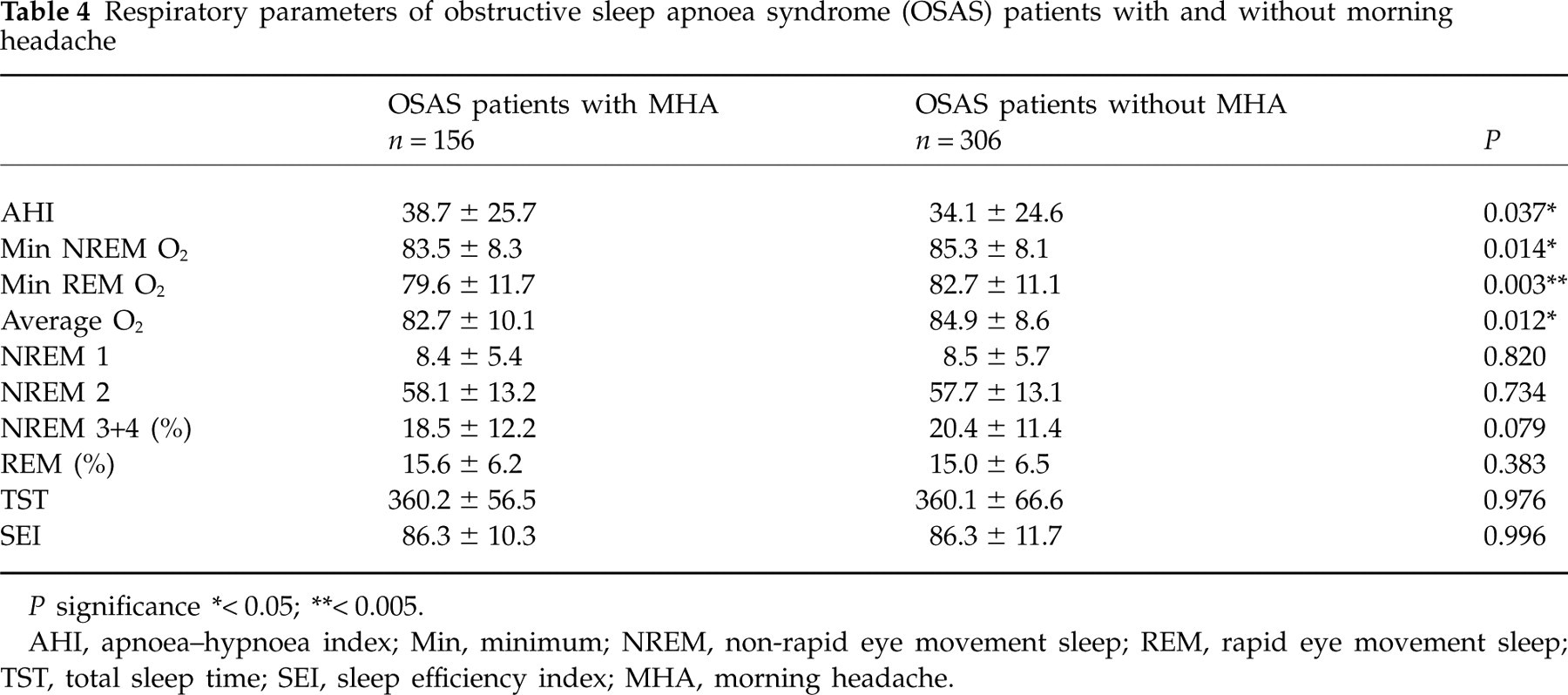
P significance
∗< 0.05;
∗∗< 0.005.
AHI, apnoea–hypnoea index; Min, minimum; NREM, non-rapid eye movement sleep; REM, rapid eye movement sleep; TST, total sleep time; SEI, sleep efficiency index; MHA, morning headache.
Table 5 shows the independent predictors of morning headache in OSAS patients. The following variables were analysed by logistic regression for prediction of morning headache: age, disease duration, AHI, sleep efficiency index, NREM min sO2, REM min sO2, mean sO2, NREM 3+4 period and REM period. None of the variables was found to be significantly associated with morning headaches.
Evaluation of determinative factors in obstructive sleep apnoea syndrome patients with morning headache

AHI, apnoea–hypnoea index; SEI, sleep efficiency index; NREM, non-rapid eye movement sleep; REM, rapid eye movement sleep.
Table 6 represents the characteristics of morning headaches in OSAS patients and comparison of headache characteristics in the total OSAS group and controls. Regarding localization, headaches were predominantly located generalized or frontal. It was pressing in quality in 66.5% of patients, throbbing in 19.4% and stabbing in 14.1%. The duration was 1–4 h in 37.5% and > 4 h in 35.8 % of patients. The severity was reported as moderate in 49.7% of patients and mild in 28.3%. Sixty per cent of patients required analgesics at least three times a week. Daily activity was influenced in 65.3% of patients with morning headaches. Morning headaches repeated nine to 15 times a month in 34.9% of patients and > 15 times a month in 26.3% of patients. None of the patients reported accompanying features with morning headache. Comparison of headache characteristics among mild, moderate and severe OSAS patients showed no significant differences. Headache characteristics such as localization, duration, frequency and severity in controls showed some differences from the OSAS patients.
Characteristics of morning headache in all obstructive sleep apnoea syndrome (OSAS) patients and control group
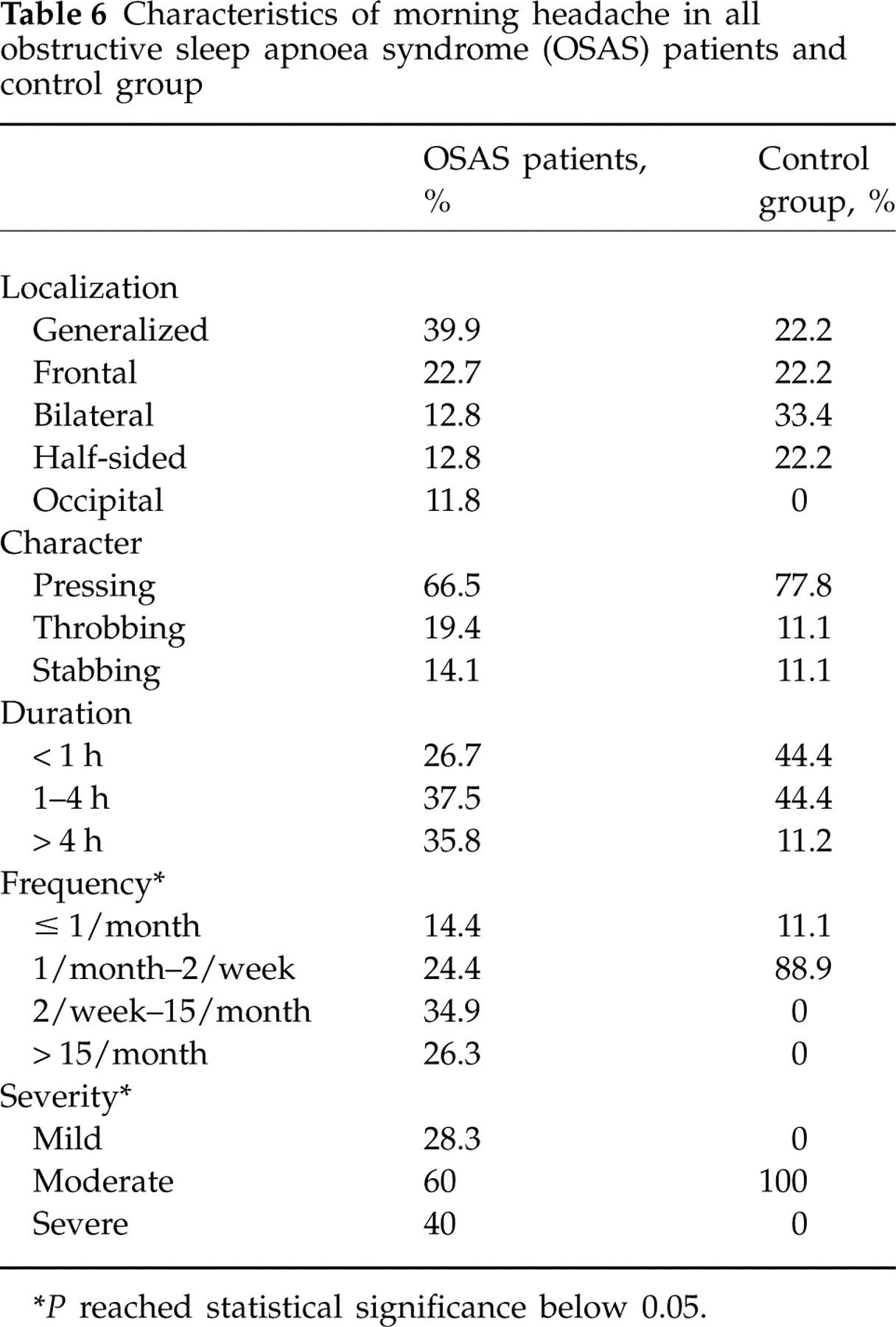
∗ P reached statistical significance below 0.05.
Of 156 patients with morning headache, 76 were treated with n-CPAP. At day 1 and week 1 of treatment, morning headache had totally disappeared in 55 (72.4%) and 64 (84.2%) patients, respectively. At the end of 1 month's treatment, morning headache was absent in 70 (92.1%) patients. Characteristics of morning headache in treated patients were similar to patients in the total group of OSAS patients with morning headache (Table 7). Four patients could not tolerate n-CPAP or failed to use it.
Characteristics of morning headache in obstructive sleep apnoea syndrome (OSAS) patients who received and did not receive treatment

P > 0.05 for all parameters.
Discussion
The main finding of our study was the demostration of significantly more prevalent morning headache in a large number of PSG-confirmed OSAS patients than in control subjects. Frequency of morning headache was found to be 33.6% of OSAS patients, whereas it was reported by only 8.9% of controls.
Few studies have evaluated the relationship between morning headache and severity of OSAS. Loh et al. (5) showed that occurrence and severity of morning headache were correlated with OSAS severity, whereas Olson et al. (10) did not show any clear association between occurrence of headache and OSAS severity or other PSG variables. AHI was reported to be higher in OSAS patients with headache, and patients with severe OSAS were more likely to have headache on awakening compared with mild OSAS (16). Our data revealed that there was a dose relationship between morning headache and severity of OSAS. We found that the prevalence of morning headache was 22% in mild OSAS, 36.4% in moderate OSAS and 38.2% in severe OSAS. These results show that the prevalence of morning headache increases with increasing OSAS severity.
Headache is generally known to be more common in women. Morning headache was also shown to be more frequent in female patients with OSAS compared with male patients (17). Our results are consistent with these findings, in that in spite of a higher number of male patients with more severe disease, morning headache was predominantly reported by female OSAS patients.
This study was not designed to determine the mechanisms of morning headache in OSAS, but our data provided some insights into the increased prevalance of morning headache among AHI categories in these individuals. Several possible mechanisms, including hypoxaemia, have been reported by which OSAS causes morning headache. Logistic regression analysis did not reveal any determinant factor in morning headaches in our study. On the other hand, our findings are consistent with a pathophysiological role of hypoxaemia in the mechanisms of morning headache. Patients with morning headache had a significantly lower oxygen saturation nadir during REM and NREM sleep with lower mean oxygen saturation value during total sleep time. It has also been suggested that morning headache in OSAS results from sleep fragmentation and architectural distruption of night sleep (11). Greenough et al. (17) showed that headache patients spent a shorter percentage of time in REM sleep. In another study, percentage of REM sleep was shown to be decreased in OSAS patients with headache complaints (17). Other reports have also suggested that disturbances in sleep architecture are not related to morning headache (12, 18). Our findings are consistent with these studies, in that neither sleep efficiency nor percentage of REM and NREM sleep showed significant differences between patients with and without morning headache.
In the literature, morning headache is reported predominantly as tension type, frontally located, pressing-tightening in quality, mild and < 30 min in duration (2, 5, 16). Our data support these findings, with predominantly generalized or frontal localization and pressing quality. On the other hand, we observed that morning headache in OSAS may be longer and rarer, as headache duration of 1–4 h and frequency of 2/week to 15/month were mostly reported, which is not typical of the criteria of IHS. As regards the severity, the majority of our patients reported that their headache was moderately severe with a requirement for frequent analgesics.
It has been shown that treatment of OSAS with either uvulopalatoplasty or n-CPAP results in improvement of morning headache (12, 19). Treatment with n-CPAP revealed the disappearence of morning headache in 72.4, 84.2 and 92.1% of our patients on the first day, first week and at 1 month of treatment, respectively. Recently, Mitsikostas et al. (20) showed poor response of headache to n-CPAP treatment. In this study, patients with chronic headache that may develop at any time of day and not only upon awakening were evaluated. So the poor response to n-CPAP in this study may be attributed to the effect of n-CPAP, which may be expected only in patients having headache upon awakening. It should be emphasized that the relief of morning headache with n-CPAP treatment in our study may be attributed to placebo effect; however, there is no placebo control study evaluating n-CPAP treatment on morning headache in OSAS. Furthermore, the relief of morning headache with n-CPAP is one of the main diagnostic criteria of sleep apnoea headache.
In summary, based on our findings we conclude that prevalence of morning headache increases with increasing OSAS severity. Although the exact cause–effect relationship between OSAS and morning headache remains unclear, hypoxaemia and female gender may influence the occurrence of morning headache. OSAS should be kept in mind in the presence of morning headache and, if needed, PSG should be carried out. The effectiveness of n-CPAP treatment in OSAS patients with morning headache was clearly demonstrated.