
Abstract
Introduction: Many migraine patients report cognitive complaints during the first hours or days following a migraine attack. The aim of this study was to assess whether and which cognitive (perceptual, attentional, or memory) processes are impaired during the first 48 hours after a migraine attack.
Methods: Three different cognitive tasks (global-local task, the attentional network task, and N-back task) were administered to 16 migraine patients (13 migraine without aura; mean age 58 years, 15 female) and 18 controls (59 years, 15 female), matched on age, gender, and educational level. Tasks were administered at three time points; during the first headache free day following a migraine attack (first session), 24 hours later (second session), and 12 days after the attack (third session).
Results: The attentional network and N-back tasks showed no significant differences between migraineurs and controls. In the global-local task, controls showed faster reaction times to global than to local stimuli, which is the standard global-precedence effect. This effect was absent in the migraineurs in all three sessions, especially if they used prophylaxis.
Conclusion: Migraineurs had no impaired attentional or working-memory functioning in the 2 days after an attack. They did show impairments in the processing of global visual features compared with controls, both between and immediately after an attack.
Introduction
Many migraine patients report mild cognitive complaints, such as slowing of reaction and memory problems, during both the ictal- and the post-ictal phase (1,2). Studies comparing cognitive functioning of migraine patients in the inter-ictal phase with controls are abundant but showed inconsistent findings. Some studies reported inter-ictal cognitive deficits in the domains of psychomotor speed (1,3), executive function (4), language (5), visual processing (6), attention (2,3), and memory (2,7), while other studies demonstrated no differences in cognitive functioning between migraineurs and controls (8−10).
However studies of specific after-effects of a migraine attack on cognitive functioning are scarce. One study investigating after-effects of a migraine attack failed to find differences in cognitive function, even though patients did report subjective impairments (2). However, there is some evidence for post-ictal physiological alterations, like altered regional cerebral bloodflow (11) and reduced alpha activity in the electroencephalograph (12), which might suggest temporary cognitive deficits. The available findings suggest a number of candidate processes but a systematic model of the impact of migraine on human information processing is lacking. Therefore, we chose a number of theoretically motivated, well-understood cognitive tasks that investigated the complete process from perception and attention to working memory.
The aim of the present study was to identify specific cognitive processes (perceptual, attentional, or memory) that might be impaired by migraine attacks during the first 48 hours after the attack, as compared to an inter-ictal baseline.
Methods
Participants
Sixteen migraine patients diagnosed according to the International Headache Society (ICHD) II criteria (13) were recruited from the neurology headache outpatient clinic databases of the Leiden University Medical Center, Leiden, the Netherlands. Eighteen healthy controls were matched on age, gender, and educational level. Controls without a history of headache attacks were recruited among relatives of investigators and patients. Excluded were subjects who were: suffering from depression, illiterate, had a history of stroke or other brain injuries, or had more than 10 migraine days per month. Approval for the study was obtained from the local medical ethics committee of the Leiden University Medical Center; all participants provided informed consent.
Design
If patients agreed to participate, they were instructed to contact the study coordinator at the end of a migraine attack on the first headache-free morning after a migraine attack. It was required that patients were headache-free, had had a good night sleep, and did not use attack medication during the last night to ensure testing was not influenced by pain, tiredness, or medication effects. Patients were then visited at home the same day to obtain the cognitive tests during the first session. The cognitive tests were repeated 24 hours later (second session) and 12 days post attack (third session). Within each participant the second and third session were on the same hour of the day as the first session. If a new migraine attack had occurred in between sessions 2 and 3, the third session had to be at least 3 days after the new attack. Session 3 was not allowed to take place during the prodromal phase of a following attack. To limit the time between the baseline and two post-attack sessions, a design was chosen in which the first test session was always the first day after the attack and, consequently, the second and third session were also in a fixed order. To control for any learning effect as a result of this repeated testing, control participants without migraine history were tested with the same protocols on three sessions with the same time intervals in between. Participants were tested by four specially trained students. All participants received the same instructions. Participants were tested by the same student during all three sessions. Participants were seated in front of a laptop monitor (Dell Latitude D-600, screen size 14.1 inch, resolution 1024 × 768, luminance 99.1 cd/m2, 85 Hz) and performed all tests under the same quiet circumstances. Participants were instructed to keep caffeine or nicotine use before the second and the third session at the same level as before the first session, so that the intra-individual consumption was likely to be constant over the three sessions. Before cognitive testing started, questionnaire data were obtained on general migraine characteristics, preceding migraine attack characteristics, general history, and medication use. Instructions for each test were according to protocol: they were read aloud by the investigator and were also shown on the computer monitor.
Neuropsychological testing
The tasks were constructed with E-prime software. The three following computerized different tests were administered during a 60-minute session at three different time points.
Perceptual organization (global-local) task
Perceptual organization capabilities were assessed by means of a global-local task (14). Participants were presented with hierarchically organized visual figures, in which a larger (global) letter was composed of smaller (local) letters. Letters used were H, S, and O. Stimuli could be congruent (if the local letters were identical to the global letter), incongruent (if the local letter and the global letter were different), or neutral (if a large or small O was presented).
Before the presentation of each stimulus, the participant was instructed to identify the global letter or the local letter, which always was an H or an S, and to press the respective response key on the keyboard. The letter at the to-be-ignored level could be an H, S, or O. This resulted in a total of 12 different letter combinations, which could be categorized in terms of global vs. local level (of the relevant stimulus) and congruent vs. incongruent vs. neutral relationship between the stimulus at the relevant level, and the stimulus at the irrelevant level.
One session consisted of 10 mini-blocks of 12 stimuli, presented in random order each. The visual instruction to respond to the local or global letter was presented for 2000 ms, followed by a 1000 ms blank screen and the stimulus, which was presented for 8000 ms or until a response was being made. Each stimulus measured 2 × 4 cm and was seen from a distance of about 60 cm. Each global letter consisted of 44 local letters. Reaction time and the accuracy of responses were recorded, with reaction times for correct responses being the main dependent variable.
Attention task (ANT)
The Attentional Network Task developed by Fan and colleagues (15) assesses three separable attentional functions (and, presumably, the underlying neural networks): alertness, orienting, and executive control of attention. The task is a combination of a flanker task (16) and a spatial cueing task (17). In each trial, participants are facing a visual cue followed by a visual target stimulus, which they respond to by pressing a left or right keyboard button.
The target stimulus consists of a horizontal row of five symbols, and participants are to respond to the central symbol, which is an arrowhead pointing to the left or right (calling for a left or right button press, respectively). The central arrow is flanked by four irrelevant symbols, two on either side. These flankers can be either congruent (arrowheads pointing into the same direction as the target, e.g. > > > > >), incongruent (arrowheads pointing into the opposite direction, e.g. < < > < <), or neutral (e.g. − − > − −). The row of symbols randomly appears at the top or bottom of the screen and it may or may not be preceded by a cue informing about target location. In particular, there are four cue conditions: the no-cue condition, where the cue is omitted, the centre-cue condition, in which an asterisk appears at the centre of the screen, the double-cue condition, where two asterisks appear at the centre of the possible target-stimulus locations, and the spatial-cue condition, where just one asterisk appears at the location where the target stimulus will be appearing.
The combinations of the three flanker conditions and four cue conditions provide the data base for calculating three indices of theoretical relevance (alertness, orientation, and executive control) (15).
Each trial would begin with the presentation of a cue, except in the no-cue condition, for 100 ms. After a blank interval of 400 ms, the target was presented for 1700 ms or until a response was being made. Three blocks of 96 randomly determined trials were presented. Target and flankers were presented in black on a white background. Each symbol measured about 5 × 7 mm, seen from a distance of about 60 cm. Before each session, a 2-minute training block was included in the protocol. Reaction time and accuracy were recorded, the primary dependent variable being reaction time for correct responses.
Working memory (N-back) task
The N-back task requires the monitoring, updating, and manipulation of remembered information and places great demands on working memory. The participant is required to monitor a series of letters shown on the screen and to respond whenever a stimulus appears that is the same as the one presented in trials before. In our study the n was 0, 1, 2, or 3. The 0-back condition served as a kind of control or baseline condition, the target letter was the letter ‘X’ and participants were to respond to any ‘X’ they would see by pressing the space bar of the computer keyboard. In the three remaining conditions, the target letter was defined as any letter that was identical to the one presented in the preceding trial (1-back, that is), two trials before (2-back), or three trials before (3-back).
There was a block for each of the four levels. Each block consisted of 60 stimuli of which 12 were target stimuli, that is, the probability of a target stimulus was 20%. Letters appeared in black on a white background, measured 3 × 3 cm and were seen from a distance of about 60 cm. Each letter was shown for 1000 ms, followed by 1000 ms blank. Reaction time to target letters and percentage of correct responses were recorded, with accuracy being the main dependent variable.
Patient characteristics
During a face-to-face interview, migraine characteristics were evaluated for the preceding attack as well as migraine history and general health. The visual analogue scale was used by participants to report the pain experienced during the preceding attack, with a value of 0 implying no pain and a value of 10 implying agonizing pain. Furthermore, preceding migraine severity was assessed by a 4-point scale; no pain, mild pain, moderate pain, or severe pain. Educational level was dichotomized to low (primary school) vs. higher.
Statistical analysis
Baseline characteristics were analysed using t-tests for continuous variables and chi-squared/Fisher exact tests for dichotomous variables. Reaction time and percentage correct for all computerized tasks were analysed using analysis of variance (ANOVA) for repeated measurements. For the omnibus analysis of the global-local task, a 3 × 2 × 2 × 2 ANOVA was used with session (3), level (global/local, 2), and congruence (2) as within-subject factors and group (migraine vs. control) as between-subject factor. The paired sample t-test was used for comparing the global-local effect in each group. For the omnibus analysis of each of the three indicators of the ANT, 3 × 2 × 2 ANOVAs were used with session (3) and condition (2) as within-subjects factors and group (migraine vs. control) as between-subjects factor. For the omnibus analysis of the N-back task a 3 × 4 × 2 design was used with session (3) and level (4: 0, 1, 2, or 3) as within-subjects factors and group (migraine vs. control) as between-subject factor. t-tests were used for more detailed comparisons. The significance level was set to p = 0.05 for all statistical tests.
Results
Characteristics of participants

Values are n (%) or mean ± standard deviation. NA, not applicable.
Characteristics of preceding migraine attack

Values are n (%) or mean ± standard deviation.
Perceptual organization (global-local) task
Mean reaction times for the global-local task are shown in Table 3. Reaction times decreased with each session in both migraineurs and controls [F(2,27) = 16.94, p < 0.0001] and congruence between the letters at the two levels (global and local) yielded faster responses than incongruence [F(1,28) = 81.56, p < 0.0001]. Neither Migraine group vs. controls nor global vs. local produced a main effect [F(1,28) < 1]. There was a migraine vs. controls-by-global vs. local interaction [F(1,28)4.99, p = 0.034]. The source of this interaction is shown in Figure 1: controls showed faster reaction time when responding to global than to local stimuli [t(1,15) = 3.86, p = 0.035 (one-tailed)], a replication of the standard global-precedence effect (14). Migraineurs actually showed a trend towards the opposite pattern with longer reaction times to global than to local stimuli, but this difference did not reach significance (p = 0.12). In other words, the standard global-precedence effect was eliminated in migraine patients. Even though the figure suggests a modulation by session, there was no three-way interaction (p = 0.26) of global vs. local, migraine vs. controls, and session, suggesting that the difference between migraineurs and controls was statistically comparable across sessions. Interestingly, the interaction of group and level approached significance if only the prophylaxis-using migraineurs were considered (p = 0.055) but was far from significance if non-prophylaxis users were compared with controls (p = 0.2).
Plot of reaction time for the perceptual organization task for migraine patients and healthy controls. Global-local reaction time (ms) according to condition Values are mean ± standard error of the mean. Reaction time for correct responses is shown. Total, mean reaction time over all conditions (global or local level and congruent or incongruent).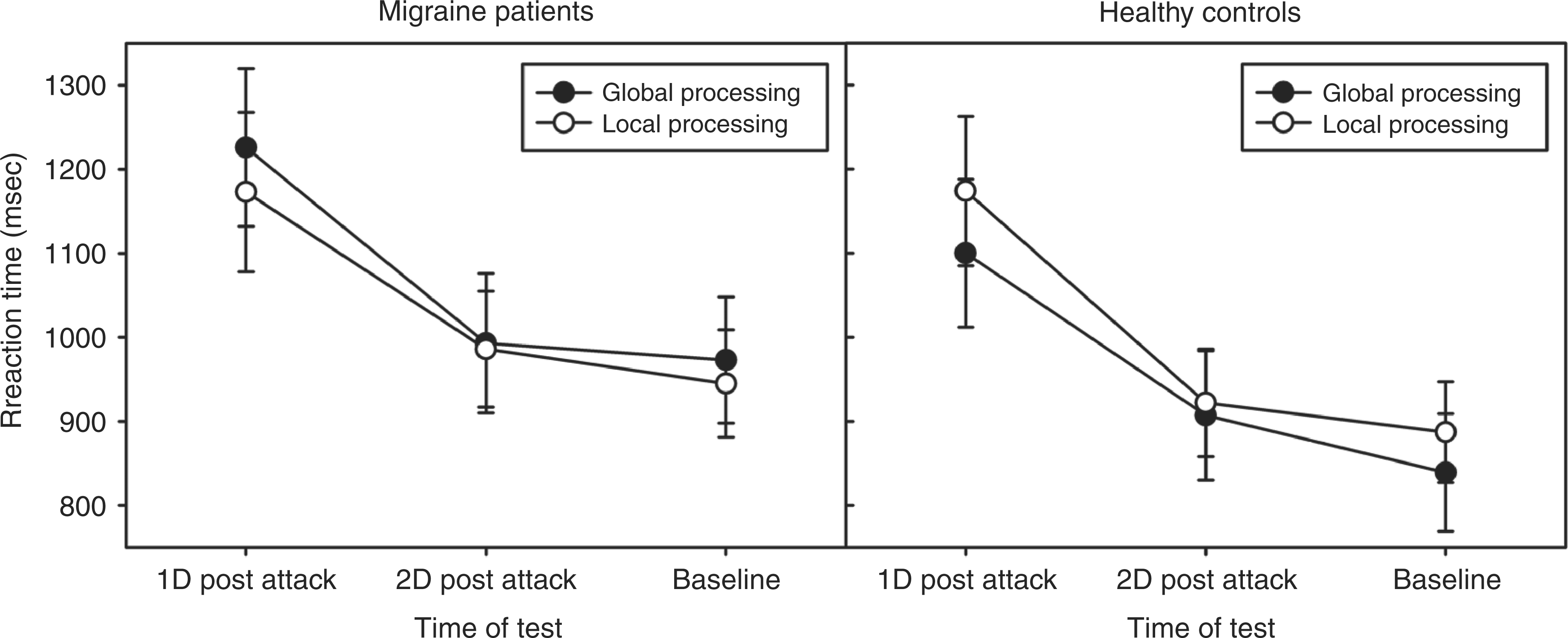

The one participant not using triptans did not perform differently compared to triptan users on the global-local test.
Attention task (ANT)
Alerting
Main effects of session [F(2,58) = 15.21, p < 0.0001] and warning cue (present/not present) [F(1,29) = 53.99, p < 0.0001] indicated that reaction time decreased over sessions and was faster with an alerting cue. Thus the standard alerting effect was replicated (18). However, no significant effect was found for group [F(1,29) < 1] or any interaction involving group [F(1,29 < 1]. The ANOVA of the error rates yielded no reliable effect, only a trend towards a group-by-cue interaction showing that migraineurs had a higher percentage of correct responses [F(1,32) = 3.55, p = 0.069].
Orienting
Main effects of session [F(2,58) = 20.6, p < 0.0001] and warning cue (spatial vs. neutral) [F(1,29) = 291.2, p < 0.0001] indicated that reaction time decreased over sessions and was faster with spatial than with neutral cues. That is, the standard benefit of spatial orienting was replicated (17). However, no significant effect was observed for the group variable [F(1,29) < 1] or any interaction involving it. There was an advantage of spatial over neutral cues in both groups in the error-rate analysis [F(1,32) = 9.88, p = 0.004].
Executive control
ANT reaction time (ms) according to flanker type

Values are mean ± standard error of the mean.
Working memory (N-back) task
N-back reaction time (ms) according to n-level

Values are mean ± standard error of the mean.
Discussion
Migraineurs often complain about cognitive impairment shortly after a migraine attack. Studies showed evidence of profound post-ictal effects on cognitive tests after epileptic attacks, however this has not been demonstrated after migraine attacks. The aim of this study was to assess the degree to which a recent migraine attack affects cognitive functions at different processing levels. We tested migraineurs in various, theoretically motivated experimental tasks at three points in time post-ictally and compared their performance with healthy controls. Three results of this study are particularly noteworthy.
First, we did not find evidence for any reliable changes in cognitive performance during the post-attack phase, as indicated by the absence of any interaction between session, group, and cognitive measures. In other words, no temporal negative effect on cognitive function after the attack was found. This observation is in line with the one previous study reporting no negative influence during the post-ictal phase of a migraine attack (2). However, while Mulder et al. (2) tested participants who still had mild headache during testing, we defined the post-ictal phase by the absence of headache. Moreover, while Mulder et al. (2) recruited their participants from a student population, we recruited migraine patients from the outpatient headache, which resulted in a higher mean age.
Second, reliable and stable differences between migraine patients and controls were observed with respect to the organization of local and global visual stimuli. The controls showed the standard global precedence effect (14) with better performance on global than on local stimulus features (trend). Interestingly, this standard global precedence effect was not present in migraineurs. The fact that this difficulty did not change across sessions suggests that it is not caused by, or associated with, the migraine attack per se but, rather, seems to be associated with the (enduring) migraine disposition.
Third, none of the remaining measures (N-back, ANT) showed any hint of an interaction with group (migraineurs vs. controls). Even though null effects need to be interpreted with the necessary caution, it is important to point out that the tasks as such worked very well ⊟ i.e., we were able to replicate all the standard effects ⊟ and yet we found no association between migraine and alerting, orientation, executive control, and working memory measures. Thus, even though more systematic research on this issue is required, we tentatively conclude that alerting, orientation, executive control, and working memory do not play a role in, and do not seem to be impaired by, migraine. This leaves the global-local task, investigating organization of local and global visual stimuli, as the test differing between migraineurs and controls, a finding which is consistent with the previous observation that migraineurs have higher perceptual thresholds for the recognition of global shape (20).
The global-local task was developed by Navon (14) and taps into the organization of visual information into coherent objects or Gestalts and assesses this performance by presenting participants with hierarchically organized visual stimuli, such as a global letter that is made of a number of local letters. Healthy humans have a strong preference to perceive the global letter first and faster, suggesting that they organize the local information into a coherent global whole ⊟ the so-called global precedence effect (14). The first evidence for specific dysfunction in migraineurs comes from two recent studies (20,21) showing that migraineurs did not differ from healthy controls in a visual task tapping into very early sensory processes (presumably performed by brain area V1) but have higher thresholds than controls for the perception of global shape (presumably performed by the extrastriate area V4). This suggests a locus in the cortical information-processing stream later than visual stages (V1) but earlier than at encoding into working memory, which implies higher visual areas that are either directly involved in feature integration or that provide integration processes with global information. As demonstrated by Badcock and colleagues (23), the global precedence effect can be eliminated by filtering out low-spatial frequency information in Navon-type stimuli. It is thus possible that in migraineurs the processing through low-spatial frequency tuned visual channels is impaired. This would fit with the observation that channels that prefer higher flicker rates (commonly tuned to lower spatial frequency ranges) can have lower sensitivity in migraineurs during their inter-ictal period (24). Hence, patients may not be able to process or to integrate more global features into perceptual representations of objects and events.
The organization of perceptual information is followed by attentional selection processes, in which no difference was found in our study between migraineurs and controls by ANT test. Human attention is thought to fall into a least three different abilities, which are handled by three neurally dissociable networks (15): alerting (activating the system in response to the presence of a relevant stimulus), orienting (selecting a particular stimulus or location for further processing), and executive control (biasing response selection towards appropriate responses). Not one of these abilities seems to be impaired by migraine.
The outcome of attentional selection processes are thought to be transferred to working memory, which organizes further processing or storage of the selected information. To assess the impact of migraine on working memory efficiency, we employed the well-established N-back task (for an overview, see Kane et al. (19)), which requires participants to hold information and continuously update this information based on new incoming stimuli. In this study, however, no difference in N-back task was found between migraineurs and controls.
Several caveats are in order and some limitations apply. It is possible that migraine-specific prophylaxis played a role in producing the observed elimination of the global-local effect in migraineurs. Various adverse effects of prophylaxis on cognition have been reported (22) and a direct effect of the prophylactic medication can be suggested. Migraine characteristics between prophylaxis users and non-users as age of migraine onset, total migraine years, current attack frequency, current attack duration, and current presence of photophobia or phonophopia did not differ. However this does not rule out that some clinical characteristics before the start of prophylaxis were in fact different (for example attack frequency) compared to the non-prophylaxis using group. The types of prophylaxes used by our participants were too heterogeneous to correct for their respective type-specific potential effects.
The absence of a post-attack effect could be explained by the high percentage of triptan users in our study, 94% of the participants used triptan during the attack preceding the tests. Possibly the use of triptans prevented the development of cognitive complaints, and differences would probably be easier to detect after untreated attacks. However, participants willing to skip their attack treatment will probably lead to the inclusion of less severely affected migraineurs. Another explanation for the absence of a post-attack effect is the long time which passed between the end of the attack and actual testing. However, testing sooner would invite possible artefacts, such as side effects of headache, mood, medication, and exhaustion. A fatigue score in each participant before each session was not obtained, and therefore adjusting for this possible important factor was not possible.
Another caveat relates to testing procedures. With regard to the fact that we tested participants repeatedly, it is important to point out that there were pronounced session effects, i.e. learning improved performance considerably. This underscores the need for a control group in studies investigating post-attack changes, as this permits the correction for learning effects, which might be particularly strong if participants are relatively old and not used to computerized testing. Even though the examiners were not blinded for diagnosis, all the relevant tests were computerized and the sequence of trials was fully randomized which should have prevented systematic biases.
Moreover, recruiting patients for tests on cognitive functioning might bias the study towards patients with a higher education and, indeed, in our study the educational level was above average. Furthermore, migraineurs recognizing cognitive decline themselves (after an attack) might be more likely to participate in a study focusing on (post-attack) cognitive effects.
Finally, due to the rather high demands posed by our experimental protocol and the relatively selective recruiting procedure, only a limited number of patients could be tested. In addition, the requirement to match the members of the control group to the patients created a sample that was considerably more heterogeneous than the student samples that have been used to develop the tasks we employed. All this is likely to have increased the error variance and made our statistical tests relatively conservative. Therefore, the absence of statistically significant effects, such as with the numerically reversed global precedence effect in migraineurs or the interaction between group and session, should be interpreted with caution. In any case, the strength of the present study is the design with matched controls that were tested within the same time intervals and the exclusion of effects of the actual headache phase by delaying post-ictal testing until the first headache free day. Future studies on post-ictal cognitive functioning should probably exclude prophylaxis users and consider starting testing somewhat sooner after the (untreated) attack. While in previous studies on cognitive function in migraineurs, specific differences were found between migraineurs with aura and migraineurs without aura, in future studies groups of both migraine with aura and without aura should be reasonable large to make comparisons between these groups.
In conclusion, no evidence for temporary changes in cognitive performance could be found during the post-ictal phase (on average 17 hours after the end of the attack) in migraineurs on attentional function, working memory, or perceptual organization capabilities using this study design. However we found that the normal global precedence was absent in migraineurs, specifically in prophylaxis users − a deficit that is likely to impair the processing of the visual context and Gestalts.
Footnotes
Acknowledgements
The authors are indebted to M Conijn, H Boden, K van der Meer, E Bernfeld, L Gerse, and J Graafland who helped including participants and collecting the data, for their impressive efforts and devotion to this project.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest
MF has, in the past 3 years, received grants and consultancy or industry support from Almirall, Coherex, Colucid, Eisai, GlaxoSmithKline, Linde, MAP, Medtronic, Menarini, Merck, Minster, Pfizer, and St Jude, and independent support from NWO, NIH, European Community FP6, Biomed EC, the Dutch Heart Foundation, NWO-Spinoza premium.