
Abstract
Background: There are no reports on the risk of stroke after trigeminal neuralgia (TN). The aim of this population-based follow-up study was to investigate whether the occurrence of TN is associated with a higher risk of developing stroke.
Methods: A total of 1453 people with at least three ambulatory visits in 2001 with the principal diagnosis of TN were enrolled in the TN cohort. The non-TN cohort consisted of 5812 age- and sex-matched, randomly sampled subjects without TN. The 2-year stroke-free survival rate between the two groups was compared using the Kaplan-Meier method. The Cox proportional hazards regression model was used to estimate the hazard ratio of stroke after adjustment for demographic and clinical covariates.
Results: In the TN cohort, 73 patients developed stroke during follow-up, while in the non-TN cohort, 157 subjects suffered a stroke. The crude hazard ratio of stroke for the subjects with TN was 1.86 (95% CI, 1.41–2.45; p < 0.0001). The adjusted hazard ratio was 1.76 (95% CI, 1.33–2.33; p < 0.0001) after adjusting for demographic characteristics and comorbid medical disorders.
Conclusion: This study showed a significantly increased risk of developing stroke after TN. Further studies are needed to investigate the underlying mechanism of this association.
Introduction
Trigeminal neuralgia (TN) is an uncommon disorder characterized by recurrent, paroxysmal lancinating pain within the distribution of the trigeminal nerve. The recurrent pain may be triggered by events such as talking, chewing, brushing teeth, or even a light touch to the face (1). The annual incidence of TN in population-based antecedent studies has been reported as 4 to 27 per 100,000 person year (2–5). TN mainly has an onset during middle or old age, but occasionally occurs in young adults (2,6). Most cases are classical TN, which lacks objective evidence of motor or sensory deficit and does not result from another disorder (1). A minority of cases are considered as symptomatic TN, which is caused by an underlying lesion, such as multiple sclerosis (1,3,7), a brain tumor (1,8), or a pontine infarct (9,10).
The exact pathophysiology of classical TN is unknown, but increasing evidence suggests that it may be related to compression of the trigeminal nerve entry zone by a tortuous vessel, which leads to demyelination and ephaptic transmission in the trigeminal nerve (1,7). It has been suggested that hypertension may be a risk factor for TN (2,3). In addition, classical TN has been reported to show signs of arterial tortuosity, which has been suggested to be associated with hypertension and increased hemodynamic stress in the cerebral vasculature (11–13). Therefore, it was of interest whether the occurrence of TN is linked to an increased risk of developing cerebrovascular disorders. However, to our knowledge, no population-based study has been carried out to investigate the temporal relationship between TN and stroke. The purpose of this population-based follow-up study was therefore to evaluate the risk of stroke after having TN.
Materials and Methods
Study Design and Subjects
We used a prospective age and sex-matched cohort design to study the effect of TN on the risk for stroke. The data used in this study were from the complete National Health Insurance (NHI) claim database in Taiwan from 2000 to 2003. This study included a TN cohort and a non-TN cohort, both of which were drawn from the Taiwanese residents who had at least one ambulatory visit recorded in the complete NHI claims database during 2001. Note that, in 2001, more than 21.6 million people were registered in the NHI, accounting for approximately 97% of the total population in Taiwan. This large-scale population-based NHI database provides a unique opportunity for investigating the risk of stroke in association with TN, which is an uncommon disorder. It should also be noted that the rationale for using the NHI database after 2000 is that, after 1 January 2000, NHI claims data were consistently encoded using the standardized International Classification of Disease, 9th Revision, Clinical Modification (ICD-9-CM) according to the regulations of the NHI Bureau. To keep individual information confidential in order to satisfy regulations on personal privacy in Taiwan, all personal identification numbers in the data were encrypted by converting the personal identification numbers into scrambled numbers before data processing under the auspices of the Department of Health.
The TN cohort consisted of subjects who had received a principal diagnosis of TN (ICD-9-CM code 350.1) in ambulatory medical care visits between 1 January 2001 and 31 December 2001. The index visit was defined as the first ambulatory visit during which the principal diagnosis of TN was made. Because the diagnosis of TN is usually made on a clinical basis, in order to maximize case ascertainment, only patients with at least three ambulatory visits (including the index visit) with the principal diagnosis of TN in this period were considered for inclusion in the TN cohort (n = 4137). The exclusion criteria for the recruitment of subjects into the TN cohort were: (1) younger than 18 years old (n = 15); (2) any previously diagnosed TN during the year 2000 (n = 2346) (to increase the likelihood of identifying only new incident TN cases); (3) a previous diagnosis of any type of stroke (ICD-9-CM codes 430–438) (n = 619) before the index ambulatory care visit; and (4) a diagnosis of multiple sclerosis (ICD-9-CM code 340, n = 17) or benign or malignant neoplasm of the nervous system (ICD-9-CM code 191, 192, 225, n = 273) before the index visit or within 2 years after the index visit (to increase the chance of identifying only patients with classical TN). The remaining 1453 patients formed the TN cohort for the subsequent analysis.
The non-TN cohort was constructed by sampling the subjects without a diagnosis of TN in the same 2001 NHI claim database. We assigned the first ambulatory visit during 2001 as the index visit. Subjects ever having a principal or secondary diagnosis of either TN or stroke before their index visit were excluded. We randomly sampled four people for each TN patient in the aforementioned TN cohort, matched by sex and age. A total of 5812 subjects were enrolled in the non-TN cohort.
Outcome and follow-up
We traced all the ambulatory medical care records and inpatient records for each subject from their index visit for a period of 2 years. To determine date and cause of death, the data were linked to a mortality database that included deaths registered up to 31 December 2003. We identified the date of the first principal diagnosis of stroke (ICD-9-CM codes 430–437) during the follow-up as the primary endpoint. The case ascertainment for stroke required ≥1 hospital discharge or ≥2 ambulatory medical care visits with a principal diagnosis of stroke. All cohort subjects were followed from the index visit to the first occurrence of stroke, death, or end of follow-up. We evaluated the effect of TN on the stroke-free survival, adjusting for demographic features, such as age and sex, and the cardiovascular comorbidities of hypertension (ICD-9-CM code 401–405), diabetes (ICD-9-CM code 250), hyperlipidemia (ICD-9-CM code 272), coronary heart disease (ICD-9-CM codes 410–414, and 429.2), chronic rheumatic heart disease (ICD-9-CM code 393–398), and other types of heart disease (ICD-9-CM code 420–429). Information on these preexisting comorbid medical disorders was obtained by tracing all the ambulatory medical care and inpatients records in the NHI database in the year before the index visit. The case ascertainment for these medical comorbidities was defined as ≥1 hospital discharge or ≥2 ambulatory visits with a relevant principal or secondary diagnosis code.
Statistical analysis
The chi-square test and Student’s t test were used to compare differences in demographic characteristics and comorbid medical disorders between the TN and non-TN cohorts. The stroke-free survival curves for the TN and non-TN cohort were compared using the Kaplan-Meier method with the log-rank test. Cox proportional hazard regression was used to estimate the effect of TN on occurrence of stroke after adjusting for demographic characteristics (age and sex) and medical comorbidities (diabetes, hypertension, hyperlipidemia, coronary heart disease, chronic rheumatic heart disease, and other forms of heart disease). A two-tailed alpha level of 0.05 was considered statistically significant for all analyses, which were performed using SAS 9.2 software (SAS Institute, Cary, NC, USA).
Results
Descriptive findings
Demographic and clinical characteristics of the trigeminal neuralgia (TN) cohort and the non-TN cohort

Values are expressed as the mean ± SD or n (%).
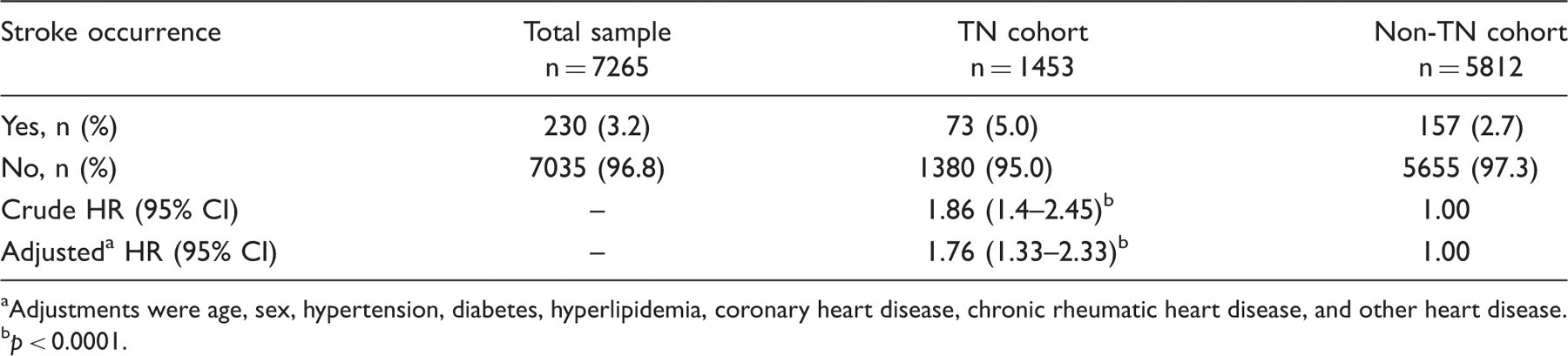
As shown in Table 2, 230 stroke events occurred in the total study sample (230/7265, 3.2%). Of the 1453 subjects with TN, 73 (5.0%) developed stroke during the 2-year follow-up, while 157 (2.7%) of the 5812 subjects in the non-TN cohort suffered a stroke. Comparison of the stroke-free survival curves showed that the stroke-free survival rate for the TN cohort was significantly lower than that for the non-TN cohort (p < 0.0001, Figure 1). The crude hazard ratio (HR) of stroke for the TN cohort compared with the non-TN cohort was 1.86 (95% CI, 1.41–2.45; p < 0.0001). The adjusted HR was 1.76 (95% CI, 1.33–2.33; p < 0.0001) after adjusting for age, sex, hypertension, diabetes, hyperlipidemia, coronary heart disease, chronic rheumatic heart disease, and other types of heart diseases.
Two-year stroke-free survival rate for the trigeminal neuralgia cohort and the non-trigeminal neuralgia cohort. Crude and adjusted hazard ratios (HR) of stroke during the 2-year follow-up for the trigeminal neuralgia (TN) cohort and non-TN cohort Adjustments were age, sex, hypertension, diabetes, hyperlipidemia, coronary heart disease, chronic rheumatic heart disease, and other heart disease.
p < 0.0001.
Crude and adjusted hazard ratios (HR) of stroke during the 2-year follow-up for the trigeminal neuralgia (TN) and non-TN cohorts, stratified by sex and age

The adjusted HR was calculated by adjusting for age, hypertension, diabetes, hyperlipidemia, coronary heart disease, chronic rheumatic heart disease, and other heart disease.
The adjusted HR was calculated by adjusting for sex, hypertension, diabetes, hyperlipidemia, coronary heart disease, chronic rheumatic heart disease, and other heart disease
p < 0.05.
p < 0.01.
p < 0.001.
We also compared the distribution of stroke subtypes in these two cohorts. In the TN cohort, 8 (11%), 39 (53%), and 26 (36%) patients had, respectively, hemorrhagic (ICD-9 code 430–432), ischemic (ICD-9 code 433–435), and other types of strokes (ICD-9 code 436, 437), while the corresponding figures for the non-TN cohort were 23 (15%), 91 (58%), and 43 (27%), with no significant difference in stroke subtype distribution between the TN and non-TN cohorts (p = 0.40).
Discussion
The major finding in our study is that TN was associated with a 1.8-fold increased risk of stroke. This association held even after controlling for common cerebrovascular risk factors. The 2-year stroke-free survival rate for the subjects with TN was significantly lower than that for the non-TN cohort. This is the first large-scale population-based follow-up study showing an increased risk of stroke after TN. The exact mechanism for the association between TN and stroke is unknown. We considered the following explanations.
First, previous studies have reported that hypertension is associated with a higher risk of TN (2,14), suggesting that hypertensive arteriosclerosis vascular changes might be a risk factor for developing TN (2,3). In the present study, we found that the TN cohort had a substantially higher prevalence of hypertension than the non-TN cohort, whereas there was no significant difference in the prevalence of diabetes. Although classical TN has been considered as an idiopathic disorder, evidence is increasing that it may be related to compression of the trigeminal nerve entry zone close to the brain stem by a tortuous vessel (7,15,16). Arterial tortuosity has been associated with hypertension (11–13,17) and may indicate hypertension-related vascular lesions of the brain (12). In addition, neurovascular compression at the ventrolateral medulla has been reported to be associated with central sympathetic activation and hypertension (18–20). We therefore postulated that the link between TN and stroke seen in our study may be mediated, at least in part, by an association between TN and hypertension-related vascular changes. It is possible that hypertension is a common risk factor for both TN and stroke, and the occurrence of TN may be a marker of increased risk of developing stroke.
Vascular tortuosity has been associated with aging and hypertension (13,17). Nevertheless, in the present study, TN remained an independent risk factor for stroke even after adjusting for hypertension and other common cerebrovascular risk factors. Moreover, in the stratified analysis (Table 3), the adjusted hazard ratio of stroke was similar in the younger (age <65 years) and older (≥65 years) groups. These findings suggest that the association between TN and stroke might be also due to mechanisms that are independent of hypertension- or age-related vascular changes. One possible explanation is that patients with TN usually suffer intense and unbearable pain that can occur spontaneously or be triggered by common daily activities, such as eating or talking. Such pain would lead to excessive anxiety and psychological distress, which have been reported to be associated with increased risk of coronary heart disease and stroke (21,22).
A unique strength of the present study is the use of a longitudinal population-based database, which enabled us to identify all incident cases of stroke and to establish a temporal relationship between TN and stroke. In addition, the sample size from these large-scale population-based data provided an adequate statistical power for evaluating uncommon disorders, such as TN. Nevertheless, there are some limitations to our study. First, the diagnosis of TN, stroke, and medical comorbidities in our study was entirely determined by the ICD codes taken from the NHI claim database. As with all administrative databases, one cannot be entirely sure about the accuracy of the data. However, the NHI Bureau randomly samples the claim data from every hospital and reviews charts on a regular basis to verify the diagnostic validity and quality of care. In addition, we also used a case ascertainment algorithm in the present study to maximize diagnostic accuracy. Second, owing to the inherent limitations of the original database, information was lacking about smoking, alcohol intake, body mass index, physical activity, or detailed values of biochemical factors, which may affect the risk estimation of stroke. Third, the follow-up time was only 2 years, which did not allow us to evaluate the long-term effect of TN on stroke.
In conclusion, the present population-based cohort study demonstrates a significantly increased risk of stroke after TN, suggesting that occurrence of TN may be a marker of increased stroke risk in the following years. Further studies are required to investigate the underlying mechanism for this association between TN and stroke.
Footnotes
Funding
This work was supported by Department of Health (DOH), Executive Yuan, Republic of China (grant numbers DOH93-TD-M-113-030, DOH94-TD-M-113-004, and DOH95-TD-M-113-002).
Conflict of Interest
None.
Acknowledgments
This study used the complete National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health. The conclusions in our study are not necessarily those of the Department of Health, Executive Yuan, Republic of China.